Article Text

Abstract
Background: A study was undertaken to evaluate the clinical impact of endoscopic ultrasound guided fine needle aspiration biopsy (EUS-FNA) in patients with mediastinal masses suspected of malignancy.
Methods: From April 1993 to December 1999, 84 patients were referred for EUS-FNA. In all patients CT scanning had shown a lesion of the mediastinum suspected of malignancy located adjacent to the oesophagus. In order to evaluate the clinical impact of EUS-FNA, the history of each patient up to referral for EUS-FNA was reviewed. A board of thoracic specialists was asked to decide the further course of the patient if EUS-FNA had not been available, and this diagnostic strategy was compared with the actual clinical course after EUS-FNA.
Results: For the 79 patients in whom sufficient verification was obtained, EUS-FNA had a sensitivity of 92%, specificity of 100%, PPV of 100%, NPV of 80%, and an accuracy of 94% for cancer of the mediastinum. In 18 of 37 patients (49%) a thoracotomy/thoracoscopy was avoided as a result of EUS-FNA, and in 28 of 41 patients (68%) a mediastinoscopy was avoided. The direct result of the cytological diagnosis obtained by EUS-FNA was that a final diagnosis of small cell lung cancer was made in eight patients resulting in referral for chemotherapy, and in another three patients with benign disease specific treatment could be initiated (sarcoidosis, mediastinal abscess, and leiomyoma of the oesophagus).
Conclusions: EUS-FNA is a safe and sensitive minimally invasive method for evaluating patients with a solid lesion of the mediastinum suspected by CT scanning. EUS-FNA has a significant impact on patient management and should be considered for diagnosing the spread of cancer to the mediastinum in patients with lung cancer considered for surgery, as well as for the primary diagnosis of solid lesions located in the mediastinum adjacent to the oesophagus.
- endoscopic ultrasound
- fine needle aspiration
- mediastinum
- lung cancer
- CT, computed tomography
- MRI, magnetic resonance imaging
- EUS, endoscopic ultrasonography
- EUS-FNA, endoscopic ultrasound guided fine needle aspiration biopsy
- PPV, positive predictive value
- NPV, negative predictive value
- TNM, tumour, node, metastases staging
- SCLC, small cell lung cancer
- NSCLC, non-small cell lung cancer
Statistics from Altmetric.com
- CT, computed tomography
- MRI, magnetic resonance imaging
- EUS, endoscopic ultrasonography
- EUS-FNA, endoscopic ultrasound guided fine needle aspiration biopsy
- PPV, positive predictive value
- NPV, negative predictive value
- TNM, tumour, node, metastases staging
- SCLC, small cell lung cancer
- NSCLC, non-small cell lung cancer
Several techniques are available for obtaining biopsy specimens from mediastinal masses—for example, mediastinoscopy, CT guided biopsy, and transbronchial fine needle aspiration. Each technique has its limitations, either because of small sized lesions or because some areas in the mediastinum are inaccessible for biopsy.
Endoscopic ultrasound scanning (EUS) has become an important adjunct in gastrointestinal endoscopy in recent years in the evaluation of lesions located within the gastrointestinal wall as well as for evaluating extramural disease.1 The combination of flexible endoscopes and high frequency ultrasonic transducers with an image plane orientated longitudinally has meant that EUS guided biopsy specimens can be taken from lesions outlined by EUS.2 Only a few preliminary reports on endoscopic ultrasound guided fine needle aspiration biopsy (EUS-FNA) of mediastinal lesions have been published, and very little is known about the clinical impact of this method.3–,11
The aim of this study was to detail our experience with EUS-FNA in patients with mediastinal masses suspected of malignancy and to evaluate the impact of this method on patient management.
METHODS
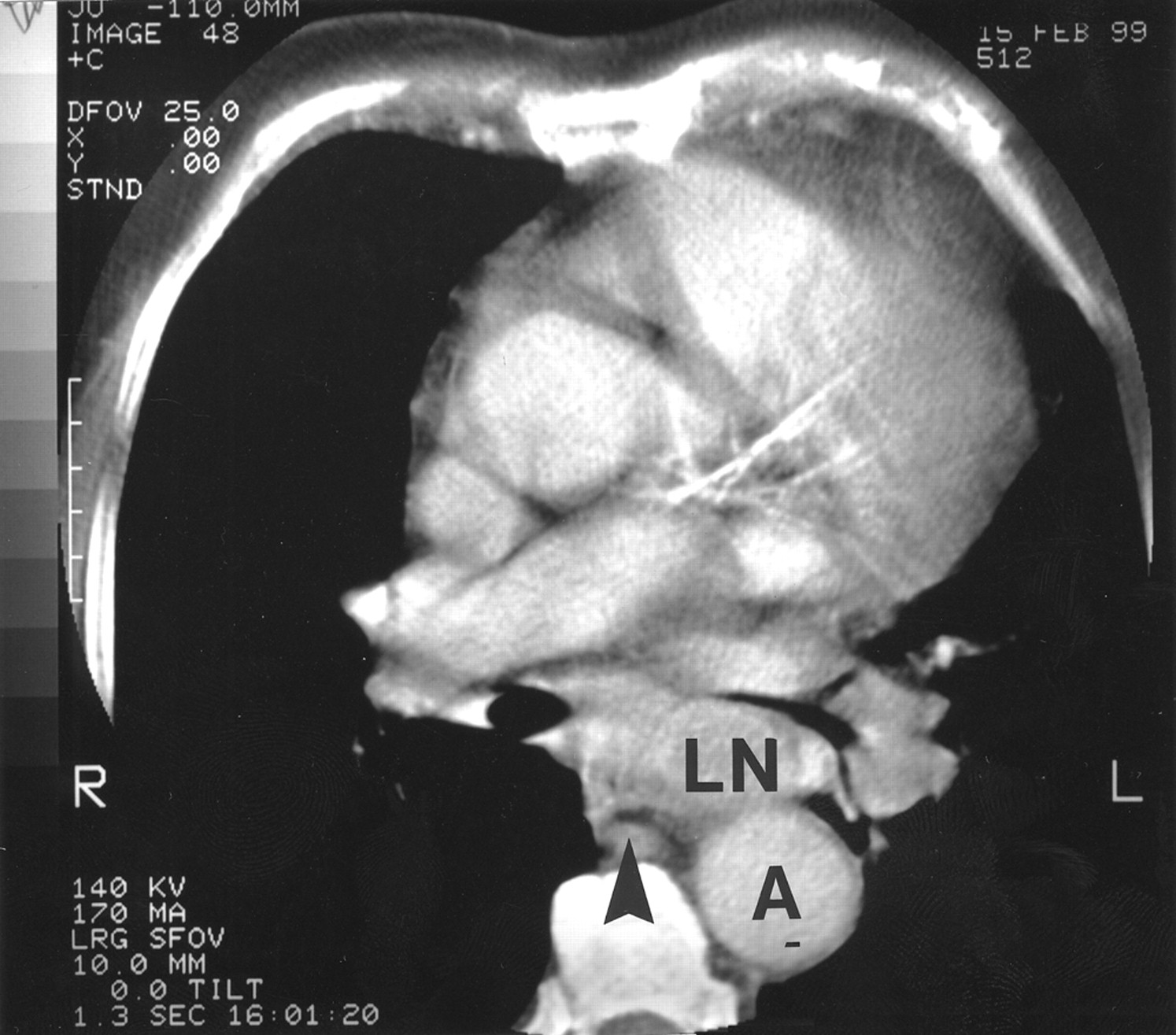
From April 1993 to December 1999, 84 patients referred to the department of cardiothoracic surgery for evaluation of a mediastinal lesion suspected of malignancy were included in the study. There were 36 women and 48 men of mean age 62 years (range 35–82). The inclusion criteria for referral to EUS-FNA were based on CT findings of a suspected lesion of the mediastinum located adjacent to the oesophagus (figs 1 and 2⇓⇓). One group of patients (n=34) had an established diagnosis of lung cancer and mediastinal invasion (stage T4 disease) and/or enlarged lymph nodes (N2 or N3 disease) located adjacent to the oesophagus suspected by CT scanning. Another group of patients (n=50) suspected of malignancy had a solid lesion and/or enlarged lymph nodes of unknown origin outlined by CT scanning located adjacent to the oesophagus.

Chest CT scan showing a central left sided lung cancer with suspected invasion of the mediastinum (aortico-pulmonary window). Arrowhead = oesophagus; A = descending aorta; T = tumour.

Chest CT scan showing enlarged lymph nodes in the mediastinum (subcarinal region). Arrowhead = oesophagus; A = descending aorta; LN = lymph node.
Since the technique of EUS-FNA was developed at our hospital, not all patients who met the inclusion criteria were referred for EUS-FNA, particularly during the early developmental phase before the procedure had been accepted by all the thoracic specialists. All patients referred from the departments of thoracic surgery and pulmonology for EUS-FNA are, however, included in the final analysis. The total number of patients examined for mediastinal malignancy (by all methods) in the study period was approximately 1800 patients.
The study was approved by the ethical committee of Copenhagen County.
Procedure
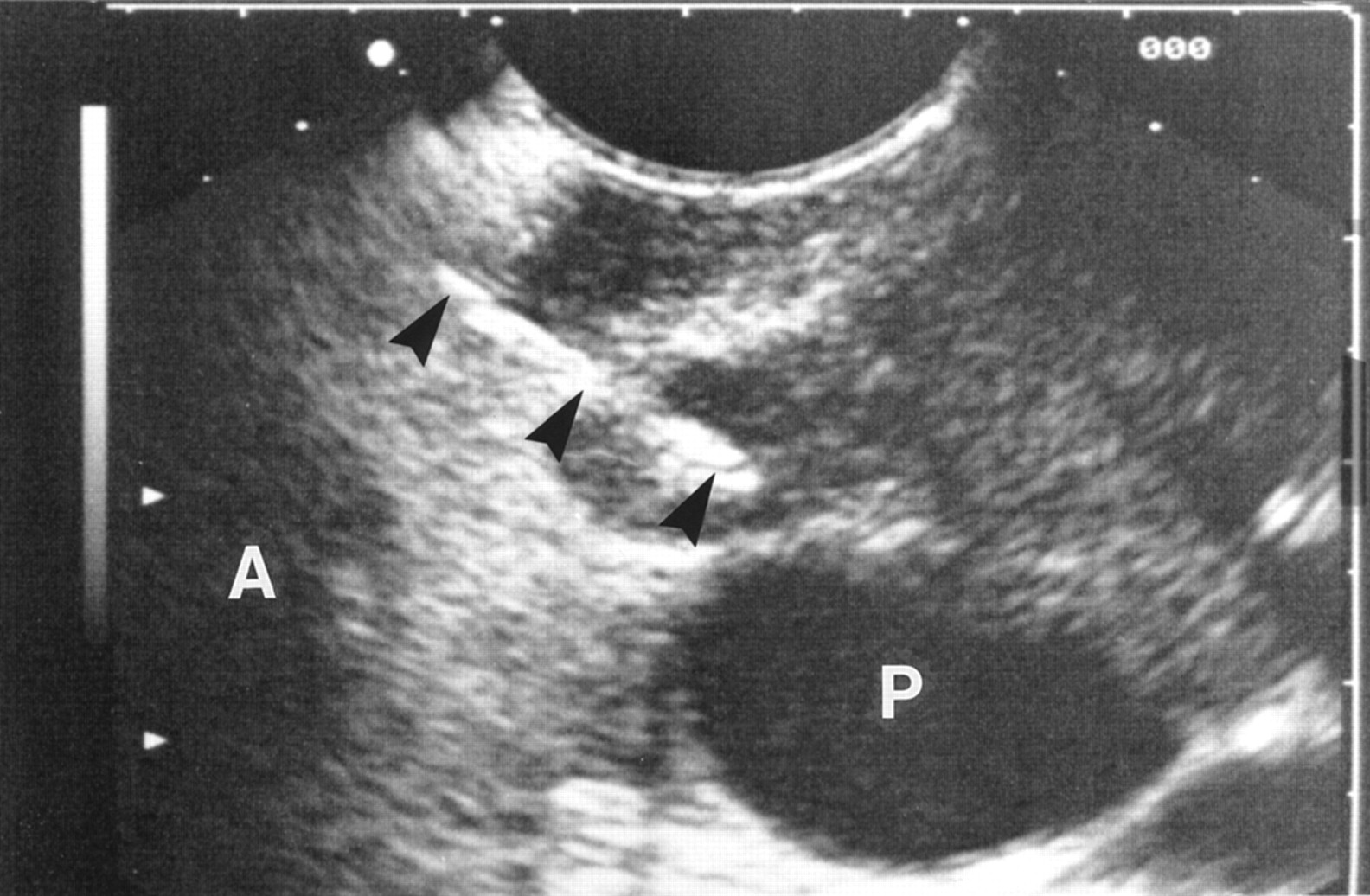
The EUS examination was performed using a flexible echoendoscope with a curved array transducer with an adjustable ultrasonic frequency of 5 or 7.5 MHz and a penetration depth of 7–8 cm (Pentax FG-32 UA, FG-34 UA and FG-36 UA; fig 3⇓). EUS-FNA was performed on an outpatient basis with the patient under conscious sedation using midazolam (Dormicum, Roche). A 22 gauge needle (GIP/MEDI-Globe, type Hancke/Vilmann) was used for the biopsy. EUS-FNA was performed via the oesophagus with 1–3 passes of the needle per lesion (fig 4⇓). The aspirated material was smeared onto glass slides, air dried, and stained for cytological examination. The patients were observed for 1–2 hours at the hospital after the procedure. All EUS-FNA examinations were performed in the department of surgical gastroenterology by one of the authors (PV). Possible complications were recorded up to 1 year after the procedure.
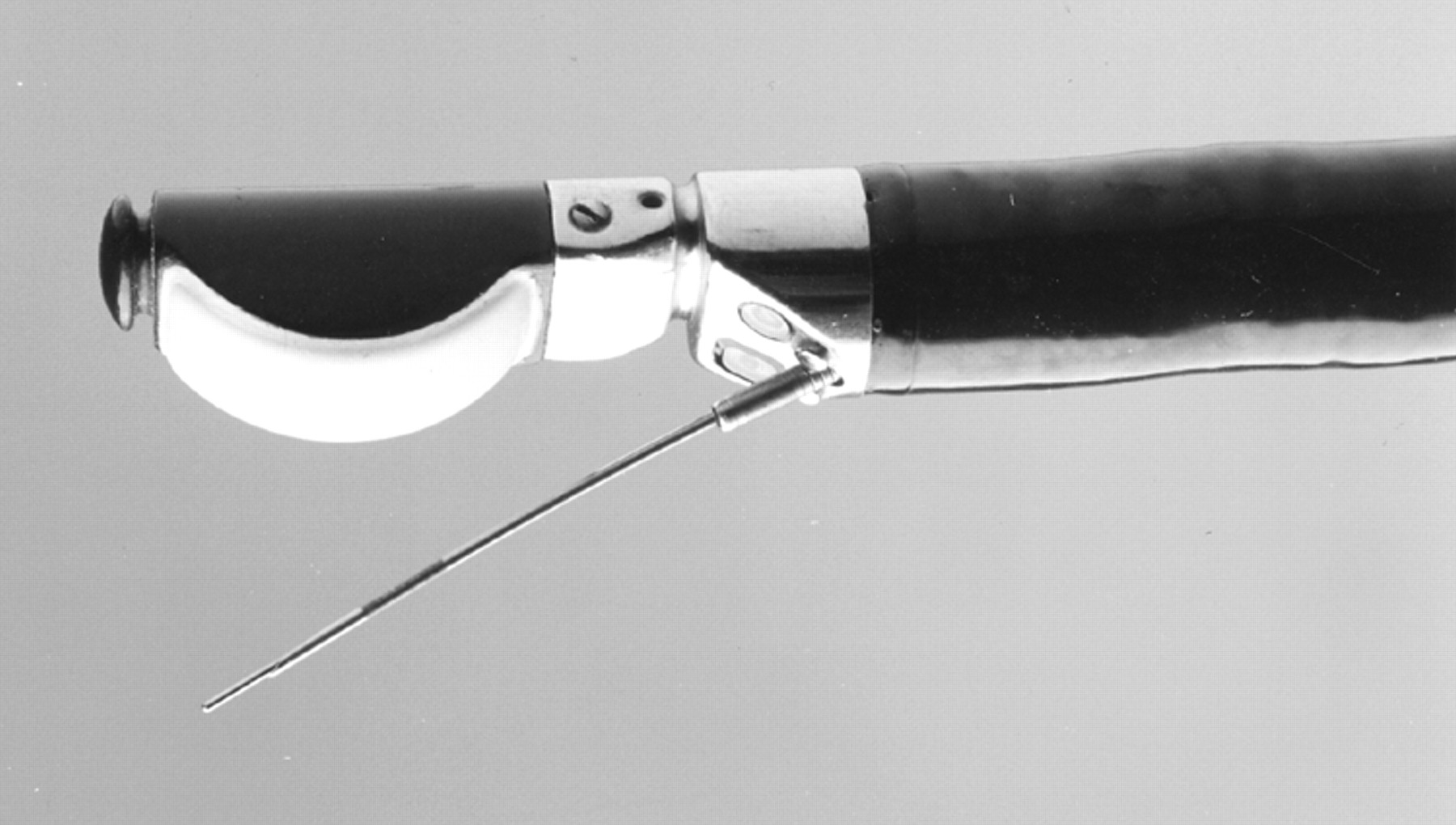
Distal end of an echoendoscope (Pentax FG-36 UA) with biopsy needle.

Ultrasound image demonstrating EUS guided biopsy of an echo poor lymph node at the aortico-pulmonary window. Arrowheads = reflections from needle inside the lymph node; A = aortic arch; P = left pulmonary artery.
The cytological specimens were stained according to the May-Grünwald-Giemsa method. All microscopic examinations were performed by the same pathologist (GKJ).
The EUS-FNA diagnoses were confirmed either by open thoracotomy, mediastinoscopy, or clinical follow up for at least 12 months. In patients in whom thoracotomy was performed, histological proof of advanced disease was always obtained. If cancer spread to the mediastinum was shown by EUS-FNA in concordance with the CT suspicion, a malignant diagnosis obtained by EUS-FNA was taken as final proof of malignancy in the mediastinum. The diagnostic values of EUS-FNA were calculated according to the following definitions:
Sensitivity = true positive EUS-FNA diagnoses/total number of positive final diagnoses
Specificity = true negative EUS-FNA diagnoses/total number of negative final diagnoses
Positive predictive value (PPV) = true positive EUS-FNA diagnoses/total number of positive EUS-FNA diagnoses
Negative predictive value (NPV) = true negative EUS-FNA diagnoses/total number of negative EUS-FNA diagnoses
Accuracy = true negative EUS-FNA diagnoses/total number of final diagnoses + true positive EUS-FNA diagnoses/total number of final diagnoses
In order to study the impact of the EUS-FNA diagnosis on the clinical decision making, the history of each patient was reviewed up to the referral to EUS-FNA. A board of thoracic specialists (MK and JHP) was asked to decide the further course of the patient if EUS-FNA had not been available, and this diagnostic strategy was compared with the actual clinical course after EUS-FNA.
RESULTS
Patients known to have lung cancer before EUS-FNA
The clinical course after EUS-FNA of the 34 patients with known lung cancer is outlined in fig 5⇓. In 18 of these patients (53%) EUS-FNA demonstrated mediastinal involvement either as N2/N3 disease or as T4 disease. SCLC was shown by EUS-FNA in one case who was referred for chemotherapy. The remaining 17 patients were followed and their clinical courses were rapid progression or death from lung cancer in all cases. All of the 18 malignant EUS-FNA diagnoses were recorded as true positive.

Clinical course of 34 patients with known lung cancer prior to EUS-FNA and mediastinal involvement suspected by CT scanning. *Rapid progression or death from lung cancer within 1 year after EUS-FNA. **No sign of mediastinal malignancy within 1 year after EUS-FNA.
In 16 patients with known lung cancer (47%) EUS-FNA of the suspected mediastinal lesion showed that it was benign. Four of these patients went directly to thoracotomy; at surgery three had no sign of mediastinal involvement and were recorded as true negative EUS-FNA diagnoses, while the fourth patient had a positive lymph node by the oesophagus and was recorded as false negative.
In 10 patients with a benign EUS-FNA result a mediastinoscopy was performed and demonstrated no mediastinal malignancy. Seven of these patients underwent a thoracotomy and in six no sign of mediastinal involvement was found. Their EUS-FNA diagnosis was recorded as true negative. The seventh patient had a subaortic lymph node metastasis located at the aortico-pulmonary window and the EUS-FNA diagnosis was recorded as false negative. In the remaining three patients with a benign EUS-FNA and a benign mediastinoscopy the thoracotomy was cancelled for various reasons (one patient refused surgery after the staging procedure had been performed, one had newly diagnosed severe cardiovascular disease, and one developed tumour invasion of the carina discovered on the day of the operation). Since no final diagnosis could be found, these patients were excluded from calculations of the diagnostic value of EUS-FNA.
In the remaining two patients with a benign EUS-FNA result no further invasive procedures were performed, in one patient because of invasion of the carina and in the other because of invasion of a thoracic vertebral body verified by MRI. In both patients the final diagnosis was recorded as inconclusive.
Comparison of the EUS-FNA results with the final diagnoses obtained by thoracotomy or clinical follow up is shown in table 1⇓.
Comparison of EUS-FNA results with final diagnoses obtained by thoracotomy, mediastinoscopy, or clinical follow up in 34 patients with known lung cancer and suspected mediastinal involvement
In the 29 patients in whom sufficient verification was obtained, the diagnostic value of EUS-FNA for mediastinal involvement had a sensitivity of 90%, specificity of 100%, PPV of 100%, NPV of 82%, and an accuracy of 93%.
Patients with unknown disease before EUS-FNA
The clinical course after EUS-FNA of the 50 patients with unknown disease is outlined in fig 6⇓.

Clinical course of 50 patients with unknown disease prior to EUS-FNA and mediastinal malignancy suspected by CT scanning. *Rapid progression or death from mediastinal malignancy within 1 year after EUS-FNA. **No sign of mediastinal malignancy within 1 year after EUS-FNA.
In 36 of these patients (72%) EUS-FNA demonstrated mediastinal malignancy either as N2/N3 disease or as T4 disease. In seven patients cytological examination showed SCLC and they were referred for chemotherapy. The clinical course of the remaining 29 patients was rapid progression or death from mediastinal cancer within a year after EUS-FNA, and all the EUS-FNA diagnoses were recorded as true positives.
In 14 patients cytological examination showed that the EUS-FNA biopsy sample was benign. Six of these patients underwent thoracotomy as the next diagnostic step. One was found to have a para-aortic lymph node metastasis and the EUS-FNA diagnosis was recorded as false negative. The remaining five patients had no sign of mediastinal malignancy at thoracotomy and the EUS-FNA diagnosis was recorded as true negative. One of these patients had a specific diagnosis of leiomyoma of the oesophagus established by EUS-FNA prior to thoracotomy.
Five patients with a benign EUS-FNA result underwent mediastinoscopy. At mediastinoscopy one patient was found to have a malignant lower paratracheal lymph node and the EUS-FNA diagnosis was recorded as false negative. In the remaining four patients the mediastinoscopies found no malignancies. Two of these patients underwent thoracotomy and again no sign of malignancy in the mediastinum was found (true negatives). The remaining two patients had the mediastinoscopy performed before EUS-FNA and in both cases a specific benign diagnosis was established by EUS-FNA (one sarcoidosis, one mediastinal abscess). Both were recorded as true negatives with regard to cancer of the mediastinum.
Three patients with a benign EUS-FNA result were followed without mediastinoscopy or thoracotomy. EUS-FNA demonstrated an unspecified inflammatory disease in two of these patients. Their clinical course was consistent with benign disease and the EUS-FNA was recorded as true negative. The last patient, in whom multiple enlarged mediastinal lymph nodes were evident on the chest CT scan, was found to have Hodgkin's lymphoma in an excised supraclavicular lymph node. The EUS-FNA result of this patient was recorded as false negative.
A comparison of EUS-FNA results with final diagnoses obtained by thoracotomy, mediastinoscopy, or clinical follow up is presented in table 2⇓.
Comparison of EUS-FNA results with final diagnoses obtained by thoracotomy, mediastinoscopy, or clinical follow up in 50 patients with unknown disease suspected of mediastinal malignancy
For the 50 patients with unknown disease before EUS-FNA the diagnostic value of EUS-FNA for mediastinal involvement had a sensitivity of 92%, specificity of 100%, PPV of 100%, NPV of 79%, and an accuracy of 94%.
All patients
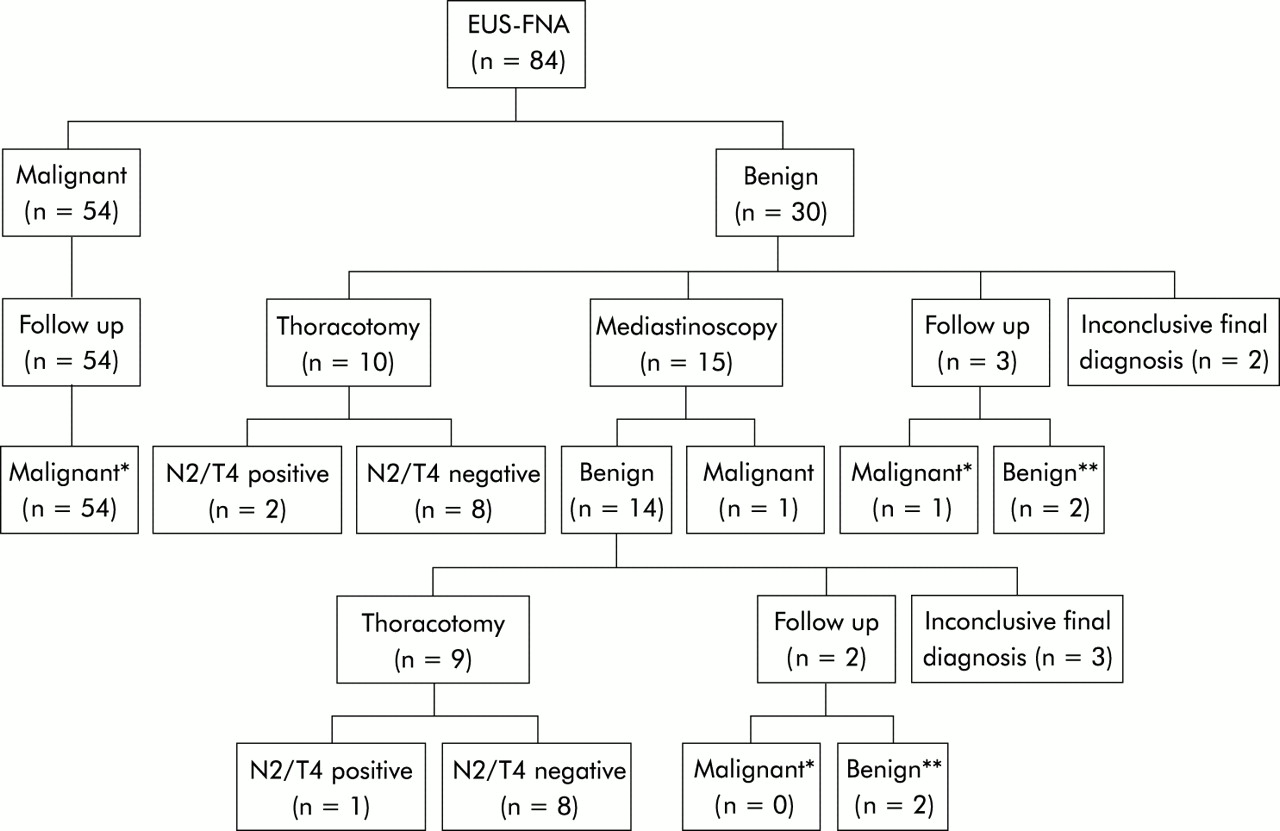
The diagnoses of the 84 patients are shown in table 3⇓ and their clinical course is outlined in fig 7⇓. A comparison of the EUS-FNA results with the final diagnoses obtained by thoracotomy, mediastinoscopy, or clinical follow up is summarised in table 4⇓.
Final primary diagnoses of 84 patients included in the study
Comparison of EUS-FNA results with final diagnoses obtained by thoracotomy, mediastinoscopy, or clinical follow up in all patients (n=84) suspected of mediastinal malignancy

Clinical course of all patients (n = 84) suspected of mediastinal malignancy. *Rapid progression or death from mediastinal malignancy within 1 year after EUS-FNA. **No sign of mediastinal malignancy within 1 year after EUS-FNA.
In 79 patients in whom the final diagnosis could be verified, the diagnostic value of EUS-FNA for cancer of the mediastinum had a sensitivity of 92%, specificity of 100%, PPV of 100%, NPV of 80%, and an accuracy of 94%.
No complications were observed with the EUS-FNA procedures.
Clinical impact of EUS-FNA
In 41 of the 84 patients the next diagnostic procedure would have been a mediastinoscopy if EUS-FNA had not been available (fig 8⇓); 13 mediastinoscopies were actually performed after EUS-FNA. In 37 of the patients the next diagnostic procedure would have been a thoracotomy/thoracoscopy; 19 thoracotomies were actually performed after EUS-FNA. Thus, 28 mediastinoscopies (68%) and 18 thoracotomies (49%) were avoided as a result of EUS-FNA in these selected patients.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagram showing the next diagnostic step if EUS-FNA had not been available, according to a board of thoracic specialists.
The direct result of the cytological diagnosis obtained by EUS-FNA was a final diagnosis of SCLC in eight patients who were referred for chemotherapy, and in another three patients with benign disease a specific treatment could be initiated (sarcoidosis, mediastinal abscess, and leiomyoma of the oesophagus).
DISCUSSION
In the evaluation of patients either suspected of having lung cancer or with an already established diagnosis, the goal is to obtain a tissue diagnosis and/or to classify the cancer according to the TNM classification.
When lung cancer involves the mediastinum, either by direct tumour invasion (T4 disease) or as lymph node metastases (N2/N3 disease), surgery is usually unrewarding.
Chest CT scanning alone is not recognised as proof of N2/N3 disease at our centre because of growing evidence of its poor accuracy (around 80%).11–,13 Mediastinoscopy has until recently been the method of choice if mediastinal tumour growth is suspected by CT scanning. However, the area accessible for mediastinoscopy is limited to the anterior part of the mediastinum. The invasive procedure is performed under general anaesthesia with a complication rate of 2–3%. In 10% of patients who undergo thoracotomy after a negative mediastinoscopy, N2/N3 disease is nevertheless established.14,15 Up to 10% of lung cancer operations result in explorative thoracotomies without tumour resection because the stage of the disease is more advanced than expected preoperatively.16 There is therefore a need for a safer and more accurate diagnostic procedure in patients with a suspected mediastinal tumour growth.
EUS-FNA is a relatively new method first described by our group in 1992.17 Since then several studies have been published and it has been shown that generally all lesions outlined by EUS may be punctured, and even lesions as small as 5 mm may be diagnosed.18 However, there are huge fluctuations in the diagnostic values depending on the site of puncture as well as on the nature of the lesion.2
EUS gives an excellent overview of mediastinal structures, including good access to the paraoesophageal space, the aortico-pulmonary window, the subcarinal region, and the region around the left atrium (levels 4, 5, and 7).19 However, an area anterior to the air filled trachea cannot be visualised.
The patients in this study were referred for EUS-FNA because of suspicious findings on the CT scan. In the evaluation of these patients EUS-FNA demonstrated high diagnostic values comparable to values obtained in other studies.8–,11 Moreover, the study showed that many mediastinoscopies and thoracotomies were avoided because EUS-FNA was used in these selected patients. In 37 of the 84 patients the next diagnostic step would have been open thoracotomy/thoracoscopy, but the results obtained by EUS-FNA spared 18 patients (49%) from this much more traumatic procedure. Above all, the minimal invasiveness of EUS-FNA was recognised as no complications were experienced. We suggest that EUS should precede mediastinoscopy in these patients, and only if EUS-FNA is negative with respect to cancer should a mediastinoscopy be performed. This strategy is strongly supported by a recent cost effective study comparing EUS-FNA with mediastinoscopy in patients with NSCLC. The cost effective advantage conferred by EUS-FNA remained even with an NPV of only 22%.20 In our study the NPV was 80%.
In this study, which included selected patients strongly suspected of mediastinal malignancy based on CT findings, we found it reasonable and in agreement with other studies5–,11 to accept a diagnosis of malignancy obtained by EUS-FNA as final proof of advanced disease. In theory the possibility of “overstaging” by EUS-FNA cannot be ruled out because the exact location of malignancy obtained by EUS-FNA was not verified by open thoracotomy. This is a potential weakness of the present study and may only be resolved by controlled studies where the physician is blind to the EUS-FNA results. Such studies have, to our knowledge, not been published and may be difficult to perform.
Whether EUS-FNA staging of lymph nodes is of benefit in unselected lung cancer patients is still unknown. Further studies should focus on this as well as on a prospective comparison with other staging modalities such as CT scanning, mediastinoscopy, transbronchial biopsy, and positron emission tomography.
In patients with benign disease a specific final diagnosis of sarcoidosis, abscess in the mediastinum, and leiomyoma of the oesophagus was made by EUS-FNA. This experience is in complete agreement with results from other groups performing EUS-FNA.2
In conclusion, EUS-FNA is a safe and sensitive minimally invasive method for evaluating patients with a solid lesion of the mediastinum suspected by CT scanning. It has a significant impact on patient management and should be considered for diagnosing cancer spread to the mediastinum in patients with lung cancer considered for surgery as well as for the primary diagnosis of solid lesions located in the mediastinum adjacent to the oesophagus.