Article Text

Abstract
Much progress has been made in the understanding of nosocomial pneumonia but important issues in diagnosis and treatment remain unresolved. The controversy over diagnostic tools should be closed. Instead, every effort should be made to increase our ability to make valid clinical predictions about the presence of ventilator associated pneumonia and to establish criteria to guide restricting empirical antimicrobial treatment without causing patient harm. More emphasis must be put on local infection control measures such as routine surveillance of pathogens, definition of controlled policies of antimicrobial treatment, and effective implementation of strategies of prevention.
- intensive care
- nosocomial pneumonia
- ventilator associated pneumonia
Statistics from Altmetric.com
Nosocomial pneumonia is the second most frequent hospital acquired infection and the most frequently acquired infection in the intensive care unit (ICU). The incidence is age dependent, with about 5/1000 cases in hospitalised patients aged under 35 and up to 15/1000 in those over 65 years of age.1–3 Death from nosocomial pneumonia in ventilated patients reaches 30–50%, with an estimated attributable mortality of 10–50%.4–9 Increasing microbial resistance worldwide imposes an additional challenge for prevention and antimicrobial treatment strategies.10
In the last two decades efforts have been made to improve the outcome by establishing valid diagnostic and therapeutic strategies. This review will focus on the main controversies in diagnosis and treatment.
DEFINITIONS
Nosocomial pneumonia usually affects mechanically ventilated patients, hence the term “ventilator associated pneumonia (VAP)” is used synonymously. However, nosocomial pneumonia may occur in non-ventilated patients, creating a distinct entity (table 1). Pneumonia may be indicated by, or defined clinically as, the presence of a new lung infiltrate plus evidence that the infiltrate is of an infectious origin such as the new onset of fever, purulent sputum, or leukocytosis (box 1).
Differences in nosocomial pneumonia affecting non-ventilated and ventilated patients (ventilator associated pneumonia, VAP)
Box 1 Definitions of nosocomial pneumonia
Pneumonia acquired after hospital admission at any time (48 hour threshold no longer adequate)
Pneumonia may present as:
early onset pneumonia (<5 days after hospital admission or intubation);
late onset pneumonia (≥5 days after hospital admission or intubation).
The risk of drug resistant microorganisms in late onset ventilator associated pneumonia is associated with:
more than 7 days of mechanical ventilation;
broad spectrum antimicrobial pretreatment.
Dividing patients with VAP into groups with early and late onset has been shown to be of paramount importance.11 Early onset pneumonia commonly results from aspiration of endogenous community acquired pathogens such as Staphylococcus aureus, Streptococcus pneumoniae, and Haemophilus influenzae, with endotracheal intubation and impaired consciousness being the main risk factors.12–15 Conversely, late onset pneumonia follows aspiration of oropharyngeal or gastric secretions containing potentially drug resistant nosocomial pathogens. Only late onset VAP is associated with an attributable excess mortality.9
The definitions of early and late onset VAP have not been standardised. Firstly, the starting point for early onset pneumonia has varied considerably, including time of hospital admission, admission to the ICU, or of endotracheal intubation. If the time of admission to the ICU is chosen as the starting point, patients may already have been colonised in hospital.14,16 In accordance with the American Thoracic Society (ATS) guidelines, we advocate using the time of hospital admission. Secondly, the cut off time separating early and late onset VAP has not been standardised. The ATS suggested using the fifth day after hospital admission.11 We have shown that colonisation of patients after head injury markedly changed between the third and fourth day in favour of nosocomial pathogens.13 Trouillet et al have shown that isolation of drug resistant microorganisms can be predicted by the duration of intubation and antimicrobial treatment17; the cut off between early and late onset VAP used was 7 days.
Traditionally, nosocomial pneumonia is defined as occurring in patients admitted to hospital for at least 48 hours.18 However, this definition is no longer adequate at least for VAP because a significant number of cases occur within 48 hours of hospital admission as a consequence of particularly emergency intubation. In these patients cardiopulmonary resuscitation and continuous sedation were independent risk factors for the development of VAP while antimicrobial treatment was protective.19
ANTIMICROBIAL TREATMENT
Several investigations have addressed the efficacy of antimicrobial treatment as well as its impact on microbial resistance. The immediate administration of treatment is crucial and inappropriate treatment is associated with an increased risk of death from pneumonia.20–22 Moreover, even if the initially inappropriate antimicrobial treatment is corrected according to diagnostic results, there remains an excess mortality compared with patients treated appropriately from the beginning.23
Conversely, antimicrobial treatment is not without risk. Rello and coworkers showed that antimicrobial pretreatment was the only adverse prognostic factor in a multivariate model. However, if pneumonia due to high risk organisms (P aeruginosa, A calcoaceticus, S marcescens, P mirabilis and fungi) was included in the model, the presence of these high risk organisms was the only independent predictor and antimicrobial pretreatment entirely dropped out.20 Thus, antimicrobial treatment is associated with excess mortality due to pneumonia caused by drug resistant microorganisms (fig 1). Furthermore, each treatment regimen exerts a specific selection pressure so that recommendations for initial empirical antimicrobial treatment must accommodate local variations in infecting organisms and their resistance patterns.24–27

Importance of adequate and appropriate antimicrobial treatment.
RISK FACTORS AND PREVENTIVE STRATEGIES
In addition to antimicrobial treatment, several risk factors for VAP can be minimised by simple and inexpensive (although not always easy to apply) preventive strategies. These include the avoidance of intubation and re-intubation by non-invasive ventilation,28,29 orotracheal rather than nasotracheal intubation,30,31 semi-recumbent instead of supine body position,32,33 avoidance of deep sedation and paralysing medication,34 and changing the ventilator circuit not more than once a week35 (table 2). However, many prophylactic measures remain controversial, as reviewed by a recent European Respiratory Society task force on VAP.36
Risk factors for VAP and preventive strategies
DIAGNOSTIC STRATEGIES
Clinical observations, laboratory results, and chest radiographs are of limited value in diagnosing VAP, so great effort has been made to establish independent microbiological criteria. In our view these efforts have so far not succeeded. Despite its limitations, clinical assessment is the starting point for diagnosing VAP and alternative strategies must be interpreted with regard to their ability to decrease the rate of false positive clinical judgments (about 10–25%).36 On the other hand, the 20–40% false negative clinical judgments remain undetected.37 Qualitative tracheobronchial aspiration has a high negative predictive value and a negative culture result in the absence of antimicrobial treatment virtually excludes VAP. Surveillance based on potential pathogens present in patients with suspected VAP is an increasingly attractive tool to direct local empirical antimicrobial policies. Can quantitative culture overcome the limitations of qualitative tracheobronchial aspirates and allow for an individual diagnostic approach to VAP?
The technique of quantitative culture of bronchoscopically retrieved protected specimen brush (PSB) and bronchoalveolar lavage (BAL) specimens has been evaluated by a variety of approaches. Early animal studies established a relationship between histological pneumonia and bacterial loads, but more recent studies have highlighted limitations of quantitative cultures. In ventilated mini-pigs the severity of bronchial and pulmonary inflammatory lesions and bacterial load were clearly associated. However, there was a large overlap, such that threshold bacterial loads could not differentiate between samples from unaffected pigs, those with bronchitis, and those with pneumonia.38 Similarly, in a subsequent study evaluating diagnostic tools, none had a satisfactory diagnostic yield.39
Studies in healthy non-intubated patients have shown a high specificity for PSB and BAL. In mechanically ventilated patients without suspected VAP the results were less impressive, yielding false positive results in 20–30%, although no strictly independent reference was used.40–43 In patients with suspected VAP a variety of diagnostic tools have been evaluated with conflicting results.44–47 These studies provided several general insights, although references and thresholds for the calculation of diagnostic indices varied considerably. Firstly, PSB and BAL had generally comparable diagnostic yields; secondly, tracheobronchial aspirates had comparable yields to PSB and BAL, with a tendency towards a lower specificity; thirdly, all tools exhibited a rate of false negative and false positive results ranging from 10% to 30%. A study focusing on the variability of PSB showed that the qualitative repeatability was 100%, while in 59% of the patients the quantitative results varied more than tenfold.48 Based on these studies, several investigations were performed using post-mortem histological results or lung culture as an independent reference or gold standard.49–55 Despite several important methodological limitations, these studies revealed important clues to the relationships between histology, microbiology, and the diagnosis of VAP: (1) limited correlation between histological findings and the bacterial load of lung cultures; (2) the recognition that no reference would be irrefutable; (3) a surprisingly high rate of false negative and false positive results of 10–50% regardless of the technique used; and (4) a comparable yield of non-invasive and invasive diagnostic tools. Reasons for false negative findings included sampling errors, antimicrobial pretreatment, and the presence of stage specific bacterial loads during the evolution of pneumonia (developing as well as resolving pneumonia). Conversely, false positive results were attributable to contamination of the samples and bronchiolitis or bronchitis, particularly in patients with structural lung disease.
Studies evaluating the influence of diagnostic techniques on outcome have a number of limitations: (1) the usefulness of diagnostic techniques may vary within different populations; (2) this approach ignores the long term effects on microbial resistance; (3) the presence of excess mortality has only been shown for late onset VAP and was low (0–10%) in some studies4–9; and (4) outcome measures are most consistently evaluated when antimicrobial treatment is stopped in patients without positive culture results which, in our view, is unethical.56 Four randomised studies have been published evaluating non-invasive and invasive diagnostic tools, three from Spain57–59 and one from France.60 The Spanish studies found no difference in outcome measures such as mortality, cost, duration of hospitalisation, ICU stay, and intubation. The multicentre French study found a bronchoscopic strategy including quantitative cultures of PSB and/or BAL specimens to be superior to a clinical strategy using qualitative tracheobronchial aspirates in terms of 14 day mortality, morbidity, and use of antimicrobial treatment. Each study had limitations, however, and the results of the French study raise the following concerns: firstly, the clinical strategy did not necessarily reflect routine practice; secondly, it is not clear from the data how the invasive strategy accounted for the better outcome; and, thirdly, the clinical group had a significantly higher rate of inadequate antimicrobial treatment.61,62 In view of these data, we draw the following conclusions:
Quantitative culture cannot confirm a diagnosis of VAP in the individual case.
Non-invasive and invasive bronchoscopic tools have comparable diagnostic yields and share similar methodological limitations.
The introduction of microbiological criteria to correct for false positive clinical judgements does not result in more confident diagnoses of VAP.37
NEW DEVELOPMENTS IN ANTIMICROBIAL TREATMENT
We suggest a change in perspective away from the individual and towards an epidemiological approach, as elaborated in the ATS guidelines.11 These include:
Initial antimicrobial treatment must always be empirical.
Empirical antimicrobial treatment can be guided by three criteria: severity of pneumonia, time of onset, and specific risk factors. All pneumonias acquired in the ICU are severe by definition in the guidelines.
The selection of antimicrobial agents must be adapted to local patterns of microbial resistance.
The diagnostic work up may offer additional clues that must be interpreted in the context of the patient's condition. However, it is generally confined to suggesting potential pathogens and their resistance, which may be particularly relevant when there is no response to empirical antibiotics. It is therefore our practice to use quantitative tracheobronchial aspirates regularly, and bronchoscopy with PSB and BAL in patients who are not responding to treatment (fig 2).

Suggested approach to the management of a patient with suspected VAP. qTBS = quantitative tracheobronchial secretions.
When can antimicrobial treatment be withheld or stopped? Firstly, patients exhibiting signs of severe sepsis or septic shock must receive empirical treatment. Secondly, patients with clinically suspected VAP yielding borderline colony counts (≥102 but <103 cfu/ml in PSB) who were untreated were found to have an excess mortality if they developed significant colony counts within 72 hours.56. We therefore argue that stable patients with clinically suspected VAP but without an established pathogen should also receive empirical treatment.
The dilemma of potential overtreatment at the cost of increased microbial selection pressure could be addressed more satisfactorily if our ability to diagnose pneumonia according to clinical criteria improved. This could be achieved, firstly, by improving the clinical criteria for suspected VAP as those currently in use (a new and persistent infiltrate on the chest radiograph plus one to three of the following: fever or hypothermia, leucocytosis or leucopenia, and purulent tracheobronchial secretions) are outdated. In particular, it is inappropriate to ignore changes in oxygenation, the criteria for severe sepsis and/or septic shock. Pugin et al63 have suggested a scoring system for VAP, including the following six weighted clinical and microbiological variables: temperature, white blood cell count, mean volume and nature of tracheobronchial aspirate, gas exchange ratio, and chest radiograph infiltrates. This score achieved a sensitivity of 72% and a specificity of 85% in a necroscopic study.53 It is tedious to calculate and includes microbiological criteria, but it indicates that criteria may be developed that significantly improve the predictive value of clinical judgment. Similarly, surrogate markers of the inflammatory response associated with VAP could be of help in guiding antimicrobial treatment decisions. Secondly, a validated scoring system may be helpful in deciding when antimicrobial treatment can be safely withheld or stopped. In contrast to community acquired pneumonia,64 severity assessment of VAP has not received much attention.
Another approach to reducing the microbial selection pressure imposed by empirical antimicrobial treatment is to reduce exposure by minimising the duration of treatment. The challenge would be to identify low risk groups without drug resistant microorganisms. In an elegant study by Singh et al65 patients with suspected nosocomial pneumonia (58% VAP) with a Pugin score of ≤6 (low clinical probability of pneumonia) received antimicrobial treatment for 10–21 days at the discretion of the attending physician or a 3 day course of ciprofloxacin. After 3 days treatment was stopped in those still considered to have a low clinical probability, whereas those with a higher Pugin score received a full course of standard antibiotics. The length of time in hospital and mortality did not differ but resistance and superinfection rates were higher in the control group (15% v 39%).
In patients with suspected VAP due to Gram negative pathogens, a controlled rotation of one antimicrobial regimen (ceftazidime) to another (ciprofloxacin) was associated with a significant reduction in the incidence of VAP (12% v 7%), the incidence of resistant Gram negative pathogens (4% v 1%), and the incidence of Gram negative bacteraemia (2% v 0.3%).25 Similarly, controlled rotation of antibiotics including restricted use of ceftazidime and ciprofloxacin over 2 years was associated with a significant reduction in VAP cases from 231 to 161 (70%), of potentially drug resistant microorganisms from 140 to 79 (56%), but with an increase from 40% to 60% of MRSA isolates.26 It should be stressed that these studies do not practise rotation in its strict sense, but simply strategies of controlled antimicrobial treatment. The role of antimicrobial rotation cannot therefore be determined yet, neither as a fixed (or blinded) rotation nor as a flexible (or controlled) rotation based on local microbial and resistance patterns.66
RECOMMENDATIONS FOR EMPIRICAL ANTIMICROBIAL TREATMENT
Based on the ATS guidelines,11 the following recommendations can be made (table 3):
General framework for empirical initial antimicrobial treatment of VAP
-
Patients with early onset VAP and no risk factors: core organisms such as community endogenous pathogens (Staphylococcus aureus, Streptococcus pneumoniae, and Haemophilus influenzae) and non-resistant Gram negative enterobacteriaceae (GNEB, including Escherichia coli, Klebsiella pneumoniae, Enterobacter spp, Serratia spp, Proteus spp) should be appropriately covered.
-
Patients with late onset VAP and no risk factors: potentially drug resistant microorganisms must also be taken into account. This is particularly true when mechanical ventilation is required for more than 7 days and against a background of broad spectrum antimicrobial treatment.17 These include multiresistant MRSA, GNEB, and Pseudomonas aeruginosa, Acinetobacter spp, as well as Stenotrophomonas maltophilia. Although not proven by randomised studies, it seems prudent to administer combination treatment. Vancomycin may be added where MRSA is a concern.
-
Patients with early or late onset VAP and risk factors: treatment is identical to late onset VAP without risk factors, except when Legionella spp is suspected.
The guidelines do not make specific recommendations for non-ventilated patients. Instead, patients not meeting severity criteria are treated as early onset VAP with modifications in the presence of additional risk factors. In our view it would be useful to compare this severity based approach with an algorithm that separates pneumonia in the non-intubated and intubated patient, differentiates early and late onset, and considers the presence of risk factors. This is the direction of the recently published German guidelines for the treatment and prevention of nosocomial pneumonia.67
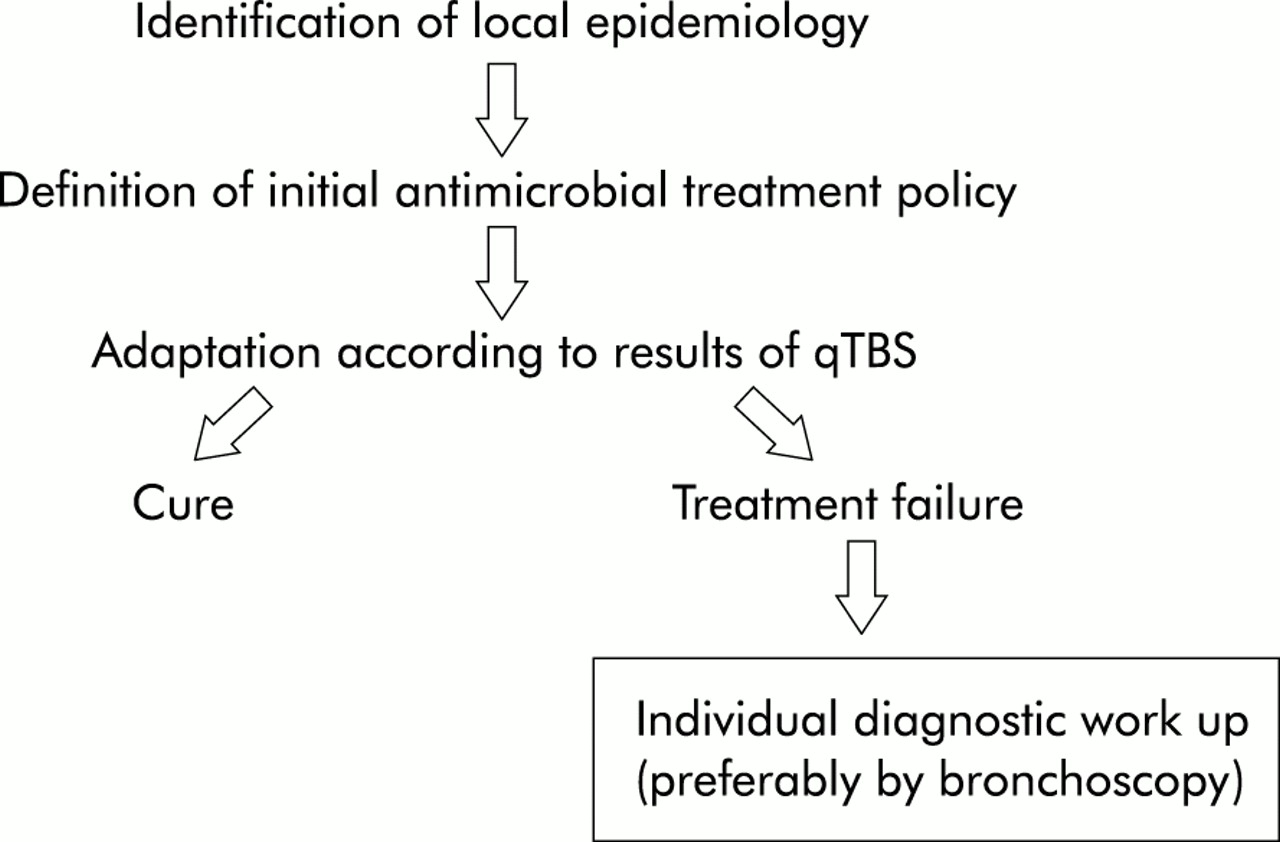
This general framework for empirical initial antimicrobial treatment must be modified according to local requirements. Regular updates of data on potential pathogens of VAP indicating trends in microbial and resistance patterns are mandatory.68 Although data on antimicrobial treatment failures are scarce, we recommend investigating each case. The separate record of these data is particularly useful in detecting patients at risk, as well as microorganisms typically associated with treatment failures. Although few microorganisms are responsible for the vast majority of antimicrobial treatment failures, the distribution of pathogens is widely divergent between centres (fig 3).23,69–71

{kind=link}
{kind=link}
{kind=link}
CONCLUSIONS
Much progress has been made in the understanding of nosocomial pneumonia and this has influenced management guidelines. Nevertheless, important issues in diagnosis and treatment remain unresolved. We argue that the controversy over diagnostic tools should be closed. Instead, every effort should be made to increase our ability to make valid clinical predictions about the presence of VAP and to establish criteria to guide restricting empirical antimicrobial treatment without causing patient harm. At the same time, more emphasis must be put on local infection control measures such as routine surveillance of pathogens, definition of controlled policies of antimicrobial treatment, and effective implementation of strategies of prevention.