Article Text

Abstract
Background: Little is known about the airway pathology of wheezing disorders in infants and preschool children, partly owing to the difficulty of undertaking invasive studies in this age group. The safety of endobronchial biopsy and the quality of biopsies obtained were reviewed in infants and preschool children.
Methods: Case notes of children under five years of age who underwent bronchoscopy and endobronchial biopsy were reviewed. The safety of the procedure was compared in a control group matched for weight and age, undergoing bronchoscopy without endobronchial biopsy. A consultant histopathologist assessed biopsy quality.
Results: 33 patients (mean age 31 months, range 4 to 59) underwent bronchoscopy and endobronchial biopsy, and were matched with 33 controls (mean age 28 months, range 3 to 52). There was no significant difference between groups in the number, type, or severity of complications occurring during or after the procedure. Biopsies from 30 of the 33 subjects could be assessed. Reticular basement membrane was identified in all 30; inflammation could be assessed in 26; areas of smooth muscle were present in 23.
Conclusions: In a group of preschool children undergoing bronchoscopy under general anaesthetic, performance of endobronchial biopsy carried no extra risk. The quality of biopsies obtained was usually sufficient to allow an assessment of remodelling and inflammation.
- preschool child
- bronchoscopy
- biopsy
Statistics from Altmetric.com
Wheezing in infants and preschool children is common1 and can be severe, causing significant morbidity.2 The majority of children will grow out of their symptoms by school age,3 although a proportion will continue to wheeze in later childhood and be given a diagnosis of asthma.4 Despite the identification of certain risk factors—such as atopy and egg allergy—for the development of asthma in preschool children with wheeze,5,6 it remains difficult to predict which children will go on to develop asthma.7 As a result, the treatment of wheeze in infants and preschool children remains unsatisfactory.8,9
Studies in adult asthma involving endobronchial biopsy have allowed detailed investigation of the cellular and molecular mechanisms of asthma,10,11 and some information is also now available about asthma in older children.12–14 Similarly, investigation of airway pathology in infants and preschool children with wheeze should help us to understand more about the basis of wheeze in this age group, particularly the role of airway inflammation. The extent and pattern of inflammation may help to guide the use of anti-inflammatory drug treatment in a similar way to that used in patients with established asthma.
In view of the paucity of information regarding the pathology of asthma and wheeze in early childhood, the need for further research in this age group has been highlighted.15,16 However, there has been some reluctance on the part of investigators to undertake invasive studies in very young children because of ethical dilemmas surrounding safety. There is also an issue of biopsy size and quality. Typically, adult biopsies are taken through a bronchoscope with a 2.8 mm channel, and in older children with a 2.2 mm channel. However, in small children a bronchoscope with a 1.2 mm channel has to be used. At our centre in the last two years, increasing numbers of children under the age of five undergoing bronchoscopy have also had endobronchial biopsies and bronchoalveolar lavage, to provide additional information about the inflammatory component in cough and wheeze, and for diagnostic confirmation in suspected pulmonary tuberculosis.
If endobronchial biopsy is to be used to investigate the pathology of wheezing disorders in infants and preschool children, it is essential that the procedure is safe and that good quality biopsies can be obtained. Our aim in this report was therefore to investigate whether the performance of endobronchial biopsy in preschool children undergoing flexible bronchoscopy increases the risk of the procedure, and to examine whether biopsies so obtained were of suitable quality for research.
METHODS
Subjects: patients having flexible bronchoscopy and endobronchial biopsy
The case notes of 33 children (mean age 31 months, range 4 to 59; mean weight 12.6 kg, range 5.1 to 18.8), in whom bronchoscopy and endobronchial biopsy were done by one consultant respiratory paediatrician (AB) at the Royal Brompton Hospital between January 2000 and November 2002, were evaluated for information about the general anaesthetic and about any complications that occurred during or after the procedure.
Controls: patients having flexible bronchoscopy without endobronchial biopsy
Thirty three controls matched for weight and age (mean age 28 months, range 3 to 52; mean weight 12.5 kg, range 4.7 to 18.4), in whom flexible bronchoscopy without endobronchial biopsy had been done by the same bronchoscopist during the same period, were identified from the database. Information concerning the general anaesthetic and complications was obtained from the case notes.
Consent
Fully informed consent for the bronchoscopy/BAL/endobronchial biopsy was obtained from the parents of all the patients.
Anaesthesia
Flexible bronchoscopy was done in theatre under general anaesthesia. The details of anaesthetic administration at our centre have been described previously.17
Flexible bronchoscopy
The bronchoscope to be used was determined by the age of the child. A 2.7 mm instrument (model XP40, Olympus KeyMed, Southend-on-Sea, Essex, UK) was used for children aged up to two years, and a 3.6 mm instrument (model 3C20 or 3C40, Olympus KeyMed) for those age two to five years. Both bronchoscopes have a 1.2 mm suction channel. If bronchial lavage was done, this was from the right middle lobe unless the findings indicated an alternative more appropriate site. Three aliquots of 1 ml/kg 0.9% saline were used. After lavage, up to six endobronchial biopsies were taken, using biopsy forceps FB-56D-1 (Olympus KeyMed), from the subcarinae of the right lower lobe, unless a specific lesion appropriate for biopsy was identified elsewhere. The forceps were passed through the suction channel, and biopsies were taken under direct vision at the junction of the subcarinae. The biopsy forceps were closed at the subcarinae for approximately two to three seconds before removal.
Postoperative care
Patients were observed initially in the theatre recovery area, and subsequently on the ward. Regular observations were carried out for at least four hours after the procedure.
Complications
Any complications that occurred during the general anaesthetic were recorded prospectively on a data sheet. Any later complications were identified from the nursing observation charts and medical notes.
Histology
Biopsies were fixed in 10% formal saline solution overnight and processed into paraffin blocks. Three 5 µm sections were then taken at 25 to 50 µm intervals, dependent on biopsy size. Sections were stained using haematoxylin and eosin and assessed semiquantitatively by a consultant histopathologist (AGN) for the presence or absence of the following histological features: epithelium, reticular basement membrane, subepithelial stroma and inflammatory cells, submucous glands, and smooth muscle. For each subject, the length of reticular basement membrane was measured in the largest biopsy obtained using image analysis (NIH image 1.55, Maryland, USA).
Analysis
The two groups were frequency matched to ensure similar demographic characteristics, and complications occurring in the groups were compared using the χ2 test with Yates correction.18
RESULTS
Thirty three children (17 boys, 16 girls) who underwent endobronchial biopsy were identified, and matched with 33 controls (22 boys, 11 girls). The indications for bronchoscopy are listed in table 1. All the biopsy patients and 30 of the 33 controls had bronchoalveolar lavage.
Indication for bronchoscopy
Details of the anaesthetic are listed in table 2. There was no difference between groups in the number of patients who had a complication during the procedure, or in the severity or type of complications.
Details of anaesthetic
There was also no significant difference in the number, type, or severity of complications occurring after the procedure (table 3). One patient from each group needed transfer to the paediatric intensive care unit overnight for observation, but none required positive pressure ventilation. The main complication after bronchoscopy was the development of fever above 38.5°C. There were no incidences of significant bleeding or pneumothorax in the biopsy group. The latter was confirmed on chest x ray in 20 patients. Chest x ray was done in these 20 after the bronchoscopy to assess the position of a pH probe, which had been passed under general anaesthesia after the bronchoscopy. (Chest x ray is not routinely requested after bronchoscopy.) Additionally, when all 66 patients were considered together, there were no significant differences in complications occurring between children under or over 10 kg in weight.
Progress after the procedure*
Histology
Suitable biopsies for assessment were available for 30 of the 33 patients. Of the other three, the amount of sampled tissue was too small for histological processing in one case, wholly obscured by crush artefact in one, and contained necrotic cell debris related to tuberculosis in the third. In the 30 suitable specimens, reticular basement membrane was present in all 30, with at least 1 mm of basement membrane in 21. Sufficient subepithelial stroma for assessment of inflammation was present in 26. Areas of smooth muscle were present in 23, and submucous glands were identified in 22. There was no clear relation between the number of biopsies taken from each subject and the overall biopsy quality (table 4). Details on the value of the information obtained from biopsies in planning further management for the individual are given in table 5.
Biopsy quality in relation to the number of biopsies taken
Influence of biopsy report on subsequent patient management
DISCUSSION
This report shows that in preschool children undergoing bronchoscopy and bronchoalveolar lavage under general anaesthetic in a tertiary centre, endobronchial biopsy carries no extra risk. In addition, biopsies obtained from this age group are of sufficient quality to assess several different structures in the airway wall.
To our knowledge, this is the first report of the safety of undertaking endobronchial biopsy in preschool children. It is important to highlight the safety of the procedure in addressing ethical issues raised by research involving endobronchial biopsy in preschool children. Complications are not uncommon in young children undergoing bronchoscopy. Carrying out an endobronchial biopsy as well could cause additional complications, as the anaesthetic may be more prolonged and the procedure itself may carry risks. The inclusion of a matched control group subjected to exactly the same procedures but without endobronchial biopsy was therefore an essential part of the study. However, there was no significant difference in the number, type, or severity of complications between the groups. The main complication seen after the procedure was the development of a fever. This is a recognised complication of bronchoalveolar lavage,19 which was done in all biopsy patients and in 30 of the 33 controls. As there was no difference between the groups in the incidence of fever, it is most likely that this complication was a result of the lavage rather than of the biopsy. Furthermore, the complications that are thought to be specifically associated with performance of biopsy, for example bleeding, were not seen in any of the biopsy group. This is in contrast to transbronchial biopsy, which carries a small but definite risk of bleeding and pneumothorax.20,21 We do not advocate the use of transbronchial biopsy as a research procedure in children.
It must also be stressed that all bronchoscopies were done in a tertiary centre, with trained personnel, and the general anaesthetic was given by consultant paediatric anaesthetists. Anaesthetic details and complications during bronchoscopy have been collected prospectively at the time of the procedure at our centre for the last five years. Information on any complications occurring after the procedure was obtained retrospectively, and therefore depended on the accuracy of the medical notes.
This report is in agreement with others that have shown that flexible bronchoscopy and bronchoalveolar lavage in children is safe,19 as is endobronchial biopsy in older children.17,22,23 In contrast to the findings of Gibson and colleagues,24 when we considered all patients (biopsy group and controls), we did not find any significant difference in complications occurring in children under or over 10 kg in weight (data not shown). In the present study, safety was maximised by the use of a general anaesthetic given by a senior paediatric anaesthetist. Although sedation is an alternative,19 the use of a general anaesthetic allows the bronchoscopist to focus on the procedure while the airway is managed by an anaesthetist, and almost always ensures successful completion with minimal discomfort for the child.25
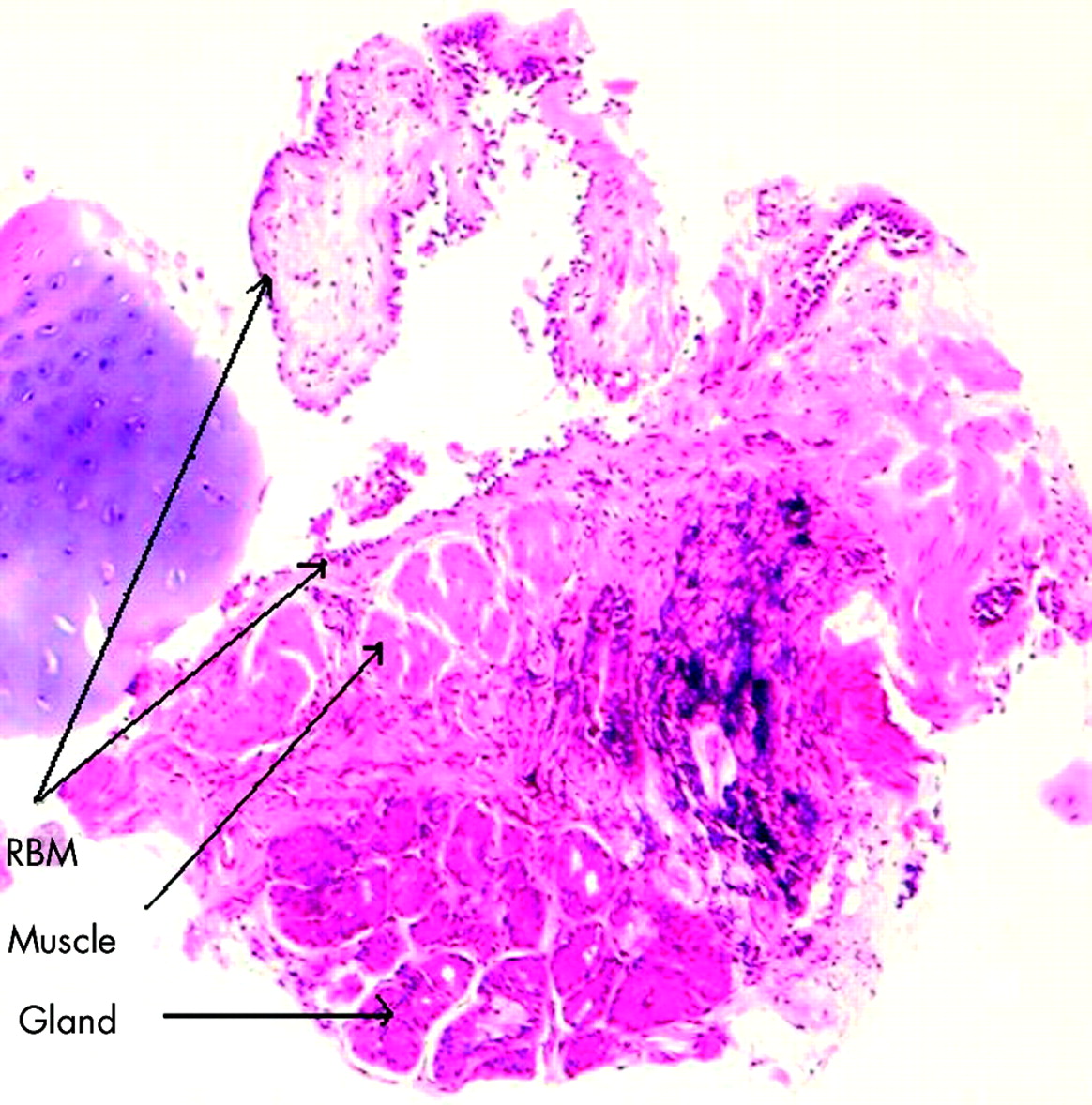
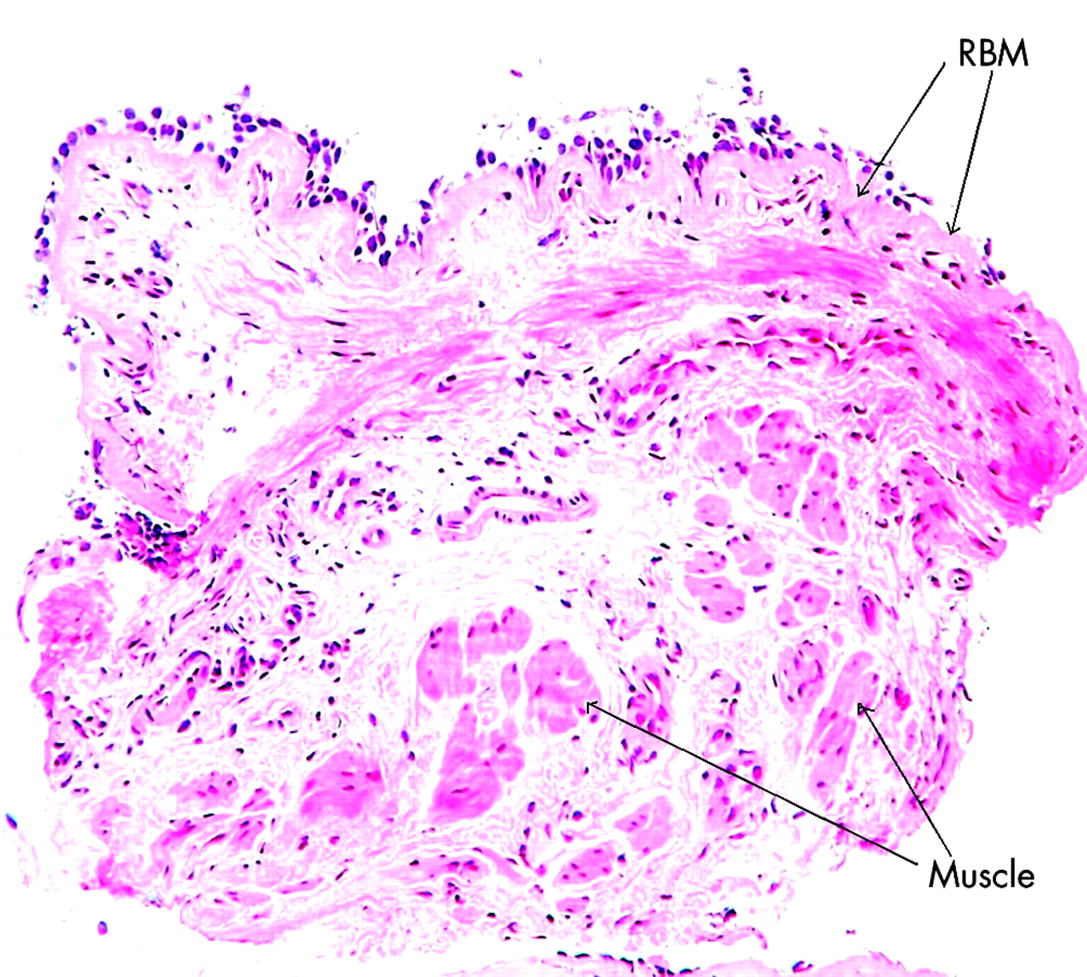
We believe this is the first report of biopsy quality in preschool children. Up to six endobronchial biopsies were taken in each case. There was no clear relation between the number of biopsies taken and the overall biopsy quality for an individual. The results suggest that no additional clinical information is obtained by taking more than three biopsies per subject. However, more may be required for research studies, depending on the hypothesis to be tested and the laboratory techniques used. Reticular basement membrane, the thickness of which is often used as a marker of airway remodelling,11 was identified in all 30 biopsies that could be assessed (fig 1). In 21 of the 30, the length of reticular basement membrane was at least 1 mm, which is the minimum length recommended for research studies.26 Sufficient subepithelial stroma for assessment of the presence of inflammatory cells was seen in 26 of the 30 specimens. Smooth muscle was present in 23 cases (fig 2). This is very similar to the figure of 78% from Payne et al in older children.13 Epithelium was the only structural feature not seen consistently, and was only present in 18 of the 30 biopsies. This is often the case, even in biopsies obtained from adults with larger biopsy forceps.11

Low power view of an endobronchial biopsy section from a three year old child, showing thickening of the reticular basement membrane (stained with haematoxylin and eosin).
{kind=link}
{kind=link}
Low power view of an endobronchial biopsy section from a 17 month old child (stained with haematoxylin and eosin).
Our main aims in this report were to evaluate the safety of endobronchial biopsy in preschool children and assess the quality of the biopsies obtained. However, the results also provide some indication of the clinical value of endobronchial biopsy in this age group, although the retrospective nature of this report is a weakness. Endobronchial biopsy was done as one of several investigations, which included bronchoscopy, bronchoalveolar lavage, and if appropriate, pH study and chest computed tomography. Information obtained (for example, the pattern of inflammation, reticular basement membrane thickness) from endobronchial biopsy was most useful in the evaluation of children with recurrent cough or wheeze, in whom a decision on the initiation or withdrawal of treatment with inhaled corticosteroids was being considered.
Conclusions
We have shown that in infants and preschool children endobronchial biopsy during flexible bronchoscopy carries no extra risk, and that the quality of biopsies obtained is sufficient to allow an assessment of airway remodelling and inflammation. It is important to emphasise that the study was done in a tertiary centre with appropriately trained personnel and specialist laboratory facilities. Any future research using endobronchial biopsy to investigate the pathology of wheezing disorders in this age group should be restricted to such centres,27 with collaboration between departments in order to maximise the use of samples and minimise the number of subjects enrolled. Studies involving comparison of invasive and non-invasive techniques should also be encouraged, to validate the latter for use in future research.28
Acknowledgments
We are grateful to Dr Rudiger Stenz for his help in obtaining information from the anaesthetic database.