Article Text

Abstract
Most deaths from acute asthma occur outside hospital, but the at-risk patient may be recognised on the basis of prior ICU admission and asthma medication history. Patients who fail to improve significantly in the emergency department should be admitted to an HDU or ICU for observation, monitoring, and treatment. Hypoxia, dehydration, acidosis, and hypokalaemia render the severe acute asthmatic patient vulnerable to cardiac dysrrhythmia and cardiorespiratory arrest. Mechanical ventilation may be required for a small proportion of patients for whom it may be life saving. Aggressive bronchodilator (continuous nebulised β agonist) and anti-inflammatory therapy must continue throughout the period of mechanical ventilation. Recognised complications of mechanical ventilation include hypotension, barotrauma, and nosocomial pneumonia. Low ventilator respiratory rates, long expiratory times, and small tidal volumes help to prevent hyperinflation. Volatile anaesthetic agents may produce bronchodilation in patients resistant to β agonists. Fatalities in acute asthmatics admitted to HDU/ICU are rare.
- asthma
- intensive care
- mechanical ventilation
- inhalational anaesthetics
Statistics from Altmetric.com
Most asthma exacerbations are managed in the community or emergency department while the more severe cases that fail to respond to bronchodilator and anti-inflammatory therapy require admission to high dependency (HDU) or intensive care units (ICU).
Worldwide asthma prevalence is increasing, and with that the total number of admissions to hospital and intensive care. Although the time between the onset of symptoms and the requirement for ventilation is becoming shorter, the outcome is improving with fewer deaths and lower complication rates.1
MORTALITY
A history of mechanical ventilation or ICU admission is a well documented indicator of subsequent near fatal asthma.2,3 Women and smokers are also over-represented in both life threatening attacks and asthma deaths.3–5 It is believed that patients who have had a life threatening attack and those who die are from a similar demographic group. In a large study of patients admitted with a near fatal episode, two thirds of subsequent severe attacks or deaths had occurred within a year.2,5 Interestingly, the association between asthma deaths and β agonist use is still debated and there has been concern that the use of long acting β agonists may increase asthma mortality.6 This has not been confirmed in studies monitoring their use.7,8 In contrast, there is a consensus that underuse of anti-inflammatory treatment in the period leading up to the acute severe attack worsens prognosis.9
Unfortunately, a proportion of asthmatic patients die despite reaching hospital alive. Such deaths can usually be attributed either to inadequate observation or treatment. Sadly, a number of patients suffer unobserved respiratory failure that progresses to cardiac arrest and anoxic brain damage.10 A small number of patients are resistant to the most aggressive treatments and interventions.
Necroscopic studies of patients dying of acute severe asthma have found extensive mucus plugging of bronchi that has been termed “endobronchial mucus suffocation” (fig 1).11 Microscopic examination reveals extensive inflammatory changes that involve all airway wall components and the pulmonary arterioles.12,13 The degree of bronchial occlusion is much greater than in control asthmatic subjects, with mucus, desquamated epithelium, inflammatory cells and plasma exudate all contributing.11 Sudden asphyxic asthma may be a distinct pathological subtype in which intense bronchoconstriction causes respiratory failure, often over the course of 1–2 hours.14 Recovery appears to be rapid, which suggests that bronchoconstriction may be the predominant pathophysiological factor.15

Mucus cast of bronchial tree coughed up by an asthmatic patient during an exacerbation. Reproduced with permission of E Klatt, Utah.
INTENSIVE THERAPY AND MONITORING
Patients who fail to improve with optimal medical treatment in the emergency department should be considered for HDU or ICU admission to facilitate continuous monitoring of physiological parameters such as pulse oximetry, ECG, and arterial and central venous pressure. Equipment and experienced staff are also available for urgent procedures such as endotracheal intubation or the insertion of thoracostomy tubes.
Clinical, physiological and laboratory assessment
The immediate assessment of patients with asthma should include the degree of respiratory distress (ability to speak, respiratory rate, use of accessory muscles, air entry), degree of hypoxia (cyanosis, pulse oximetry, level of consciousness), and cardiovascular stability (arrhythmias, blood pressure). Accessory muscle use, wheeze, paradox, and tachypnoea may diminish as the patient tires.16
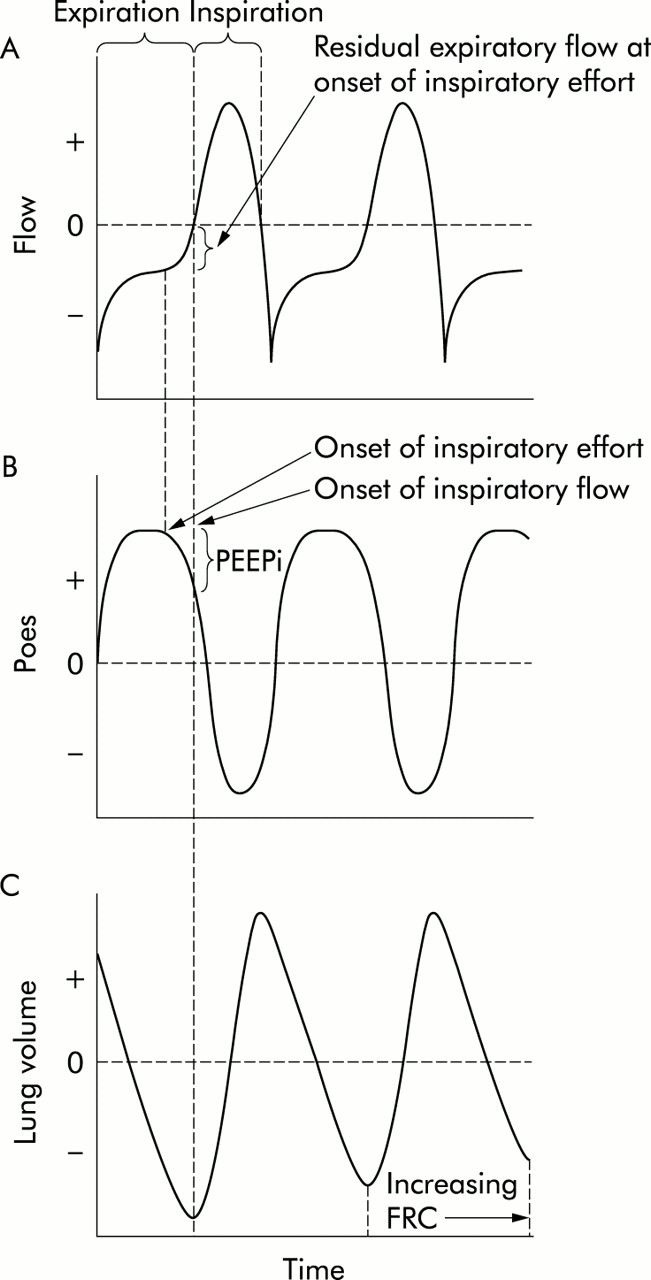
Forced expiratory volume in 1 second (FEV1) and peak expiratory flow rate are the most used and convenient measures of airflow obstruction that support clinical findings and quantify the response to treatment.17 Occasionally patients are too distressed to perform forced expiratory manoeuvres or there is a risk of precipitating further bronchoconstriction.18 Expiratory airflow limitation results in a dynamic increase in end expiratory lung volume which interferes with inspiratory muscle function, both of the diaphragm and the chest wall. The positive alveolar pressure at end expiration (PEEP) due to residual elastic recoil has been termed intrinsic (PEEPi) and its presence is suggested by residual expiratory flow at the onset of inspiration. In spontaneously breathing patients the magnitude of PEEPi can be estimated by the change in intrapleural pressure (usually measured by an oesophageal pressure probe) between the onset of inspiratory effort and the onset of inspiratory flow (fig 2). The work of breathing is increased in the presence of PEEPi because the residual alveolar pressure must be overcome by muscle effort before inspiratory flow commences. Many patients also use expiratory muscles to aid expiration, which may paradoxically worsen dynamic airway collapse and PEEPi. Inspiratory muscle activity may also persist during expiration,19–21 which contributes to increased expiratory work of breathing. In mechanically ventilated paralysed patients the magnitude of PEEPi is estimated by performing an end expiratory breath hold and measuring the airway pressure with reference to that of the atmosphere. In the presence of PEEPi a short expiratory time may lead to “breath stacking” and progressive hyperinflation as the next breath is initiated before the previous tidal volume has been completely exhaled. The pathological effects of PEEPi include hypotension due to reduced venous return and an increased risk of pneumothorax.22

{kind=link}
{kind=link}
(A) Schematic diagram of an asthmatic patient exhibiting significant residual flow at end expiration. (B) The oesophageal pressure (Poes), an estimate of intrapleural pressure, shows the degree of pressure change required to overcome intrinsic pressure (PEEPi) and initiate inspiratory flow. (C) A progressive increase in lung volume (breath stacking) occurs if expiratory time is insufficient to allow complete exhalation of the tidal volume.
Pulse oximetry is an invaluable adjunct to monitoring since the avoidance or abolition of hypoxia is a prime goal of treatment. Regular arterial blood gas measurements provide a measure of gas exchange and facilitate the monitoring of serum potassium levels. The arterial carbon dioxide tension (Paco2) and acid-base status help to identify the presence of pre-existing respiratory or metabolic acidosis, and the trend in Paco2 is helpful when assessing the response to treatment. The degree of hypokalaemia and lactic acidosis may also guide treatment.23 A chest radiograph is indicated to identify pneumothorax, areas of segmental or lobar collapse, or infiltrates that may suggest pneumonia. However, the yield is low.24,25 An ECG may detect myocardial ischaemia or identify arrhythmias, especially in older patients.26 Right axis deviation and right heart strain are common findings. Potassium, magnesium, calcium and phosphate deficiencies should be corrected to reduce the risk of arrhythmia and respiratory muscle weakness.
There are other causes of wheeze and respiratory distress that must be considered in the differential diagnosis. These include left ventricular failure, upper airway obstruction, inhaled foreign body, and aspiration of stomach contents.
Treatment
Intensive care treatment of the poorly responsive asthmatic patient should include high concentrations of inspired oxygen, continuous nebulisation of β agonists, intravenous corticosteroids, and respiratory support.27–29 Clinicians must be aware of the need to optimise oxygenation and avoid dehydration and hypokalaemia. Unrestricted high concentrations of oxygen (60–100%) must be administered to abolish hypoxaemia,27,30 unlike the patient with chronic obstructive lung disease where controlled limited oxygen is indicated.
Hypokalaemia is common and may be exaggerated by fluid resuscitation and the administration of β agonist bronchodilators. Repeated infusions of potassium chloride may be required with careful monitoring of serum levels and continuous ECG monitoring.
Specific asthma drug treatment
On admission to the ICU there should be a rapid review of earlier asthma treatment to identify elements that can be intensified or deficiencies remedied. Drugs contraindicated in asthma include β blockers, aspirin, non-steroidal anti-inflammatory drugs, and adenosine.
Corticosteroids
Evidence continues to accumulate that early treatment with adequate doses of corticosteroid improves outcome in severe acute asthma. There does not appear to be any benefit from high doses of hydrocortisone exceeding 400 mg/day, and no particular advantage of the intravenous over the oral route provided there is reliable gastrointestinal absorption.31 Inhaled corticosteroids have not been fully evaluated in this setting.
β agonists
Salbutamol (albuterol in North America) is the most commonly prescribed β agonist for the treatment of acute asthma.29 It appears to be more effective and induces less hypokalaemia when delivered by the inhaled route, although there is a theoretical rationale for administering salbutamol intravenously to bypass obstructed airways.32 Concerns over blood levels and potential cardiotoxicity may inhibit more aggressive use of nebulised salbutamol.33 However, continuous administration of nebulised salbutamol in doses approaching 20 mg/h can achieve bronchodilation without toxicity; indeed, the patient’s heart rate may fall with alleviation of airway obstruction.34
Interpretation of the literature on continuous nebulised salbutamol is hampered by differences in the definitions of “continuous” (length of time) and the delivered doses used in individual studies. One study compared 27.5 mg salbutamol by either continuous or intermittent nebulisation over 6 hours35 and, not surprisingly, showed little difference between intermittent and continuous regimens. Another study suggested benefit from prolonged continuous aerosol use only in severe asthma.36 Doses of 0.3 mg/kg/h nebulised salbutamol have been safely used in children without significant toxicity.37 Higher inhaled doses may be required in mechanically ventilated patients due to aerosol losses in the ventilator circuit.
Salbutamol delivered by metered dose inhaler (MDI) with a spacer device is at least as effective as nebulised drug in the management of acute asthma in the emergency department.38 In patients with hypoxia and respiratory distress, however, nebulised drugs may be easier to administer. Even intranasal and intratracheal instillation of β agonists may be effective in an emergency situation.39,40 Salbutamol is currently a racemic mixture of R and L forms. The S-enantiomer does not have β agonist effects and competes for the binding sites of the R form, levosalbutamol.41 Formulations of levosalbutamol have fewer side effects and greater efficacy than the racemic mixture, suggesting that it may be preferable in acute severe asthma.42 Terbutaline is an alternative β agonist that has been less widely studied but is effective by the inhaled, intravenous, and subcutaneous routes. Long acting β agonists such as salmeterol and eformoterol are not recommended because of their slow onset of action.
Both nebulised and intravenous adrenaline (epinephrine) are effective in the treatment of acute asthma. The putative benefits of the α-adrenergic component of adrenaline include reduced microvascular permeability and airway wall oedema, and less impairment of ventilation/perfusion matching than with more selective β agonists.43 However, there does not appear to be any clinical benefit over β agonists such as salbutamol.44
Some of the metabolic and cardiovascular complications of acute severe asthma may be exacerbated by high dose β agonist therapy. Lactic acidosis as a result of parenteral β agonist use, anaerobic metabolism due to high work of breathing, tissue hypoxia, intracellular alkalosis, and reduced lactate clearance due to liver congestion all contribute to the complex metabolic disturbances of acute severe asthma. Haemodynamically significant arrhythmias are relatively infrequent, even with the combination of methylxanthines and β receptor agonists45; however, β agonist induced hypokalaemia heightens the risk.
Box 1 Contraindications to a trial of mask CPAP or NIV in acute severe asthma
-
Need for immediate endotracheal intubation
-
Poor patient cooperation
-
Inability of the ventilator to supply high Fio2
-
Hypercapnia (CPAP less likely to benefit than NIV)
-
Excess respiratory secretions
-
Lack of experienced staff and/or a high dependency area
Ipratropium
Ipratropium bromide has a mild additional bronchodilating effect when added to β agonists that may only be significant in severe asthma.46 The safety profile and the fact that individual patients may obtain benefit have resulted in aerosolised ipratropium (500 μg 6 hourly) being recommended for the treatment of acute severe asthma.47
Aminophylline
The addition of aminophylline does not add to the bronchodilating effect of optimal doses of β agonists.48 Other reported benefits of aminophylline such as improving diaphragmatic endurance, stimulating ventilatory drive, and anti-inflammatory effect do not seem to improve outcome in acute severe asthma.49–53 Currently, aminophylline is not recommended as a first line drug in acute asthma management and its inclusion as a second line agent is still debated.46 However, when other agents fail to achieve bronchodilation, aminophylline can be used providing dosing regimens are adhered to. Typically, a loading dose of 5 mg/kg by slow intravenous infusion over 20 minutes is followed by an infusion of 500 μg/kg/h. If prolonged administration is required, daily monitoring of blood theophylline levels is essential. The therapeutic range is 55–110 μmol/l (10–20 mg/l).
ASSISTED VENTILATION
If there is inadequate response to drug treatment or if the patient is in extremis at presentation, mechanical ventilation may be required.
Mask continuous positive airway pressure (CPAP) and non-invasive ventilation (NIV)
In spontaneously breathing patients the application of low levels of mask CPAP (3–8 cm H2O) may improve respiratory rate, dyspnoea, and work of breathing in asthma, particularly if there is evidence of smoking related lung disease.20,54,55 There is a danger that CPAP may worsen lung hyperinflation. If patients are intolerant of the mask or do not derive benefit, CPAP should be withdrawn. In hypercapnic patients CPAP alone may not improve ventilation.
Few studies have looked specifically at NIV in asthma. Low levels of CPAP and pressure support of 10–19 cm H2O in acute severe asthma improved gas exchange and prevented endotracheal intubation in all but two of 17 hypercapnic patients.56 However, the rate of intubation in patients with acute asthma, even in the presence of hypercapnia, is low at 3–8%.28,57 It is reasonable to give asthmatic patients a trial of NIV over 1–2 hours in an HDU or ICU if there are no contraindications (box 1).56 Deciding when to initiate NIV, when a trial of NIV has failed, and optimising NIV in this setting require considerable expertise. In our experience, high flow ventilators specifically designed for NIV (such as the BiPAP Vision; Respironics, Pittsburg, USA) that allow significant mask and mouth leaks are better tolerated than many conventional ICU ventilators.
Endotracheal intubation
Cardiopulmonary arrest and deteriorating consciousness are absolute indications for intubation and assisted ventilation. Hypercapnia, acidosis, and clinical signs of severe disease at presentation may not require immediate intubation before an aggressive trial of conventional bronchodilator therapy.57,58 Conversely, progressive deterioration with increasing distress or physical exhaustion may warrant intubation and mechanical ventilation without the presence of hypercapnia.
Box 2 Summary of recommendations for the process of intubation
-
Performed/supervised by experienced anaesthetists or intensivists
-
Skilled assistants in an appropriate environment
-
Good preparation and understanding of the pathophysiology
-
Correct electrolyte disturbances and rehydrate
-
Obtain reliable large bore venous access
-
Continuous ECG and pulse oximetry
-
Continuous arterial monitoring not essential, but helpful
-
Pre-oxygenate
-
Use familiar method of intubation
-
Use familiar sedatives and muscle relaxants
-
Prepare for the rapid correction of hypotension, arrhythmias and barotrauma.
-
Ventilator set up and ready to monitor airway pressures early
-
Get aerosol delivery system for the ventilator connected or commence parenteral bronchodilator therapy
-
Plan ongoing sedation/paralysis before intubation
Once it has been decided that mechanical ventilation is required, the necessary medications, suitable monitoring equipment, and expert help should be sought. An understanding of the pathophysiology and anticipation of difficulties can minimise the complications associated with endotracheal intubation and ventilation. The best technique for intubation is generally that most familiar to the clinician performing the procedure.
The process of intubation begins with explanation and reassurance for the patient, followed by pre-oxygenation. The asthmatic patient is often dehydrated and the combination of PEEPi, the loss of endogenous catecholamines, and the vasodilating properties of the anaesthetic agents can cause catastrophic hypotension.59,60 Volume resuscitation before induction of anaesthesia can limit the degree of hypotension but vasoconstrictors such as ephedrine or metaraminol should be at hand.
Intubation is best performed by direct laryngoscopy after induction of general anaesthesia. Endoscopic methods have been advocated with either oral or nasal intubation,16,58 but laryngeal spasm and further bronchoconstriction may occur. Satisfactory local anaesthesia of the oropharynx, nasopharynx, and larynx is therefore essential. Longer term sedation is required once the airway has been secured. Some recommendations for successful and safe endotracheal intubation are summarised in box 2.
Drug therapy for intubation and mechanical ventilation
Anaesthetic agents and sedatives
Etomidate and thiopentone are short acting imidazole and barbiturate drugs, respectively, that are commonly used for intubation although rarely bronchospasm and anaphylactoid reactions have been reported. Longer term sedation may be obtained by infusion of midazolam (2–10 mg/h); metabolites may accumulate in renal and hepatic impairment. Propofol is a useful drug for intubation and intermediate term sedation, mainly because of its rapid onset and offset of action. It is easily titratable for intubation, providing deep sedation rapidly, although it has no analgesic properties. However, vasodilatation and hypotension occur, especially in dehydrated patients. Relatively little literature regarding its specific use in asthma is available. The doses of all the above agents need to be adjusted for patient size and pre-existing level of consciousness.
Ketamine is a general anaesthetic agent that has been used before, during, and after intubation in patients with acute severe asthma.61–63 It has sympathomimetic and bronchodilating properties. The usual dose for intubation is 1–2 mg/kg given intravenously over 2–4 minutes. It may increase blood pressure and heart rate, lower seizure threshold, alter mood, and cause delirium. Inhalational anaesthetics used for gas induction have the advantage of bronchodilation and may make muscle relaxation unnecessary. However, specialised anaesthetic equipment is required for this approach.
Opioids are a useful addition to sedatives and provide analgesia during intubation and mechanical ventilation. Morphine in large boluses causes histamine release, which may worsen bronchoconstriction and hypotension. Some intravenous preparations also contain metabisulphite, to which some asthmatics are sensitive. Fentanyl is a better choice of opioid for intubation as it inhibits airway reflexes and is short acting. It causes less histamine release than morphine but large boluses may cause bronchospasm and chest wall rigidity.
Neuromuscular blocking drugs
Rapid sequence induction with cricoid pressure should be used to prevent aspiration of gastric contents. Suxamethonium, a depolarising muscle relaxant, is widely used. It has a rapid onset and short duration of action but may cause hyperkalaemia and increased intracranial pressure. Rocuronium, a non-depolarising muscle relaxant with an acceptably rapid onset, offers an alternative. Allergic sensitivity may occur to any neuromuscular blocking agent and most may also cause histamine release and the potential for bronchospasm, particularly in bolus doses. Atracurium boluses should be avoided because of this possibility and vecuronium or pancuronium infusions used for longer term maintenance of muscle relaxation.
Myopathy and muscle weakness are well recognised complications of the long term administration of non-depolarising neuromuscular blocking agents in asthmatic patients with an incidence of about 30%.64–66 In most cases the myopathy is reversible, but may take weeks to resolve. There is an association between neuromyopathy and the duration of muscle relaxant drug use that is independent of corticosteroid therapy.65 The use of neuromuscular blocking agents should therefore be kept to a minimum.
Mechanical ventilation
Mechanical ventilation provides respiratory support while drug therapy reverses bronchospasm and airway inflammation.28 Abolishing hypoxia is the most important aim.
Modes of ventilation
Commonly adopted ventilation modes include pressure limited and time cycled (pressure control or bilevel ventilation) or volume limited and time cycled modes (synchronised intermittent mandatory ventilation, SIMV).28 In pressure limited modes, maximum airway pressure is set and the tidal volume delivered depends on respiratory system compliance. Volume cycled modes, however, deliver a set tidal volume and can be successfully and safely used provided an airway pressure limit is set appropriately. As the patient improves and begins to breathe, spontaneously triggered modes of ventilation such as pressure support ventilation (PSV) can be introduced.
Ventilator settings
The major variables that need to be set when placing a patient on mechanical ventilation include the oxygen concentration of inspired gas (Fio2), tidal volume (Vt) or inspiratory pressure, ventilator rate, inspiratory to expiratory time ratio (I:E ratio), and PEEP. The aims are to minimise airway pressure, allowing sufficient time for completion of expiration while achieving adequate alveolar ventilation. Suggested initial ventilator settings are shown in box 3.
Box 3 Initial ventilator settings in paralysed patients (adapted from Finfer and Garrard109)
-
Fio2 = 1.0 (initially)
-
Long expiratory time (I:E ratio >1:2)
-
Low tidal volume 5–7 ml/kg
-
Low ventilator rate (8–10 breaths/min)
-
Set inspiratory pressure 30–35 cm H2O on pressure control ventilation or limit peak inspiratory pressure to <40 cm H2O
-
Minimal PEEP <5 cm H2O
Outcome is improved in mechanically ventilated asthmatics by limiting airway pressure using a low respiratory rate and tidal volume while permitting a moderate degree of hypercarbia and respiratory acidosis.67 Hypercarbia has not been found to be detrimental except in patients with raised intracranial pressure or severe myocardial depression. Moderate degrees of hypercarbia with an associated acidosis (pH 7.2–7.15) are generally well tolerated. Reducing the respiratory rate to 8 or 10 breaths/min prolongs expiratory time so that I:E ratios of greater than 1:2 can be achieved. An attempt to increase minute ventilation (to reduce Paco2) by increasing the ventilator respiratory rate invariably reduces the expiratory time and I:E ratio, increases air trapping, and may paradoxically cause an increased Paco2. This has resulted in perceived failure of mechanical ventilation.68
Humidification of inspired gas is particularly important in asthmatic patients to prevent thickening of secretions and drying of airway mucosa, a stimulus for bronchospasm in itself.69
Ventilator alarms
These include peak pressure and low tidal volume/low minute ventilation alarms. If exceptionally high airway pressures occur or there is a sudden fall in Vt, blockage of the endotracheal tube, pneumothorax, or lobar collapse should be excluded. Plateau rather than peak airway pressure may provide the best measure of alveolar pressure and provide the best predictor of barotrauma, together with measures of hyperinflation such as PEEPi.70
Extrinsic PEEP
Low level CPAP may be beneficial in spontaneously breathing, mechanically ventilated patients, especially if expiratory muscle activity is contributing to dynamic airways collapse. However, in mechanically ventilated paralysed patients extrinsic PEEP was of no benefit at low levels and was detrimental at high levels because the fall in gas trapping was outweighed by the rise in functional residual capacity (FRC).22 However, in this study large Vt were used (up to 18 ml/kg); furthermore PEEPi and arterial blood gases were not measured. Changes in FRC and gas trapping may guide the level of PEEP. Applied extrinsic PEEP should not exceed PEEPi.
Topical drug delivery to the ventilated patient
Mechanical ventilation, whether invasive or non-invasive, may compromise the delivery of bronchodilator aerosols. The amount of nebulised drug reaching the airways depends on the nebuliser design, driving gas flow, characteristics of the ventilator tubing, and the size of the endotracheal tube.47,71 Drug delivery may vary from 0% to 42% in ventilated patients.72 The presence of humidification alone may reduce drug deposition by as much as 40%, but may be reversed by the addition of a spacer device.73,74 Both ultrasonic and jet nebulisers are effective in ventilated patients.75 Nebulisers may, however, be a source of bacterial contamination.76
Box 4 Recommendations for aerosol delivery to mechanically ventilated patients
Metered dose inhaler (MDI) system
-
Spacer or holding chamber
-
Location in inspiratory limb rather than Y piece
-
No humidification (briefly discontinue)
-
Actuate during lung inflation
-
Large endotracheal tube internal diameter
-
Prolonged inspiratory time
Jet nebuliser system
-
Mount nebuliser in inspiratory limb
-
Delivery may be improved by inspiratory triggering
-
Increase inspiratory time and decrease respiratory rate
-
Use a spacer
-
High flow to generate aerosol
-
High volume fill
-
Stop humidification
-
Consider continuous nebulisation
Ultrasonic nebulisers
-
Position in inspiratory limb prior to a spacer device
-
Use high power setting
-
Use a high volume fill
-
Maximise inspiratory time
-
Drugs must be stable during ultrasonic nebulisation
Metered dose inhalers have been widely used and may provide at least as good drug delivery as nebulisers, depending on actuator design and the presence of humidification and spacer devices.77,78 The recommended characteristics of aerosol delivery systems used in ventilated patients are shown in box 4. Ideally, each aerosol delivery system should be evaluated for each type of ventilator circuit used.73
THERAPEUTIC OPTIONS IN THE NON-RESPONDING PATIENT
A proportion of patients improve rapidly following the introduction of mechanical ventilation, and weaning should occur in line with this improvement. Unfortunately, for some there is difficulty in achieving adequate ventilation or there is persistent hypoxia. Difficulty in ventilation may be due to refractory bronchospasm, extreme hyperinflation, or mucus plugging.
Manual compression
This technique was first described anecdotally by Watts in 1984.79 Hyperinflation is relieved by manual compression of the chest wall during expiration.80 The technique has been advocated and used with success in both intubated and non-intubated patients, although it has not been fully evaluated by a controlled clinical study in humans.81,80
Mucolytics
There is often a striking degree of mucus impaction in both large and small airways that contributes to hyperinflation, segmental and lobar collapse with shunting, increased airway pressure, and barotrauma. Chest physiotherapy and mucolytics have no proven benefit. Bronchoscopic lavage with locally applied acetylcysteine may be used to help clear impacted secretions in selected refractory patients but its routine use is not advocated.82 Recently, recombinant DNase, a mucolytic prescribed for sputum liquefaction in cystic fibrosis, has been used to treat mucus impaction in asthma but there are no clinical trials.83
Inhalational anaesthetic agents
Halothane, isoflurane, and sevoflurane are potent bronchodilators in asthmatic patients receiving mechanical ventilation who have failed to respond to conventional β adrenergic agents.84 Experimental evidence indicates a direct effect on bronchial smooth muscle mediated via calcium dependent channels as well as by modulating vagal, histamine, allergen, and hypoxia induced bronchoconstrictor mechanisms.85,86 Furthermore, these agents reduce pulmonary vascular tone resulting in lower pulmonary artery pressures in acute asthma.87 Bronchodilator responses are seen in the form of reduced peak airway pressures within minutes, associated with improved ventilation distribution (lower Paco2) and reduced air trapping.88 Although bronchodilator effects are seen at sub-anaesthetic concentrations, these agents also offer a relatively expensive method of sedation. A few ICU ventilators, such as the Seimens Servo 900 series, can be fitted with a vaporiser allowing anaesthetic gases to be administered. Effective exhaled gas scavenging systems are required when using inhalational anaesthetics in the ICU. If this facility is not available a Cardiff canister can be added to the expiratory port of the ventilator to remove effluent anaesthetic gases. Significant side effects such as hypotension and myocardial irritability exist, and prolonged administration of some agents may result in bromide or fluoride toxicity.89 Sevoflurane, a halogenated ether, is largely devoid of cardiorespiratory side effects and may be the preferred agent. Administration of sub-anaesthetic concentrations of these agents via face mask may relieve bronchospasm refractory to conventional treatment.90
One of the difficult aspects of mechanical ventilation of the acute asthmatic patient is the weaning and extubation process. The presence of the endotracheal tube within the larynx and trachea induces bronchoconstriction which becomes troublesome as the sedation is withdrawn in preparation for extubation.91,92 Use of an inhalational anaesthetic agent allows the endotracheal tube to be removed under anaesthesia with the confident expectation of rapid recovery once the anaesthetic is discontinued.
Helium
A mixture of helium and oxygen (heliox) may reduce the work of breathing and improve gas exchange because of its low density that reduces airway resistance and hyperinflation. However, the benefits are marginal and the concentration of inspired oxygen is consequently decreased. Flow meters and nebuliser generator systems must be adapted for heliox use in ventilated patients.93 The use of heliox to prevent intubation has not been studied, but dyspnoea scores were improved in one study, possibly by reducing the work of breathing.94
Magnesium sulphate
Early anecdotal reports suggested benefit from intravenous magnesium sulphate, which has been inconsistently supported by randomised studies.95–99 A significant benefit was recently observed in children receiving intravenous magnesium sulphate (40 mg/kg) during acute asthma attacks.100 Overall, the case for magnesium sulphate in acute asthma requires further evaluation in both adults and children.
Leukotriene inhibitors
Leukotrienes are inflammatory mediators known to be active in the airway inflammation of asthma. Leukotriene receptor antagonists (zafirlukast, montelukast) and synthesis blockers (zilueton) currently have a relatively minor role in the management of poorly controlled and aspirin sensitive asthma.101 However, recent work has suggested a role for leukotriene antagonists in acute asthma.102–105
Platelet activating factor (PAF) inhibitors
PAF inhibitors attenuate the late response in asthma but have limited clinical efficacy.106
Nitric oxide (NO)
NO exerts a weak bronchodilator effect.107 It dilates pulmonary arteries and, when inhaled, may improve ventilation/perfusion matching.
OUTCOME AND FOLLOW UP
ICU admission identifies an asthmatic patient as a member of a poor prognostic group.3,5,108 Follow up should include a focus on anti-inflammatory therapy and a written management plan that may include the emergency use of intramuscular adrenaline. Issues such as access to health care services, compliance with treatment, avoidance of triggers, socioeconomic and psychosocial factors also need to be addressed.
Acknowledgments
The authors would like to thank Dr Duncan Young for his review of the manuscript and helpful suggestions.