Article Text

Abstract
Background: Acute exacerbations of chronic obstructive pulmonary disease (AE-COPD) are a common cause of hospital admission. Many exacerbations are believed to be due to upper and/or lower respiratory tract viral infections, but the incidence of these infections in patients with COPD is still undetermined.
Methods: Respiratory syncytial virus (RSV), influenza A and B, parainfluenza 3, and picornaviruses were detected by nested reverse transcription polymerase chain reaction (RT-PCR) in upper (nasal lavage) and lower respiratory tract specimens (induced sputum). In a 2:1 case-control set up, 85 hospitalised patients with AE-COPD and 42 patients with stable COPD admitted for other medical reasons were studied.
Results: Respiratory viruses were found more often in sputum and nasal lavage of patients with AE-COPD (48/85, 56%) than in patients with stable COPD (8/42, 19%, p<0.01). The most common viruses were picornaviruses (21/59, 36%), influenza A (15/59, 25%), and RSV (13/59, 22%). When specimens were analysed separately, this difference was seen in induced sputum (exacerbation 40/85 (47%) v stable 4/42 (10%), p<0.01) but was not significant in nasal lavage (exacerbation 26/85 (31%) v stable 7/42 (17%), p=0.14). In patients with AE-COPD, fever was more frequent in those in whom viruses were detected (12/48, 25%) than in those in whom viruses were not detected (2/37, 5%, p=0.03).
Conclusion: Viral respiratory pathogens are found more often in respiratory specimens of hospitalised patients with AE-COPD than in control patients. Induced sputum detects respiratory viruses more frequently than nasal lavage in these patients. These data indicate that nasal lavage probably has no additional diagnostic value to induced sputum in cross-sectional studies on hospitalised patients with AE-COPD and that the role of viral infection in these patients is still underestimated.
- respiratory virus
- chronic obstructive pulmonary disease
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) is the fourth leading cause of mortality world wide and an important cause of global burden of disease.1 The disease is associated with intermittent exacerbations characterised by acute deterioration in symptoms, lung function, and quality of life.2,3 Exacerbations have major effects on health status, are associated with considerable morbidity and mortality, and often lead to hospital admission with high treatment costs.4 Infectious agents are recognised as a major pathogenic factor in exacerbations. Bacteria have a role in the pathogenesis5,6 and the exacerbations of COPD. However, bacteria are absent in about 50% of exacerbations and the frequency of isolation does not increase during exacerbation.7
The relevance of viral infections has been studied by sensitive methods such as reverse transcription polymerase chain reaction (RT-PCR) in exacerbations of bronchial asthma8,9 and it has been shown that respiratory viruses can directly infect the lower respiratory tract.10 Furthermore, 85% of asthma attacks in children were associated with viral infections.11 Using less sensitive methods such as viral cultures and serology, viruses could be detected in only 44% of asthma exacerbations in adults12 and in only 24% of severe asthma attacks requiring hospitalisation.13 Exacerbations of COPD have previously been investigated using these less sensitive methods. Most authors therefore found respiratory viruses in only about 20%, probably underestimating the problem.14–16
Comparison of different diagnostic methods for the detection of respiratory viruses including virus culture, antigen detection tests, serology, and PCR showed that PCR is more sensitive and at least equally specific.17,18 Moreover, the technique of sputum induction is known as a non-invasive tool for the evaluation of lower airway inflammation in COPD.19,20 The first study using these techniques has recently been published, underlining the importance of respiratory viruses in exacerbations of COPD.21
The aim of this case-control study was to document the presence of five common respiratory viruses in respiratory tract specimens of hospitalised patients with exacerbations of COPD with RT-PCR and to correlate these data to clinical parameters.
METHODS
In a prospective case-control study two groups of patients with COPD (one group with an acute exacerbation of COPD (AE-COPD) and a control group with stable disease) were studied between July 1998 and September 1999 at a 600-bed university hospital in Bochum, Germany. Subjects were recruited in a 2:1 ratio each month in order to prevent seasonal selection bias. All subjects were first identified and selected by the emergency room physician and then investigated further by the physician in charge of the study.
Inclusion criteria for both groups were: age 18–85 years; exacerbated (cases only, see definition below) or stable (controls only, see definition below) COPD (see definition below); chronic airflow limitation (forced expiratory volume in 1 second (FEV1) <80% predicted); and admitted to hospital. Exclusion criteria for both groups were: bronchial asthma (see definition below) and dyspnoea of other origin (see definition below).
The study was approved by the ethical committee of the Ruhr-University of Bochum, Germany. Written informed consent was obtained from all subjects and control patients before inclusion in the study.
Data collection
The following parameters were recorded on admission: age, sex, smoking habits, current medication, clinical signs and symptoms of respiratory infection, pulmonary function testing, chest radiograph for identification of pulmonary infiltrates, C reactive protein (CRP), and routine blood chemistry and counts. Pulmonary function was reassessed at the clinical end point of hospital discharge (fig 1). Within 48 hours after admission nasal lavage fluid and induced sputum were collected (see protocols below).

Flow of patients through the study.
Definitions
Asthma was suspected in the presence of a compatible history of cough, sputum, wheeze, chest tightness, or breathlessness, particularly when the symptoms were episodic and worse at night.22 Special attention was paid to history of atopic disease and seasonal character of symptoms.
COPD and its stages (I–III) were defined according to the ATS criteria.23
Exacerbation of COPD: condition according to the definition given above plus worsening in dyspnoea, cough and expectoration.24
Stable COPD: condition according to the definition given above without exacerbation (defined above) in the 30 days before hospital admission and without changes in treatment within the last 14 days (including inhaled and oral medication).
Dyspnoea of other origin: cardiovascular, bronchopulmonary (pneumonia, interstitial lung disorders), pleural, or others (upper airways obstruction, neuromuscular, anaemia).
Smoking habit: non-smokers had never smoked, ex-smokers had smoked daily and given it up. Smokers smoked daily at the time of the study. Amount of lifetime smoking was assessed as pack-years.
General physical condition: assessed using the definition by WHO (0 = no restricting condition; 1 = ambulatory patient; 2 = disabled at work, <50% in bed during day time; 3 = >50% in bed during day time, needs special care; 4 = completely disabled).
Diagnostic methods
Spirometric tests were performed using a Jaeger Flowscreen device (E Jaeger, Würzburg, Germany). The best of three trials was selected and data were compared with reference values.25 Forced expiratory volume in one second (FEV1) and forced and inspiratory vital capacity (FVC, IVC) were assessed. A routine posterior-anterior chest radiograph was evaluated on admission by expert radiologists for all subjects.
Nasal lavage
All subjects were positioned on a chair with the head inclined towards the chest for nasal lavage. A total of 6 ml non-buffered isotonic saline solution (NaCl 0.9%) was injected and aspirated into each nose orifice using a special adapter (Allergopharma, Reinbek, Germany) and a syringe for at least five cycles. Collected specimens were then translocated into a sputum container, transported to the laboratory, and processed within 20 minutes.
Induced sputum
Sputum was induced according to slightly modified protocols.26,27 Briefly, 20 minutes after two puffs of salbutamol (200 μg/puff) FEV1 was assessed and patients with FEV1 <60% predicted inhaled non-buffered isotonic saline solution (NaCl 0.9%) using a PariBoy nebuliser (Starnberg, Germany); all others inhaled hypertonic saline solution (3%). The concentration in the latter could be incremented according to clinical efficacy in steps of 1% lasting 10 minutes up to 5%. All patients were instructed to rinse the mouth and throat and to deeply expectorate at least every 5 minutes. Spirometry was repeated in all subjects to exclude bronchoconstriction.
Nasal lavage fluid and sputum processing
Nasal lavage and sputum samples were diluted with an equal volume of 10% dithiothreitol (Sputolysin, Calbiochem; La Jolla, USA) and incubated for 15 minutes at room temperature. Specimens were then centrifuged with 1500 rpm for 15 minutes (CS-6KR, Beckman Instruments Inc, Palo Alto, USA). The supernatant was collected, cells were resuspended in 500 μl phosphate buffered saline, and both were frozen at –20°C until further processing within 7 days.
Viral ribonucleic acid (RNA) extraction
Cells and cell-free supernatants (250 μl and 1000 μl, respectively) from induced sputum and nasal lavage samples were stored at –20°C. The RNA isolation procedure was carried out immediately after thawing. RNA was prepared by binding to a silica matrix followed by a spin column purification according to the instructions of the manufacturer (Qiagen, Hilden, Germany) of QIA RNeasy kit (cells) and QIAamp DNA blood kit (cell-free supernatants). The final volumes were 150 μl for cells and 100 μl for cell-free supernatants. All samples were stored at –70°C.
Reverse transcription and RT-PCR analysis
Complementary DNA (cDNA) was prepared by reverse transcription of 5 μl of the eluted RNA. The reaction volume was 26 μl, containing 5 μl 5× first strand buffer (Gibco BRL), 1 μl DTT (Gibco BRL), 1 μl DMSO (Merck), 2 μl 5 mM of each dNTP (Amersham), 5 μl virus-specific primer (100 pmol), 5 U M-MLV-RT, and 5 μl RNA. All samples were run with simultaneous negative controls—that is, reaction mixtures with 5 μl sterile water instead of sample RNA). The reaction mixtures were overlaid with 30 μl mineral oil, incubated at 37°C for 45 minutes, and then heated at 95°C for 5 minutes. All cDNA samples were stored at –20°C.
The polymerase chain reactions for the detection of RSV, influenza A, influenza B, parainfluenza (PIV) 3, and enterovirus RNA were carried out as nested PCR (except semi-nested PCR for the detection of rhinovirus (HRV) RNA). For the first amplification step the reaction mixture was made up to 100 μl with 10 μl 10× PCR buffer (Amersham), 0.2 mM of each dNTP, 50 pmol of each primer, 2 U Taq polymerase, and 10 μl cDNA. The reaction mixtures were overlaid with 100 μl mineral oil and amplified in a thermal cycler (Peltier thermal cycler, MJ Research). In the nested PCR step 3 μl of the initial reaction product were added to a reaction mixture of 100 μl containing the same components as the first PCR step but a reduced primer concentration (20 pmol). Table 1 shows all primer sequences, their genomic localisation, cycle profiles, and the expected length of the PCR product. Obtained PCR products were detected by electrophoresis on ethidium bromide-stained 2% agarose gels and photographed under UV illumination. One negative control (purified water) was included in each run and valid results were only assumed if all negative controls showed no band in electrophoresis. PCR results were accepted as positive when a clear band was detected at the level of the expected base pair length for each virus. The validity of the base pair length was checked before the study.28
Primer sequences, genomic localisation, cycle profiles, and the expected length of the PCR product
RNA isolation and RT-PCR analysis were carried out by the Department of Medical Microbiology and Virology at the Ruhr University of Bochum. The personnel were blinded to the clinical data. A numerical coding system was used to identify the specimens.
Statistical analysis
The primary objective of this study was to compare the frequency of viral detection in respiratory specimens of patients with and without an acute exacerbation of COPD. Secondary objectives were to distinguish the viral detection between the upper and lower respiratory tract and to correlate these findings with clinical data.
Continuous data were assumed to be of non-parametrical distribution and results were expressed as median (range). Differences between groups were assessed by the Mann-Whitney U test. For discrete variables, frequencies and percentages were reported and compared using the χ2 test or Fisher's exact test where appropriate. The Yates correction procedure was applied to all comparisons. All significance levels were set to 5%. Data were analysed and processed using SigmaStat Version 2.0 on a Windows 98 operating system.
RESULTS
Patients
A total of 194 patients were enrolled in the study (fig 1), 67 (35%) of whom could not enter the final analysis for the following reasons: 46 (24%) did not fulfil inclusion criteria, 12 (6%) withdrew consent, 26 (13%) had FEV1 >80% predicted, eight (4%) had concurrent reasons (tuberculosis, n=4; bronchial carcinoma n=2; pulmonary embolism n=1, and heart failure n=1). Six (3%) suffered from diseases rendering a further investigation impossible (myocardial infarction, n=1; acute respiratory failure, n=5); 14 (7%) were not able to produce enough sputum (patients did not differ significantly in their clinical status and lung function from the study group, data not shown); and the viral specimens were lost for one patient (0.5%).
A total of 127 patients (table 2) were analysed, 85 (67%) patients with AE-COPD and 42 (33%) controls. The two groups were comparable in terms of age, sex, body mass index (BMI), smoking habits, history of COPD, general physical condition, and FEV1 at baseline. For patients with AE-COPD the FEV1 at baseline had to be assessed before discharge to determine comparability with the non-exacerbated group.
Demographic and spirometric data of study patients
FEV1 on admission in patients with AE-COPD showed increased airflow limitation compared with controls (p<0.01), as well as clinically more frequent wheezing and rhonchi (p<0.01, table 3). Clinical signs of airway infection including nasal congestion and rhinorrhoea, sore throat, purulent sputum, and fever as well as headache and muscle pain were significantly more frequent in patients with AE-COPD. The two groups of patients were comparable with regard to basic clinical status and differed according to symptoms and clinical parameters of exacerbation. According to the inclusion criteria, CRP was significantly higher on admission in patients with AE-COPD (table 3). Moreover, FEV1 improved significantly from 37.9 (16.8–79.5)% predicted initially to 49 (15.3–79.9)% predicted by discharge in the AE-COPD patients.
Symptoms, medication and C reactive protein levels of study patients
Detection of respiratory viruses
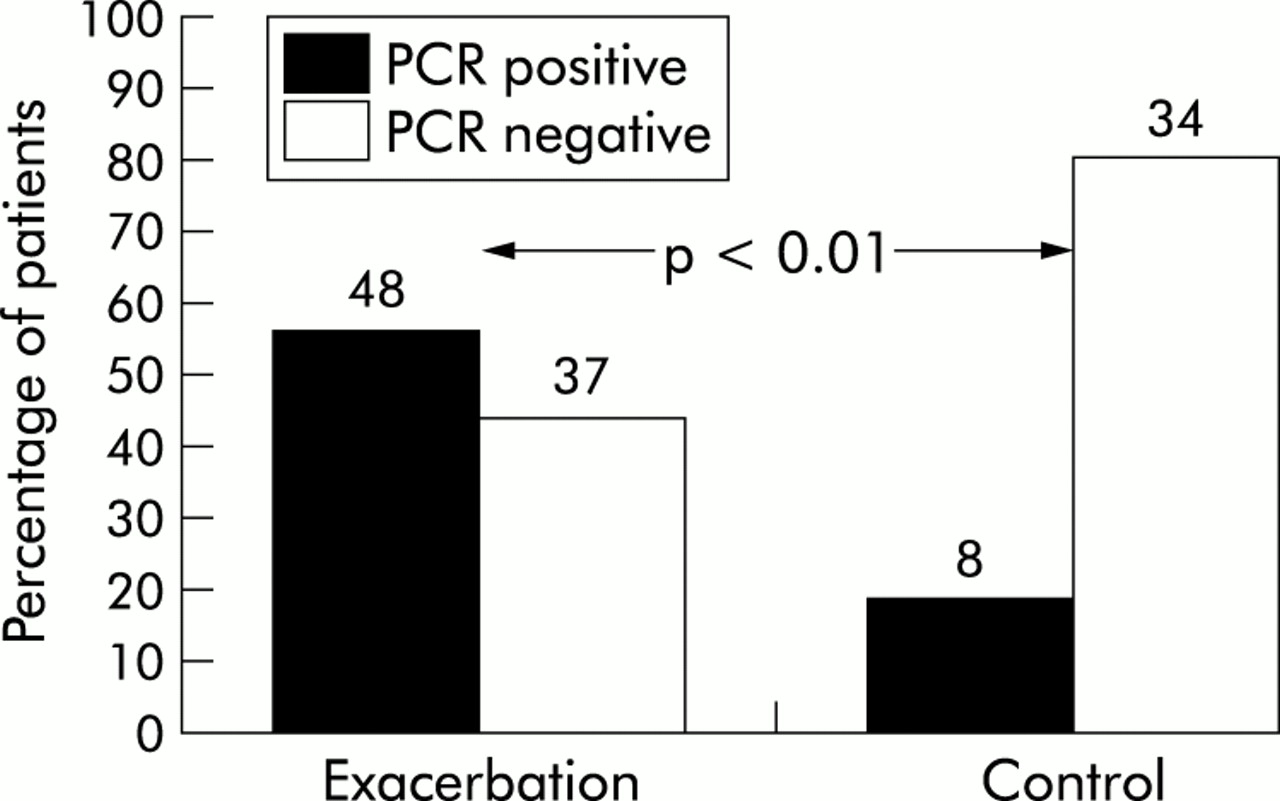
Respiratory viruses were detected in sputum and nasal lavage in 48 (56%) of 85 patients with AE-COPD and eight (19%) of the 42 controls (p<0.01, fig 2). In the 48 patients with AE-COPD 59 viruses were detected and multiple viruses were detected in 10 of the 48 patients (21%). In the patients with stable COPD, nine samples were virus positive with multiple virus isolation in only one of eight patients (13%). The viruses detected are summarised in table 4 according to study group and type of specimen analysed. The most common viruses were picornaviruses, influenza A, and RSV.
Distribution of viruses

{kind=link}
{kind=link}
Detection of respiratory viruses in induced sputum and nasal lavage specimens. Data are percentages of patients; probability according to χ2 test. Absolute numbers are given on top of the boxes. Respiratory viruses were detected more frequently in respiratory specimens from patients with an acute exacerbation of COPD (p<0.001).
Sputum and nasal lavage specimens were analysed separately to determine the preferred site for virus detection. In induced sputum 49 viruses could be detected in 40 of 85 exacerbated patients (47%) compared with only four viruses in four of 42 stable patients (10%, p<0.01). In contrast, in nasal lavage specimens only 32 viruses were detected in 26 of 85 patients (31%) with an exacerbation and seven viruses were detected in seven of 42 patients with stable disease (17%, p=0.14). Comparing the PCR results of the two sites in the AE-COPD group, we found respiratory viruses in 18 of 48 (38%) virus positive patients in both nasal lavage and induced sputum. However, most of the viruses were found only in induced sputum (22/48 (46%) v 8/48 (17%), p=0.01).
Correlation between virus detection and clinical symptoms
The patients with a current exacerbation also reported more exacerbations in the preceding year than the controls (2 (0–12) v 1 (0–8), respectively, p=0.03, table 3). However, virus detection seemed to be unrelated to the number of exacerbations because the frequency was not higher in virus positive subjects (2.5 (0–12) v 2.0 (0–12); p=0.45).
Patients with AE-COPD were admitted to hospital a mean (SD) of 11 (9) days after onset of the first symptoms. Interestingly, patients with viruses in nasal lavage came earlier (8 (12.5) days) than those without viruses in the nasal lavage (12.5 (9.8) days, p=0.05). There were no such differences in patients with or without viruses in induced sputum. In patients with AE-COPD fever was more frequent in those in whom a virus was detected (25%) than in those without detection of viruses (6%, p=0.03). Clinical signs of upper airway infection were not associated with detection of viruses. This was also the case when airway obstruction, as determined by FEV1, was compared between virus positive and negative subjects in the AE-COPD group, although there was a trend to lower FEV1 in the virus positive group. Moreover, no typical clinical pattern could be described for particular viruses.
Drug treatment
Overall, 49 of the 85 patients with exacerbation (58%) and 23 of the 42 patients with stable disease (55%) were receiving treatment with oral corticosteroids (p=0.91) before admission to the hospital. The median (range) dose was 5 (0–80) mg and 5 (0–150) mg (p=0.88), respectively. Similarly, inhaled corticosteroids were used by 65% of the patients with an exacerbation and 55% of patients with stable disease (p=0.37). There were therefore no differences in the frequency of use and dose of corticosteroids—either orally (table 3) or inhaled—and, moreover, there was no association with virus detection (data not shown).
DISCUSSION
The most important findings of this study were: (1) acute exacerbations of COPD requiring admission to hospital are associated with the presence of respiratory viruses in nasal lavage and induced sputum; (2) specimens of the lower respiratory tract used in this study had a higher viral recovery than upper respiratory tract specimens in patients with acute exacerbations of COPD; (3) fever was the only clinical symptom associated with virus detection in specimens of exacerbated patients.
In our 2:1 case-control set up, special care was taken to avoid seasonal selection bias by monthly recruitment of both groups. Both groups were comparable with regard to the distribution of demographic data, general physical condition, and lung function. Because the airflow limitation could not be compared between the two groups at baseline due to the obstructive nature of the AE-COPD, we assessed FEV1 again before discharge as an approximation for baseline in that group. To date there is no widely accepted definition of acute exacerbations of COPD, but most published definitions encompass some combination of three clinical findings: worsening dyspnoea, increase in sputum purulence, and increase in sputum volume.24,29,30 Moreover, patients with AE-COPD in this study had significantly more frequent clinical signs of airway infection than the control group. These symptoms agree with the “minor symptoms” proposed by Seemungal et al19 based on criteria modified from Anthonisen et al.24
The percentage of virus positive samples in our study was high compared with previous reports14–16 because all but two studies19,21 used less sensitive methods than PCR.14,17,18 In addition, previous studies using PCR reported results of only one single virus at a time.19 We believe that the figures are valid and that the presence of viruses in the respiratory tract has been underestimated in previous studies. This is supported by a recent study which found respiratory viruses in nasal aspirates of 39.2% of all exacerbations.21 Moreover, it seems very likely that, if we included further respiratory viruses such as parainfluenza 1 and 2 or adenovirus, the detection rate would have been even higher.
We detected respiratory viruses significantly more often in the AE-COPD group (56%) than in the controls (19%), suggesting that respiratory viral infections may be related to COPD exacerbations. The recently published global initiative for chronic obstructive lung disease (GOLD) stated that infection of the tracheobronchial tract and air pollution are the most common causes of exacerbation.29 In addition, all recently performed trials to prove the efficacy of antibiotic strategies to manage exacerbations of COPD yielded only very limited results.24 It has been suggested on various occasions that viral infections may be highly prevalent in AE-COPD.4 Our data fully support this hypothesis; the most frequent viruses were picornaviruses (36%), influenza A (25%), and RSV (22%). Other studies using viral culture and/or serology found similar distributions of viruses.15,16,31
In addition, this hypothesis was supported by the fact that the difference in the frequency of viral detection between the two groups was almost exclusively based on the results of induced sputum, which reflects more closely the lower respiratory tract. While induced sputum detected respiratory viruses in 47% of the exacerbated patients, we found positive nasal lavage samples in only 31%. This indicates that nasal lavage samples are probably less able to discriminate between patients with and without exacerbated COPD when virus detection is the issue.
Fever was the only clinical sign associated with a positive virus PCR. Because this was a hospital based study, we observed a wide range of days between onset of symptoms and hospital admission. In order to draw final conclusions on the role of viral infection for the development of clinical signs and symptoms, future studies will have to control for the duration between first symptoms and medical contact. Viruses detected by PCR may not always reflect acute infection, but the association between fever and detection of respiratory viruses in patients with an exacerbation indicates a clinically apparent infection.
Patients with AE-COPD had more exacerbations in the preceding year than controls (table 3). This is in agreement with Seemungal and co-workers who found that frequent exacerbations in the previous year were a predictive factor for frequency of exacerbations.3 Nevertheless, there was no correlation between a higher frequency of preceding exacerbations and virus detection.
One possible limitation of this study is that, because of the high sensitivity of the methods used, we also found respiratory viruses in the patients with stable COPD. However, viruses emerge occasionally during the typical virus season without clinical signs of exacerbation. This is in agreement with the findings of Gump et al32 who also found viral infections during periods of remission but more commonly associated with exacerbations. Furthermore, it cannot be ruled out that virus particles remained in the lower respiratory tract from a previous exacerbation, although the patients were in stable disease. It remains an unsolved issue whether viruses recovered from the lower respiratory tract of patients with chronic lung disease indicate infection, colonisation,33 or persistence as has been proposed for adenoviruses.34 This may be a subject of future longitudinal studies.
This case-control study shows that respiratory viruses most probably have a role in exacerbations of COPD. Viral infections seem to have been underestimated in the past, mainly for methodological reasons. Future studies will have to focus even more on the clinical relevance of viral particles in the lower respiratory tract of patients with AE-COPD and investigate possible interventions.
Acknowledgments
The authors would like to thank B Schärling and S Werner (both University Hospital Bergmannsheil, Department of Internal Medicine, Division of Pneumology, Allergology and Sleep Medicine) for assistance in collecting and processing of the samples.
REFERENCES
Footnotes
-
Supported by Bundesministerium für Bildung und Forschung (BMBF) grant #01GC 9802/8.