Article Text

Statistics from Altmetric.com
Concerns about suppression of the hypothalamic pituitary adrenal (HPA) axis by systemic steroids as well as by inhaled corticosteroids have been widely held since their introduction. Several studies have suggested that inhaled corticosteroids can replace oral corticosteroids during exacerbations of asthma1 and in severe asthma.2 We have recently published a study in which treatment of unstable asthmatic patients for 2 weeks with high doses of inhaled fluticasone resulted in a greater improvement in airway hyperresponsiveness than oral prednisolone.3 Additionally—and to our surprise—we found a comparable decrease in serum cortisol levels with fluticasone 1000 μg twice daily and oral prednisolone 30 mg/day. A radioimmunoassay (RIA) method was used to determine serum cortisol suppression in blood with corticosteroid treatment, as in most studies published to date.4,5 However, prednisolone and its metabolites are known to be chemically similar to serum cortisol and might therefore interfere with cortisol measurements by RIA.6 Analytical methods involving chromatographic separation of cortisol from prednisolone and its metabolites, such as high performance liquid chromatography (HPLC), circumvent this problem of interference.
We compared serum cortisol measurements by both conventional RIA and by HPLC in the same study,3 which was of a double blind, double dummy, three arm parallel group design. Patients received either oral prednisolone (30 mg/day), fluticasone propionate 1000 μg twice daily (FP2000), or fluticasone propionate 250 μg twice daily (FP500), both via Diskhaler dry powder inhalation. Measurements at the start of the study and after 2 weeks of treatment were performed at the same time in the morning.
The Gilson ASTED (automated sequential trace enrichment of dialysates) system was used followed by separation with HPLC and detection by UV absorbency.7 The upper and lower limits of measurement were found to be 688 and 6.9 nmol/l, respectively, and the coefficient of variation ranged from 5.6% to 7.0%.
For RIA analysis samples were homogenised and diluted at +60°C. 100 μg 3H (1000 Bq/100 μl) cortisol solution was added to all serum samples after which 0.2 ml of a polyclonal rabbit antiserum was added. The sensitivity of the assay was 15 nmol/l and the coefficient of variation ranged from 5% to 8%.
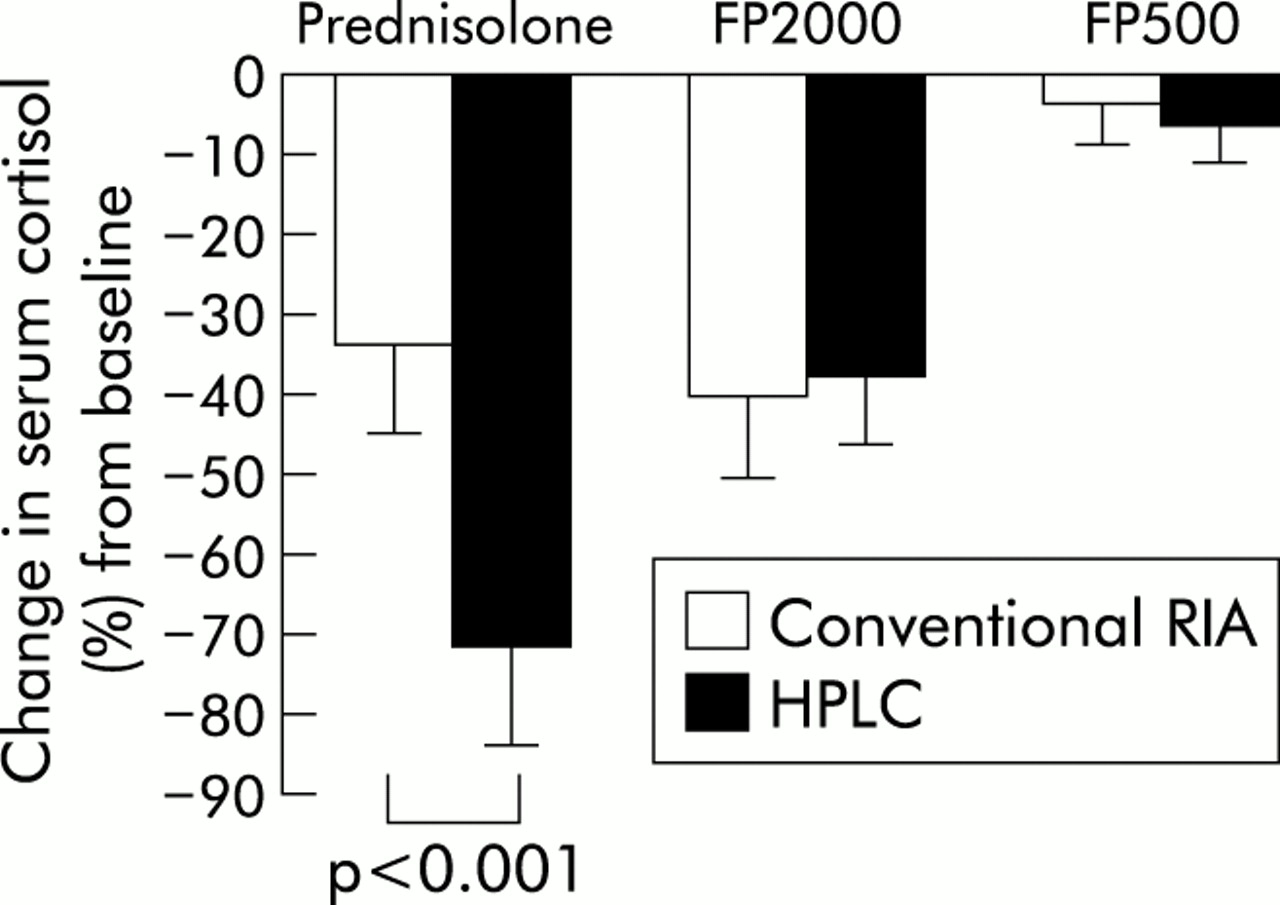
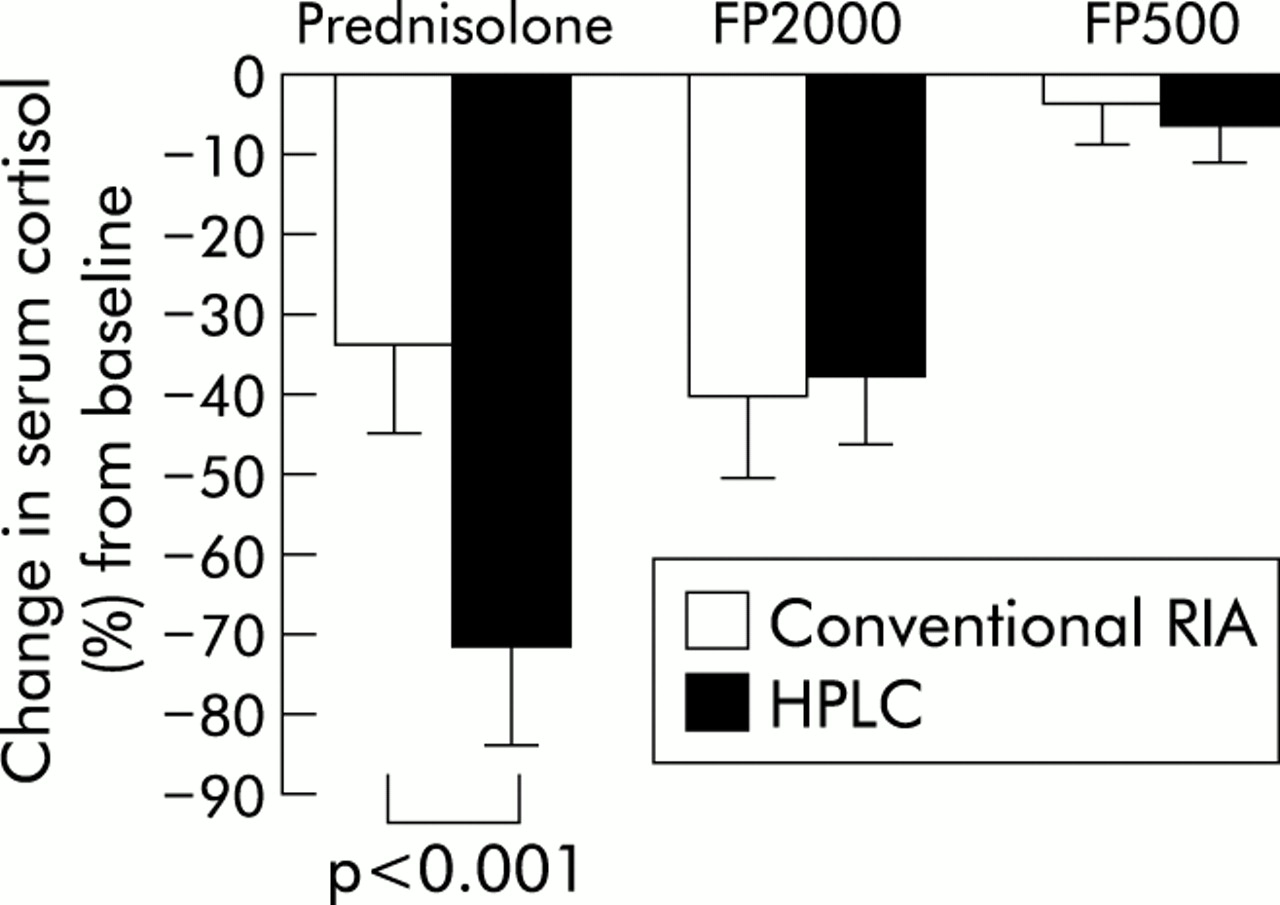
The number of patients with cortisol samples available for both RIA and HPLC was 28 for FP2000, 23 for oral prednisolone, and 33 for FP500. There were no significant differences at baseline between the groups or between the methods of cortisol measurement. Both treatment with FP2000 and with oral prednisolone significantly reduced serum cortisol levels (fig 1), but suppression of serum cortisol in the oral prednisolone group using the HPLC method (–72%) was significantly larger than with the RIA method (–34%, fig 1). As expected, the difference between the cortisol levels measured by RIA and HPLC increased with higher serum prednisolone concentrations (data not shown). The difference is fully explained by the fact that serum prednisolone levels were not separately identified from cortisol by the RIA method. This crossreactivity of prednisolone with cortisol can differ considerably between laboratories and with the RIA method (monoclonal or polyclonal) used, but is always present and ranges from 10% to 100%.3,8–10 There were no significant differences in the change in serum cortisol levels between the HPLC and RIA methods in the inhaled fluticasone groups (FP2000 and FP500).
We conclude that determination of serum cortisol by RIA severely underestimates serum cortisol suppression over a range of 6.9–690 nmol/l serum cortisol in the presence of prednisolone. Our study shows that cortisol suppression in the presence of prednisolone should not be assessed by conventional RIA.
{kind=link}
Change in mean (SE) serum cortisol level (%) from baseline in the three treatment groups measured by conventional radioimmunoassay (RIA) and high performance liquid chromatography (HPLC).