Article Text

Abstract
Background: Over 50% of cases of tuberculosis (TB) in the UK occur in people born overseas, and new entrants to the country are screened for TB. A study was undertaken to determine the prevalence and disease characteristics of pulmonary TB in new entrants to the UK seeking political asylum.
Methods: A retrospective analysis of the results of screening 53 911 political asylum seekers arriving at Heathrow Airport between 1995 and 1999 was performed by studying Airport Health Control Unit records and hospital medical records. Outcome measures were chest radiograph abnormalities, sputum smear, culture, and drug resistance data for Mycobacterium tuberculosis.
Results: The overall prevalence of active TB in political asylum seekers was 241 per 100 000. There were large variations in prevalences of TB between asylum seekers from different regions, with low rates from the Middle East and high rates from the Indian subcontinent and sub-Saharan Africa. The frequency of drug resistance was high; 22.6% of culture positive cases were isoniazid resistant, 7.5% were multidrug resistant (resistant to both isoniazid and rifampicin), and 4% of cases diagnosed with active disease had multidrug resistant TB.
Conclusions: The prevalence rate of TB in political asylum seekers entering the UK through Heathrow Airport is high and more M tuberculosis isolates from asylum seekers are drug resistant than in the UK population. Extrapolating these figures, it is estimated that 101 political asylum seekers with active pulmonary TB enter the UK every year, of whom about 25 would have smear positive disease.
- tuberculosis
- asylum seekers
- mass screening
Statistics from Altmetric.com
The overall incidence rate for tuberculosis (TB) in the UK rose throughout the late 1980s and 1990s and was 10.9 per 100 000 per year in England and Wales according to the results of the 1998 National Tuberculosis Survey (Information from Public Health Laboratory Service Communicable Disease Surveillance Centre, December 1999). The incidence rate in London is higher and increasing faster, reaching 31.2 per 100 000 per year in 1998. Most patients with TB are from ethnic minority communities, with 38% in the Indian subcontinent population and a further 13% in Africans. The 1998 national survey revealed that 56% of TB notifications were in persons born outside the UK, and rates were especially high in recent entrants to the UK. In subjects from the Indian subcontinent the rates in those who had arrived in the UK within the last 5 years were three times higher than in those who had arrived more than 5 years before.
Much of the burden of TB is thus borne by a relatively small proportion of the UK population. Screening of people arriving to live in the UK from areas of the world with high TB notification rates is an important part of the UK's TB control programme. Screening allows early identification of active pulmonary TB which, in turn, reduces transmission rates. Such screening can take place in a variety of ways. The USA and Canada screen for pulmonary TB prior to entry, thus circumventing difficulties associated with screening after immigration. For the UK a similar scheme (the XY form) is available at certain centres in a few countries. However, most TB screening is by the port of arrival system where the immigrant is identified at the port of entry with either immediate referral for investigation or with notification to the Consultant in Communicable Disease Control (CCDC) for the eventual area of residence who initiates investigation and follow up at local chest clinics.
Over the last 4 years 224 305 people intending to live in the UK have been referred to the Health Control Unit (HCU) at Heathrow Airport. Of these, 169 029 were immigrants and 55 276 were political asylum seekers. Many new arrivals have addresses in the UK where they intend to stay; others arrive with no intended address. Political asylum seekers usually lack pre-existing arrangements for residence in the UK and rarely have permanent forwarding addresses at entry, making follow up in the community difficult. For this reason the rate of referral for screening at the port of entry is close to 100%, whereas referral of non-asylum seekers is less complete.
In this study we have used a large sample of all political asylum seekers arriving at Heathrow Airport over a 4 year period to estimate minimum prevalence rates at entry into the country of different groups of political asylum seekers. These rate estimates have then been used to estimate the minimum number of cases of TB in all political asylum seekers in the UK.
METHODS
We established the numbers of political asylum seekers referred to and seen by the HCU over the period 1 April 1995 to 31 March 1999 and recorded the final diagnosis of patients referred to hospitals in North and West London. Political asylum seekers were categorised according to age group, sex, region of origin, smear and culture status, and sensitivity of the isolate of Mycobacterium tuberculosis. The overall numbers of political asylum seekers entering the UK during the 4 year period from 1995 to 1998 (inclusive) were obtained and the prevalence of the disease in the population screened at Heathrow was extrapolated to estimate the numbers of political asylum seekers with TB who enter the UK annually.
Heathrow HCU screening protocol
Referral to the HCU occurs at the discretion of officers of the Immigration Service who take into account areas of the world where the prevalence of TB is high. A threshold of 40 cases per 100 000 was recommended by the 1994 Joint Tuberculosis Committee guidelines and the 1996 Department of Health recommendations for control and prevention at district level. Nearly all political asylum seekers arriving at Heathrow from TB endemic areas are therefore referred to the HCU for medical screening by basic clinical examination and a miniature chest radiograph. If the chest radiograph shows possible pulmonary TB, the subject is either transferred by ambulance to hospital for further investigation or allowed to proceed with his/her immigration process with referral to the CCDC for the area of intended residence. This decision is based on the HCU doctor's judgement of the risk of active TB based on clinical assessment and the radiographic appearances, and the reliability of the forwarding address. All the chest radiographs initially passed as normal are subsequently reviewed by a consultant chest physician. If they are found to be abnormal, the CCDC for the area in which the subject resides is informed and local screening arranged.
Hospital investigation
The details of the diagnostic work up vary from hospital to hospital. Most patients are referred to the regional infectious diseases unit at Northwick Park Hospital where they undergo a repeat chest radiograph, tuberculin test, and microscopy, culture and sensitivities of sputum samples and up to three samples of gastric lavage. Patients with smear negative sputum and gastric washing samples then have a bronchoscopic examination with auramine and Ziehl-Nielsen staining, and mycobacterial culture and sensitivity of the bronchial lavage samples. Patients are diagnosed with active TB if microbiological samples are smear or culture positive, or if the clinical features and radiological appearances strongly suggest active infection in the absence of positive microbiology.
Data collection
Records at the Heathrow HCU covering the period 1 April 1995 to 31 March 1999 were examined to identify all political asylum seekers. The country of origin, age, sex, and chest radiographic result were recorded. Those referred to hospital were identified and their medical case notes were examined to establish the eventual diagnosis, their smear and culture status, and the drug susceptibility of the cultured M tuberculosis. The Research, Development and Statistics Directorate of the Home Office provided numbers according to country of origin of political asylum seekers entering the UK from 1 January 1995 to 31 December 1998.
RESULTS
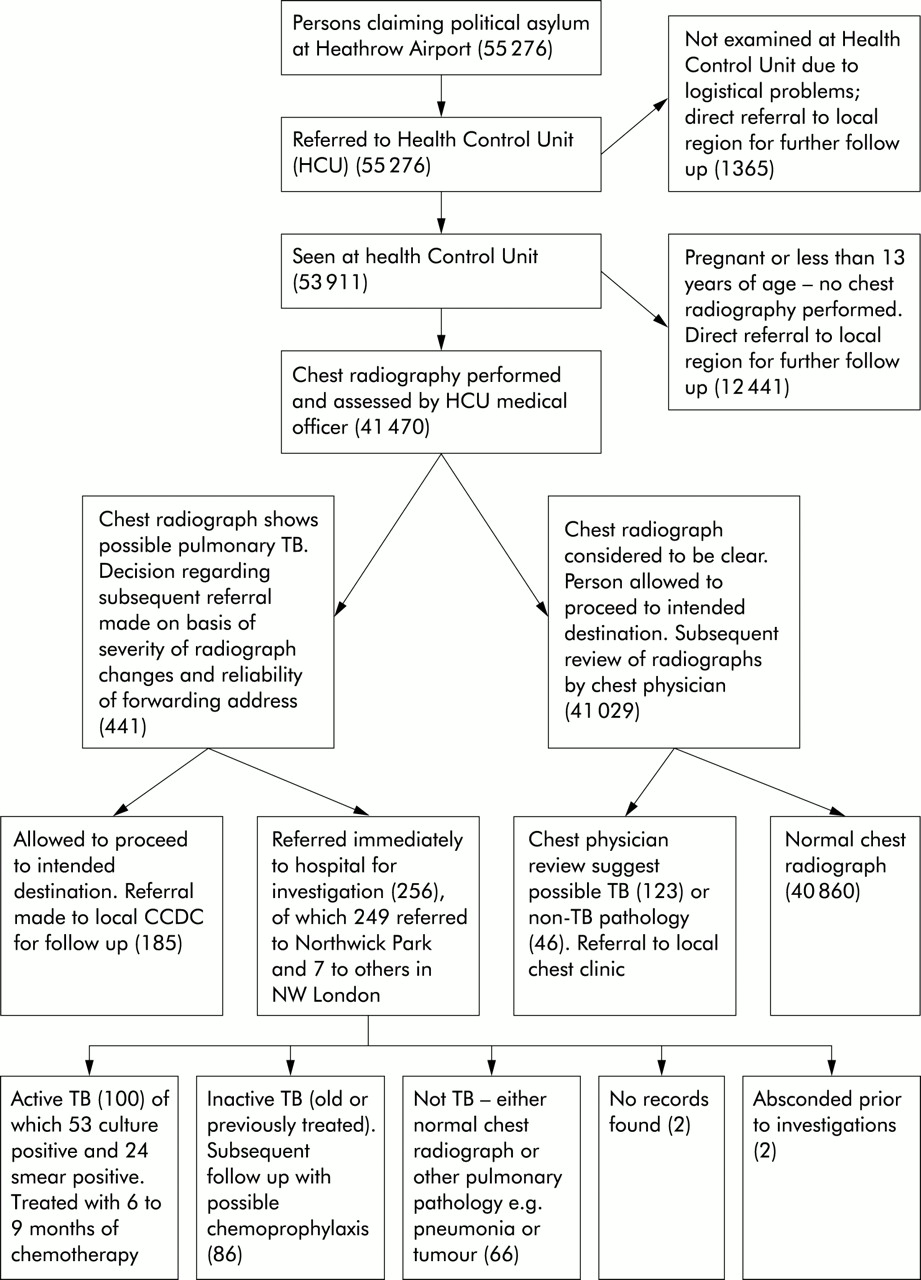
Figure 1⇓ shows the decision tree used. A total of 55 276 political asylum seekers were referred to the Heathrow HCU during the 4 year study period. Logistical problems prevented 1365 from being examined at the HCU, and follow up in the community was arranged. Of the 53 911 seen in the HCU, 696 were pregnant and 11 745 were below the age of 13. These 12 441 asylum seekers did not undergo radiographic examination and were referred to CCDCs for further follow up. A total of 41 470 political asylum seekers therefore received a screening chest radiograph. Most were men (M:F 26 840:14 640) and most were young adults (28 412 aged 13–30, 11 416 aged 31–50, 1642 aged over 51 years). Of the radiographs performed, 441 were considered to be suggestive of pulmonary TB; the remaining 41 029 radiographs were subsequently reviewed by a consultant chest physician and 123 of these were thought to show possible TB. Contact was then made with the appropriate chest clinic via the CCDC to ensure subsequent follow up.

{kind=link}
Flow chart showing protocol of tuberculosis screening programme at Heathrow Airport. Numbers refer to number of political asylum seekers between April 1995 and March 1999.
Of the 441 patients with abnormal chest radiographs, 256 were judged to need immediate hospital assessment and 249 of these (97%) were referred to Northwick Park Hospital. The other seven were referred to other infectious diseases units in North and West London. No records could be found for two patients referred from the HCU, and a further two patients absconded before investigations were completed. Review of the medical case notes of the 252 evaluable patients investigated in hospital revealed a diagnosis of active TB in 100 patients (40%), all of whom were treated with antituberculous chemotherapy for 6–9 months (table 1⇓). M tuberculosis was cultured from 53 of these 100 patients and 24 were smear positive. Twelve (22.6%) of the 53 patients who were culture positive had M tuberculosis resistant to isoniazid, of which four isolates (7.5%) were multidrug resistant TB (MDR-TB), defined as resistance to both isoniazid and rifampicin. The cases of MDR-TB were from Cambodia, Iraq, Lithuania and Somalia, and all four cases were smear positive. One patient had M tuberculosis resistant to streptomycin alone. Eighty six of the 252 patients (34%) were diagnosed as having inactive or previously treated TB and were offered chemoprophylaxis where appropriate. Sixty six of the patients (26%) were found not to have TB at all; the repeat chest radiograph was normal or showed other pulmonary pathology such as bacterial pneumonia or tumour.
Numbers of political asylum seekers with active, culture +ve, smear +ve, and drug resistant TB by region of origin
The prevalence rate of active TB in the political asylum seekers screened at the HCU was 241 per 100 000 for those who received chest radiograph screening (95% CI 196 to 293). Of the 100 patients with active TB, 79 were male and 21 were female equating to prevalence rates of 294 per 100 000 males screened (95% CI 236 to 367) and 144 per 100 000 females screened (95% CI 94 to 219). Analysis by age showed that 65 of the 100 patients were aged 13–30 years, 27 were aged 31–50 years, and eight were aged over 50 years. Calculated prevalence rates for these three age groups were 229 (95% CI 180 to 291), 237 (95% CI 163 to 344), and 487 (95% CI 247 to 958) per 100 000, respectively.
For the subsequent analysis we considered all four years and looked at rates of TB among the political asylum seekers who underwent radiographic examination. Geographical areas and countries showed variations in the prevalence of active disease (tables 1 and 2⇑⇓). Prevalence rates per 100 000 cases of active TB were lower among asylum seekers from Eastern Europe (187), the Balkans (174), and the Middle East (32). The highest prevalence rates per 100 000 were in political asylum seekers from Somalia (1047), Central Africa (565), India (472), and Afghanistan (355). During the period of the study the Home Office statistics that most closely corresponded to our study period (1 January 1995 to 31 December 1998), showed that 152 120 people claimed political asylum in the UK. We used the prevalence in each region of our screened population, extrapolated to all political asylum seekers in the UK as a whole, to estimate that 406 (95% CI 313 to 496) political asylum seekers entering the country during the 4 year study period would have been predicted to have active pulmonary TB, of whom 99 (95% CI 54 to 142) would have smear positive disease (table 2⇓).
Estimated cases of active and smear positive pulmonary TB in political asylum seekers entering UK from 1995 to 1999 extrapolated from Heathrow figures
DISCUSSION
This study is the first to estimate prevalence rates of TB in political asylum seekers arriving in the UK and is based on a large sample of over 41 000 subjects. Because we only have outcomes for the 252 cases referred directly from Heathrow HCU to hospital, our data almost certainly underestimate the prevalence of TB in this group. We have no information about the 117 asylum seekers who were allowed to proceed to their destination with local follow up or the 123 abnormal chest radiographs that were picked up on subsequent review. It is likely that at least some of the political asylum seekers who were not referred to hospital had active TB, though their chest radiograph abnormalities would have been less convincing than those referred directly to hospital. In addition, some might have had extrathoracic TB. We have no data on this but, according to the national tuberculosis survey conducted by the PHLS in 1998, 38% of TB in the UK is extrapulmonary and is thus not detectable by radiographic screening.
Of the 100 patients with active disease, 53% were culture positive which closely matches the results of the 1998 national survey in which 54% of patients with active TB had positive culture results. However, the incidence of drug resistant disease is far higher than in the 1998 national survey in which 4.9% of culture positive cases were resistant to isoniazid and 0.8% were MDR-TB compared with 22.6% and 7.5%, respectively, in our survey. Compared with the UK in 1998, there was a significantly higher risk of an asylum seeker being resistant to isoniazid than an indigenous case (relative risk 4.6, 95% CI 3.0 to 5.9). Political asylum seekers were also significantly more likely to have MDR-TB (relative risk 4.0, 95% CI 1.25 to 8.75).
Despite the relatively high prevalence rates in political asylum seekers arriving at Heathrow Airport compared with average rates for the UK, the actual number of cases detected only represents a small proportion of annually notified cases (less than 0.5%). Furthermore, while the rates of MDR-TB were almost 10 times higher than in the UK population, only one case of MDR-TB was detected per year of the study period.
One important finding of our study was the difference between the prevalence of active disease in asylum seekers from various geographical regions. Those from the Middle East (an area of the world considered by the WHO to have a high prevalence of TB) had a prevalence of TB of 32 per 100 000 which is similar to the annual notification rate for London as a whole (31.2 per 100 000) and considerably lower than that for certain London boroughs such as Newham, Brent, and Tower Hamlets (79, 77, and 77 per 100 000, respectively).1 By contrast, political asylum seekers from sub-Saharan Africa had very high rates of active TB with those from Somalia having the highest prevalence rate (1047 per 100 000).
Assuming that the political asylum seekers presenting to Heathrow are representative of asylum seekers nationwide, we calculated that there would have been 406 cases of active TB in asylum seekers nationally over the 4 year study period of which 99 would have been smear positive. However, there are weaknesses in these assumptions. Some asylum seekers claim political asylum only after they have been resident in the UK for some time, and they may differ in social and economic characteristics from the group claiming asylum at entry. Our data also showed variations in the prevalence of TB among different age and sex groups, and the data provided by the Home Office did not include details of age and sex.
Only two previous reports have specifically studied TB among political asylum seekers. Van den Brande et al2 screened asylum seekers on a voluntary basis at the Central Transit Centre in Brussels during 1993 and calculated a prevalence of 396 cases of active disease per 100 000 subjects screened with chest radiographs. However, there was a high drop out rate during this voluntary programme, and the authors advised that screening of political asylum seekers entering Belgium should be mandatory and that follow up of the screened cases should be regulated. Kesseler et al3 performed a similar voluntary screening project study in North Rhine, Westphalia between 1992 and 1994. They performed chest radiographs on 4058 political asylum seekers and found 48 cases of active tuberculosis (prevalence rate 1183 per 100 000). They too recommended compulsory chest radiographs shortly after arrival with subsequent regulated treatment or prophylaxis programmes.
A number of other studies have looked at the prevalence of pulmonary TB in persons newly arrived in Europe and North America (table 3⇓). Bonvin et al4 studied 4512 immigrants to Switzerland between 1988 and 1990. Of 2469 who underwent chest radiography, 238 had a radiograph suggestive of TB and, after investigation, 55 were considered to have active TB (2228 per 100 000 for the population screened).
Previous studies of TB in immigrant and asylum seeking populations entering European countries.
Two studies in the UK5,6 have examined screening of immigrants, not specifically political asylum seekers, using the port of arrival system. Hardie and Wilson5 estimated that only 36 000 (26%) of the 140 000 immigrants arriving in the UK annually were traced and screened and, of the 20 000 who had chest radiographs, 100 per 100 000 were found to have active TB. Ormerod's review of screening in the Blackburn area6 found that the port of arrival system failed to identify 60% of new immigrants.
Political asylum seekers and other immigrants differ in a number of ways, and this is reflected in differences in the criteria used by immigration officers to refer them to the port health control units. Whereas it is policy to refer political asylum seekers whenever possible, other immigrants are referred on the basis of country of origin and intended length of stay. Political asylum seekers tend to either have no forwarding address or one is only obtained after a number of weeks or months. They will more often live in shared accommodation and, because of cultural differences and a fear of deportation, may be more reluctant to seek medical help. Transmission of TB is by prolonged close contact. For this reason, political asylum seekers with TB pose a risk primarily to other asylum seekers and those in the new entrant community. When considered with the significantly higher risk of drug resistant disease in political asylum seekers with TB, this underlines the importance of primary screening for TB in this population in order to ensure that they receive appropriate treatment and that others in the immigrant community are protected.
Screening of political asylum seekers arriving at Heathrow Airport between 1995 and 1999 yielded a diagnosis of pulmonary TB in at least 241 per 100 000 of those who underwent radiography, which is a prevalence 22 times higher than the annual incidence rate for the UK as a whole (10.9 per 100 000 in 1998). The true burden of TB among political asylum seekers is almost certainly higher, as non-respiratory TB is not detected by chest radiography and because follow up information was only available for 252 of the 564 cases identified by radiographic abnormalities.
Acknowledgments
The authors thank the staff at Heathrow Airport Health Control Unit and Northwick Park Infectious Diseases Unit for their help in collecting the data, especially Professor G Pasvol, Dr RA Wall, and Northwick Park Hospital Audit Department.
Footnotes
All authors contributed equally to the idea of the study and substantially to the writing of the paper. ST and JB collected the data from Heathrow. MC was responsible for the hospital data and performed the data analyses. RD is guarantor for the study.
Funding: None.
Conflict of Interest: None.