Article Text

Abstract
Background: Chest physiotherapy is essential to the management of cystic fibrosis (CF). However, respiratory muscle fatigue and oxygen desaturation during treatment have been reported. The aim of this study was to determine whether non-invasive ventilation (NIV) during chest physiotherapy could prevent these adverse effects in adults with exacerbations of CF.
Methods: Twenty six patients of mean (SD) age 27 (6) years and forced expiratory volume in 1 second (FEV1) 34 (12)% predicted completed a randomised crossover trial comparing standard treatment (active cycle of breathing technique, ACBT) with ACBT + NIV. Respiratory muscle strength (PImax, PEmax), spirometric parameters, and dyspnoea were measured before and after treatment. Pulse oximetry (Spo2) was recorded during treatment. Sputum production during treatment and 4 and 24 hours after treatment was evaluated.
Results: There was a significant reduction in PImax following standard treatment that was correlated with baseline PImax (r=0.73, p<0.001). PImax was maintained following NIV (mean difference from standard treatment 9.04 cm H2O, 95% confidence interval (CI) 4.25 to 13.83 cm H2O, p=0.006). A significant increase in PEmax was observed following the NIV session (8.04 cm H2O, 95% CI 0.61 to 15.46 cm H2O, p=0.02). The proportion of treatment time with Spo2 ⩽90% was correlated with FEV1 (r=−0.65, p<0.001). NIV improved mean Spo2 (p<0.001) and reduced dyspnoea (p=0.02). There were no differences in FEV1, forced vital capacity (FVC) or sputum weight, but FEF25–75 increased following NIV (p=0.006).
Conclusion: Reduced inspiratory muscle strength and oxygen desaturation during chest physiotherapy are associated with inspiratory muscle weakness and severity of lung disease in adults with exacerbations of CF. Addition of NIV improves inspiratory muscle function, oxygen saturation and small airway function and reduces dyspnoea.
- cystic fibrosis
- respiratory muscles
- chest physiotherapy
- non-invasive ventilation
Statistics from Altmetric.com
Chest physiotherapy is integral to the management of cystic fibrosis (CF) lung disease. Techniques to aid the removal of secretions from the airway have been shown to slow the rate of deterioration in pulmonary function.1 Patients with CF are required to perform these airway clearance techniques both during acute respiratory exacerbations and periods of clinical stability.2 Despite the essential nature of airway clearance techniques, they are often an onerous task for patients with CF and have been associated with increased energy expenditure, oxygen desaturation, respiratory muscle fatigue, and dyspnoea.3–,6 These effects are likely to be greatest during an acute exacerbation when energy expenditure is increased due to infection and inflammation, and bronchial obstruction and respiratory muscle performance are at their worst.7 These factors may compromise the patient’s ability to perform airway clearance techniques at a time when it is most crucial.
Non-invasive ventilation (NIV) with bilevel positive airway pressure has been shown to reduce respiratory muscle work at rest in adults with stable CF and respiratory failure.8 The effect of this form of NIV on airway clearance has not been examined and there is some controversy regarding its role in patients who produce copious respiratory secretions.9 A different mode of NIV, inspiratory pressure support ventilation, has been used to prevent respiratory muscle fatigue during airway clearance in children with stable CF.5 However, the results of this study may not be applicable to adults with CF because of differences in respiratory muscle performance.10 To date, no studies have evaluated the effects of NIV on airway clearance during acute exacerbations, a time when it may be most useful. The aim of this study was to evaluate the effects of bilevel positive airway pressure during airway clearance on respiratory muscle performance, pulmonary function, oxygen saturation, and sputum clearance in adults with acute exacerbations of CF.
METHODS
Study subjects
All patients aged 18 years or over admitted to a university teaching hospital with an acute exacerbation of CF were assessed for inclusion in the study. An acute exacerbation of CF was defined as the presence of four or more of the following symptoms: change in sputum production; new or increased haemoptysis; increased cough; increased dyspnoea; malaise; fatigue or lethargy; fever; anorexia or weight loss; sinus pain or tenderness; changes in sinus discharge; loss of appetite; more than 10% (of best over last 6 months) deterioration in lung function.11 Patients who produced more than 20 g sputum in 24 hours were eligible for inclusion. This was confirmed by a sputum collection conducted on admission. Subjects were excluded if they required continuous (24 hour) NIV; had decreased level of consciousness, pneumothorax, symptomatic gastro-oesophageal reflux requiring modification of treatment, major haemoptysis (200 ml or more over 24 hours), or oxygen saturation (Spo2) <90% on room air at study entry. Subjects were also excluded if they had started home antibiotic treatment before day 5 of admission.
The study was approved by the hospital ethics committee and written informed consent was obtained from each subject before testing.
Study design
Subjects participated in two treatment sessions—standard treatment and NIV assisted treatment—on days 3 and 4 of hospital admission. A within subject crossover design was used with subjects randomly allocated to treatment order. Treatments were conducted at the same time each morning and by the same physiotherapist. All measurements were obtained by an independent data collector who was blinded to treatment order.
Treatment methods
Active Cycle of Breathing Technique (ACBT)
The Active Cycle of Breathing Technique (ACBT)12 was used in both the standard and NIV assisted treatments. The ACBT cycle consisted of a sequence of six thoracic expansion exercises, breathing control (quiet breathing), six thoracic expansion exercises, breathing control, the forced expiration technique (one or two huffs from mid to low lung volume combined with breathing control), and cough as required. The number of cycles performed and number of coughs were recorded. The treatment was performed in body positions determined by the patient’s usual treatment regimen or the presence of focal chest signs on assessment, with a minimum of 10 minutes in each position. Treatment duration was 30 minutes.
NIV assisted treatment
During NIV assisted treatment NIV was administered with a bilevel device (BIPAP Duet LX Bi-Level System; Respironics, Pittsburg, USA) for the entire duration of the treatment. Inspiratory and expiratory pressure settings were determined at an acclimatisation session conducted on the day before the start of the study and were chosen to maximise both patient comfort and the level of pressure support delivered. A minimum expiratory pressure of 4 cm H2O was given. The patient interface consisted of a nasal mask (Mirage Mask System; ResMed, Sydney, Australia) and expectoration occurred without removal of the mask. A warm water humidifier (HC100, Fisher and Paykel Healthcare Pty Ltd, Breakfast Creek, Australia) was connected in series between the bilevel device and the nasal mask. A disposable bacterial filter (Suregard; RJ and VK Bird, Melbourne, Australia) was used to prevent cross infection.
Both sessions were performed without supplemental oxygen. Use of bronchodilators and dornase alfa on study days was standardised with respect to timing and dosage for each subject. Subjects continued with their usual predetermined physiotherapy regimens of airway clearance and exercise for the remainder of the day. These regimens were held constant until the end of the data collection period.
Measurements
Inspiratory and expiratory muscle strength were measured before and immediately after each treatment using maximal static respiratory pressures produced at the mouth (Pmax Monitor; PK Morgan Ltd, Kent, UK). PImax was measured at residual volume (RV) and PEmax was measured at total lung capacity (TLC) with the subject seated in a hard backed chair. Each pressure was measured at 1 minute intervals, a minimum of three times until there was less than 5% difference between the two highest values. The highest value obtained for PImax and PEmax was recorded and compared with predicted values.13 PImax was reported as a positive value for simplicity of recording. Subjects had been trained to carry out these manoeuvres on the day before the study to ensure that reproducible values were obtained. Standard pulmonary function testing was performed using a Vitalograph spirometer (Vitalograph Ltd, Buckingham UK) before and immediately after each treatment according to American Thoracic Society guidelines14 with the subject seated in a hard backed chair. Oxygen saturation (Spo2) was measured continuously throughout treatment using a pulse oximeter and finger probe (Oxypleth; Novametrics, Wallingford, CT, USA). Mean Spo2, minimum Spo2, and proportion of treatment time with Spo2 ⩽90% were obtained. Sputum expectorated during treatment, 4 hours after treatment, and for the remainder of the 24 hour period was collected and weighed (FX320 electronic balance; A&D Ltd, Tokyo, Japan). Breathlessness was measured at the beginning and end of each treatment using the Borg scale15 and preference for treatment type was recorded following the final treatment session.
A baseline measurement of static lung volumes was obtained during the 48 hour period before the treatment sessions in a constant volume body plethysmograph (Medgraphics 1085D Series with BREEZPF software; Medical Graphics Corporation, St Paul, Minnesota, USA). Body mass index (BMI), sputum pathogens, and current medications were recorded for all subjects.
Analysis of data
Crossover two sample t tests were used to analyse for effects attributable to treatment (standard v NIV assisted), period (day 3 v day 4), and carryover (the contribution of treatment on day 3 to response on day 4).16 The relationship between variables was assessed with correlations. Alpha was set at 0.05.
RESULTS
Twenty seven subjects fulfilled the selection criteria and were randomised to treatment order. One subject withdrew at the start of testing because of pain on respiratory muscle testing. The demographic data for the remaining 26 subjects are shown in table 1⇓. Inhaled bronchodilators were used by all subjects and 15 subjects also used dornase alfa. All subjects were colonised with Pseudomonas aeruginosa and none were colonised with Burkholderia cepacia. One subject used nocturnal NIV for hypercapnic respiratory failure and another had previously used NIV for respiratory support during a severe acute exacerbation. All other subjects were naive to NIV. Inspiratory pressures delivered during the NIV assisted session ranged from 10 to 20 cm H2O and expiratory pressures from 4 to 5 cm H2O. There was no correlation between level of pressure support and FEV1; however, there was a weak correlation between level of pressure support and RV/TLC (r=0.42, p=0.04).
Mean (SD) demographic data of study subjects
Baseline PImax varied between subjects, ranging from 56 to 171 cm H2O (47–173% predicted normal). There was a moderate association between baseline PImax and BMI (r=0.43, p=0.03). There was a significant reduction in PImax following standard treatment (p=0.04, fig 1⇓). The largest reductions were observed in those with lowest baseline inspiratory muscle strength (r=0.73, p<0.001) and lowest BMI (r=0.61, p<0.001). In contrast, PImax was maintained following NIV assisted treatment, resulting in a significant difference compared with the standard treatment (mean difference 9.04 cm H2O, 95% CI 4.25 to 13.83 cm H2O, p=0.006). Baseline PEmax also varied widely (40–148% predicted normal) and had a moderate association with BMI (r=0.45, p=0.02). However, PEmax did not change significantly following standard treatment but increased following NIV assisted treatment (mean difference 8.04 cm H2O, 95% CI 0.61 to 15.46 cm H2O, p=0.02; fig 1⇓).
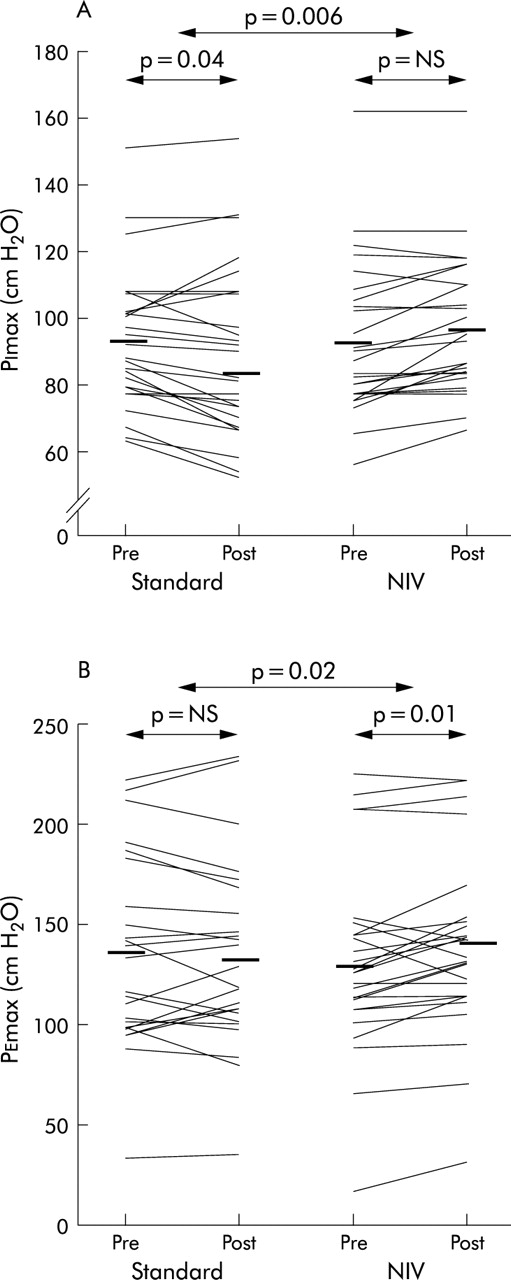
Effect of standard and NIV assisted treatments on maximal inspiratory (A) and expiratory (B) pressures. Individual data. Group means are represented by bold horizontal lines.
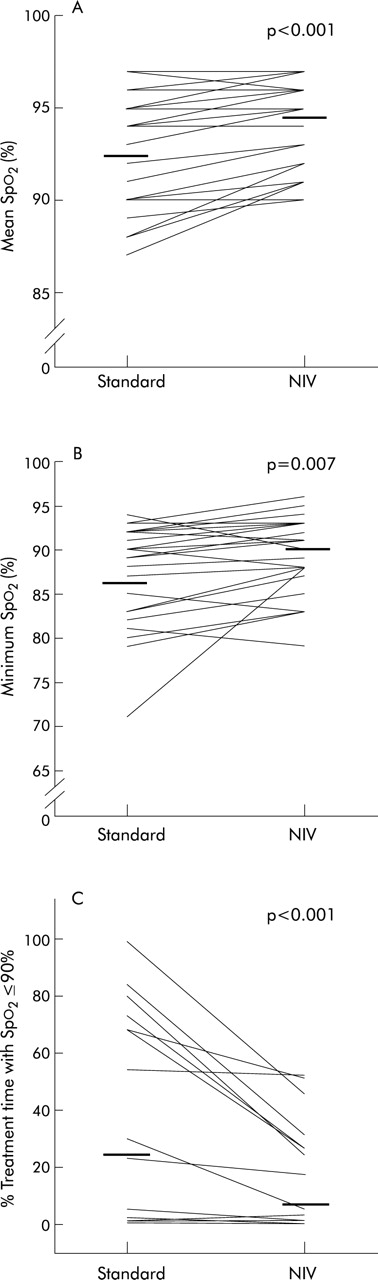
Mean and minimum Spo2 were significantly lower during standard treatment than during the NIV assisted session (fig 2⇓). The proportion of standard treatment time spent with Spo2⩽90% was correlated with FEV1 (r=−0.65, p<0.001). Addition of NIV resulted in a significant reduction in the proportion of treatment time with Spo2 ⩽90% (p<0.001).
{kind=link}
{kind=link}
Effect of standard and NIV assisted treatments on oxygen saturation: (A) mean Spo2, (B) minimum Spo2 and (C) % of treatment time with Spo2 ⩽90%. Individual data. Group means are represented by bold horizontal lines.
FEV1, FVC, and forced expiratory ratio (FEV1/FVC) did not change significantly following either treatment, but there was a significant increase in FEF25–75 following NIV assisted treatment (table 2⇓). There were no differences between standard and NIV assisted treatment in mean (SD) weight of sputum expectorated during treatment (15.92 (6.44) v 15.32 (6.20) g, p=NS), 4 hours after treatment (11.57 (9.65) v 13.97 (9.86), p=NS) or for the remainder of the 24 hour period (44.14 (23.26) v 41.35 (25.59), p=NS). Breathlessness scores increased following both treatments but to a slightly lesser extent following NIV assisted treatment (Borg score after treatment 2.69 (1.82) v 2.26 (1.96), p=0.02). Fifteen subjects preferred treatment with NIV, eight subjects preferred standard treatment, and three subjects did not have a preference.
Mean (SD) lung function parameters before and after treatment
No carryover or period effects were identified for any of the outcome variables. There was no significant difference in the number of ACBT cycles or coughs between the treatment sessions.
DISCUSSION
In this study of adults with acute exacerbations of CF and moderate to severe lung disease, standard chest physiotherapy with ACBT resulted in reduced inspiratory muscle strength and oxygen desaturation. These findings were associated with impaired baseline inspiratory muscle strength, reduced BMI, and more severe bronchial obstruction. The addition of NIV during treatment resulted in preserved inspiratory muscle strength and improved expiratory muscle strength. Improvements in oxygen saturation and small airway function were observed without change in the wet weight of sputum expectorated. No adverse effects were observed and NIV was well tolerated, with 58% of patients preferring it to the standard treatment.
The improvements in respiratory muscle strength during NIV assisted airway clearance are consistent with observations in children. Fauroux and colleagues5 evaluated the effects of the forced expiratory technique (FET) on respiratory muscle strength in 16 children with CF, all of whom had reduced respiratory muscle strength at baseline. A significant reduction in PImax was evident after 20 minutes of FET in all subjects. There was a significant increase in PImax following an identical treatment with the addition of inspiratory pressure support ventilation (PSV). The reduction in PImax was less consistent across subjects in our study. Our results suggest that, in adults, decreased inspiratory muscle strength following airway clearance is most likely when baseline inspiratory muscle strength and BMI are low. PImax was maintained in our subjects following NIV assisted treatment, but an increase was not observed.
We did not observe a reduction in PEmax following standard treatment. This difference in response of inspiratory and expiratory muscles may be related to differences in the force-volume relationship. As PEmax is not related to hyperinflation,17 the load imposed by the repeated inspiratory and expiratory manoeuvres associated with airway clearance may not be as great for the expiratory muscles in these severely hyperinflated patients. There may also be differences in response due to the nature of the airway clearance technique employed. The FET used by Fauroux et al consisted of slow active expirations from TLC to RV. The ACBT routine used in our study incorporated a more conventional form of FET consisting of forced expirations from mid to low lung volumes, hence the expiratory muscles were not required to generate force over such a wide range of lung volumes. An increase in PEmax was observed following NIV assisted treatment, the significance of which is unclear.
Significant falls in Spo2 occurred during standard treatment with ACBT. The effect of airway clearance on oxygen saturation has been inconsistently reported, with some studies indicating significant desaturation4,5 and others suggesting that this can be avoided by incorporating periods of breathing control.18 In our study the falls in Spo2 were observed mainly during the FET and this was not prevented by periods of breathing control. We also observed a relationship between the proportion of treatment time with Spo2 ⩽90% and FEV1, with the most desaturation evident in subjects with the greatest degree of airflow obstruction. The largest increases in Spo2 with NIV were seen in these same subjects. Improvement in oxygen saturation is likely to be associated with increased effective alveolar ventilation during NIV, which has previously been observed in adults with advanced CF.8 NIV may also have a role in the prevention of airway closure during the prolonged expirations required for airway clearance, similar to that postulated for positive expiratory pressure breathing.19
In concordance with previous short term studies of airway clearance techniques, standard treatment with ACBT had no effect on lung function parameters.20 Spirometric testing was performed to evaluate the safety of NIV as an adjunct to treatment, especially in light of concerns regarding impaction of secretions in the small airways as a result of positive pressure. No deleterious effects on small airway function were observed in this short term study and a small increase in FEF25–75 was observed. A weak but significant relationship between small airway function and mucociliary clearance has previously been reported.21
Wet weight of sputum is a simple, clinically available measurement that has been shown to impact on quality of life in CF.11 However, it may not accurately reflect the degree of mucus clearance as it does not account for concomitant mucus production, swallowing of secretions, or contamination with saliva. The crossover design used in this study attempted to control for some of these factors. In addition, we recruited only subjects who expectorated more than 20 g of sputum per day, as the relationship between mucus transport measured with radioactive aerosol tracer and expectorated mucus is thought to be stronger in patients who produce a large volume of secretions.22 Future investigations into the direct effect of NIV on bronchial mucus transport are required.
NIV delivers a high flow of gas at low relative humidity. This has been associated with impaired mucociliary clearance and drying of airway secretions within 30 minutes of exposure.23 To avoid these potentially confounding effects on airway clearance, we chose to incorporate a heated humidifier into the NIV circuit. It has previously been shown that exposure of sputum to 100% relative humidity does not increase wet weight at 1 hour.24 It is unlikely that deposition of water in the airway occurred at the temperature and relative humidity delivered during treatment, as there would have been no exchange of heat and moisture with the mucosa and the inspired gas did not contain aerosolised water.
A ventilatory mode that combined inspiratory and expiratory pressure was chosen for this study as it has been shown to provide better unloading of the diaphragm than inspiratory support alone in patients with COPD.25 Expiratory pressure settings in our study were kept at 4–5 cm H2O as other authors have reported interference with coughing at higher pressure settings.26 Inspiratory pressures were set to achieve the maximal level of pressure support associated with patient comfort. The level of pressure support delivered thus ranged from 6 to 15 cm H2O. This method of determining ventilatory settings reflects clinical practice but does not provide information on the degree of respiratory muscle unloading that was achieved. Vitacca and colleagues27 compared the effects of pressures set according to patient comfort with those set according to invasive measurement of respiratory mechanics. They found that both methods were effective in achieving respiratory muscle unloading. The weak correlation found in our study between the level of pressure support and degree of hyperinflation suggests that we did provide increased support to those with the greatest mechanical load during breathing.
Patients with CF now frequently survive to adulthood. The course of the disease is nonetheless characterised by progressive airflow obstruction and respiratory failure. Physiotherapists are frequently required to provide treatment to these severely unwell patients, including those requiring NIV for prolonged periods before transplantation.28 We have shown that NIV can safely be used to assist airway clearance during acute exacerbations in adults with CF, and that beneficial effects may be seen in those with severe bronchial obstruction and reduced inspiratory muscle strength. Further study is required to evaluate longer term effects and direct effects on secretion clearance.
Acknowledgments
This study was supported by the Alfred Hospital Research Trust, Australian Physiotherapy Association Victorian Branch, National Health and Medical Research Council of Australia Dora Lush Scholarship, and Anaesthetic Supplies Pty Ltd, Australia.