Article Text

Abstract
Background: Pulmonary hypertension is a common complication of chronic obstructive airways disease (COPD) and its presence implies a poor prognosis. However, it is difficult to measure and its specific contribution to symptoms is difficult to quantify. A micromanometer tipped pulmonary artery catheter was used to measure pulmonary artery pressure (PAP) during sleep and on exercise.
Methods: Ten patients (five with COPD receiving long term oxygen therapy and five normal individuals) were studied. Pulmonary artery pressure was recorded continuously during two periods of sleep (breathing oxygen followed by air for the COPD group) and during exercise.
Results: In the COPD group PAP during sleep on oxygen was significantly lower than PAP during sleep breathing air (mean (SD) difference 9.6 (5.3) mm Hg, 95% CI 4.9 to 14.3, p= 0.016). PAP during exercise was not significantly different from PAP during sleep breathing air (mean (SD) difference 0.8 (8.9) mm Hg, 95% CI –7.0 to 8.6, p= 0.851). In normal individuals the group mean (SD) PAP was 15 (5.9) mm Hg for the first nocturnal period and 15 (5.7) mm Hg for the second nocturnal period. PAP during exercise was not significantly different from PAP during sleep breathing air (mean (SD) difference 3.3 (2.2) mm Hg, 95% CI 1.1 to 5.5, p= 0.061).
Conclusion: In patients with COPD, PAP rose significantly during sleep to levels similar to those measured during exercise, but this could be reversed with oxygen.
- chronic obstructive pulmonary disease
- sleep
- pulmonary artery pressure
Statistics from Altmetric.com
Pulmonary hypertension is a common complication of chronic obstructive pulmonary disease (COPD) and, when severe, implies a poor prognosis.1 Because the signs and symptoms of the underlying illness can be overwhelming and accurate measurement of pulmonary hypertension requires a cardiac catheter, it is often difficult to diagnose and quantify secondary pulmonary hypertension and its role in the morbidity of COPD is poorly understood. Pulmonary artery pressure (PAP) may rise during sleep or exercise in patients with COPD.2,3 When this rise on exercise is excessive, the future development of resting pulmonary hypertension is likely.4 It has been shown that other routine daily activities are associated with a reduction in oxygen saturation in patients with COPD but normal resting saturations,5 but the haemodynamic significance of this is more difficult to quantify. Conventional measurement of PAP is difficult during sleep, exercise, or in ambulant patients because of the nature of conventional fluid filled pulmonary artery catheters and, in particular, their dependence on external transducers. We have previously used a micromanometer tipped pulmonary artery catheter and data recording system to make continuous PAP recordings in patients with pulmonary hypertension secondary to connective tissue disease.6
We hypothesised that this system might also provide accurate measurements of PAP during daily activity, sleep, or exercise in patients with COPD, providing information about the total haemodynamic burden faced by these individuals.
METHODS
Patients and measurements
Ten subjects (five men) of mean (SD) age 61 (8) years (range 43–69) were studied. Five patients had COPD defined as irreversible airflow obstruction determined by lung function testing (table 1) and were receiving long term oxygen therapy (LTOT) and five were normal. The latter group was referred with suspected pulmonary hypertension, usually because of misleading screening investigations (such as overestimation of PAP by echocardiography) or because of a strong clinical suspicion of pulmonary hypertension despite normal non-invasive tests. In this group, where our own screening investigations were normal, we measured ambulatory PAP to exclude exercise induced pulmonary hypertension. All patients were referred to our unit for further investigation of suspected pulmonary hypertension and all underwent conventional cardiac catheterisation with fluid filled Swan-Ganz catheters followed by monitoring of ambulatory PAP with a high fidelity micromanometer tipped catheter.
Demographic data, lung function, and resting haemodynamics of patients with COPD and normal controls
The normal subjects were defined as those in whom there was no evidence of COPD or of pulmonary hypertension, neither in the cardiac catheterisation laboratory nor after 24 hours of ambulatory PAP monitoring. All patients in the normal group had normal lung function and oxygen saturations when measured in our laboratory.
Pulmonary artery pressure was continuously measured in both groups during sleep in two 4-hour periods, from midnight to 04.00 hours and from 04.00 hours to 08.00 hours. The COPD group was given continuous oxygen at their usual flow rate for the first period and remained off oxygen for the second period. Ward nursing staff were asked to confirm that the patients were asleep at the stated times. Baseline PAP values refer to those recorded while the subject was asleep breathing air as this was the state against which the effect of interventions on PAP were measured.
Written informed consent was obtained for all patients. The study was approved by the West Glasgow Hospitals University NHS Trust ethics committee.
The catheter
This has been described in detail elsewhere.7 Briefly, it is a 7F solid micromanometer tipped catheter (Gaeltech Ltd, Dunvegan, Isle of Skye) which can be zeroed in situ. This is carried out by injecting 0.4 ml of air into a luer fitting on the end of the catheter, causing a pressure of approximately 124 mm Hg to be applied to both sides of the transducer so that a high and equal pressure is applied to both its surfaces, thus restoring its zero state. This creates a calibration line which can be identified on the pressure trace. After removal from the subject the catheter tracing is checked against a known pressure using a sealed chamber and a sphygmomanometer. This value is then used in the analysis programme as a further mechanism to correct any drift which may have occurred in vivo.
Exercise testing
All patients exercised while breathing air using the Sensormedics V-Max system (Sensormedics, Yorba Linda, CA, USA) wearing an adult facemask (Hans Rudolph, Kansas City, MO, USA). The electromagnetically braked cycle ergometer was chosen over the treadmill because it is safer and can maintain a given work rate despite fluctuations in the frequency of pedalling. A steady state workload of 30 watts was chosen because this was felt to be manageable for all the patients with COPD.
Data analysis
The analysis programme (Gaeltech, Isle of Skye, UK) permits PAP tracings to be matched accurately with periods of activity. Mean pressures were derived from the recorded pressure waveform in a novel manner. Single point pressures were recorded at a rate of 32 samples per second for the area indicated by the observer on the pressure trace. The area under the curve was calculated and averaged over the period of time indicated by the observer. This method of calculation for mean pressure was employed in the initial design of the catheter because it provides a mathematical mean of all pressures. This is more accurate when information is necessarily derived from a physiological measurement such as the pressure trace. Mean PAP during sleep was measured for the middle two hours of each nocturnal period. Exercise PAP measurements were the average mean pressure recorded over 1 minute from the onset of the 4th minute of steady state exercise.
Statistics
All data are expressed as mean (SD) with 95% confidence intervals (unless otherwise stated). Statistical testing was by paired t test. A p value of <0.05 was considered to be statistically significant. Statistical analyses were carried out using the oxstat package for personal computers (oxstat II, Microsoft Corporation).
RESULTS
COPD group
Mean PAP during sleep
Group mean (SD) PAP was 60 (8.1) mm Hg during sleep breathing air and 51 (5.5) mm Hg breathing oxygen (table 2). PAP during sleep on oxygen was significantly lower than PAP during sleep breathing air (mean (SD) difference 9.6 (5.3) mm Hg (95% CI 4.9 to 14.3), p=0.016; fig 1, table 2).
Mean (SD) pulmonary artery pressure (PAP) in mm Hg in patients with COPD and normal subjects during rest and exercise

Mean pulmonary artery pressure (PAP) in normal subjects and patients with COPD. Mean PAP for the COPD group and the control group is shown during each activity. For the COPD group PAP was significantly lower when breathing oxygen than when breathing air (*p<0.05).
Mean PAP during exercise
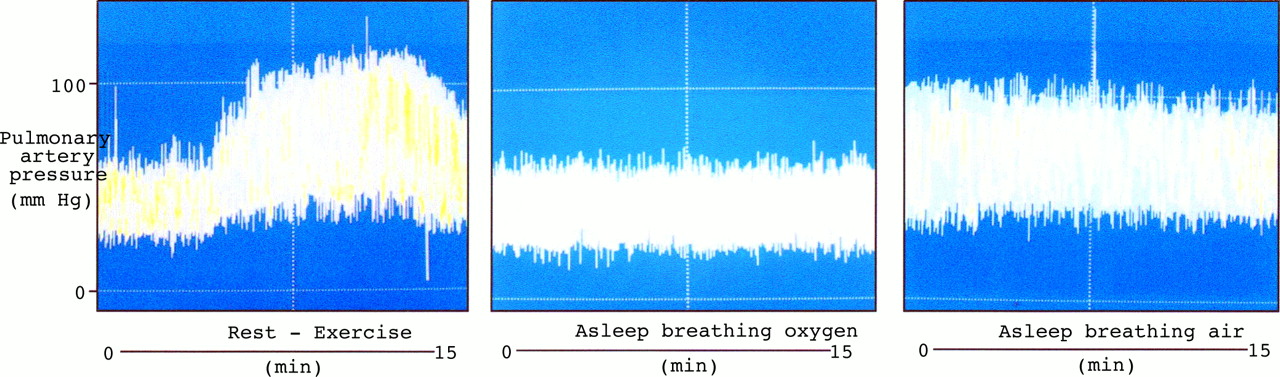
Group mean (SD) PAP during exercise was 59.0 (10.7) mm Hg, which was not significantly different from PAP during sleep breathing air (mean (SD) difference 0.8 (8.9) mm Hg (95% CI –7.0 to 8.6), p=0.851 (table 2, fig 1). An example of an ambulatory PAP trace in a patient with COPD during rest followed by exercise, during sleep breathing air, and during sleep breathing oxygen is shown in fig 2.

{kind=link}
{kind=link}
Ambulatory pulmonary artery pressure (PAP) trace in a patient with COPD. PAP tracings from a single patient with COPD during rest followed by exercise (left panel), during sleep breathing air (centre panel), and during sleep breathing oxygen (right panel). The rise in PAP during sleep breathing air is similar to that recorded during steady state exercise at 30 watts. Breathing oxygen abolished this rise during sleep.
Normal group
Mean PAP during sleep
Group mean (SD) PAP in the normal group was 15 (5.9) mm Hg for the first nocturnal period and 15 (5.7) mm Hg for the second nocturnal period (table 2, fig 1).
Mean PAP during exercise
Group mean (SD) PAP in the normal group during exercise was 17.0 (4.0) mm Hg (table 2), which was not significantly different from PAP during sleep breathing air (mean (SD) difference 3.3 (2.2) mm Hg (95% CI 1.1 to 5.5), p=0.061, table 2, fig 1).
Comparison between COPD and normal groups
PAP while asleep on oxygen v asleep on air for the COPD group was significantly different from asleep on air for the normal group (mean (SD) difference 7.6 (5.6) mm Hg (95% CI 2.7 to 12.5), p=0.039).
Exercise v asleep on air for both groups was significantly different (mean (SD) difference 5.0 (2.7) mm Hg (95% CI 2.3 to 7.7), p=0.034).
DISCUSSION
In this study we have shown that patients with COPD receiving LTOT tolerate invasive haemodynamic assessment, including ambulatory PAP monitoring, and can safely perform cardiopulmonary exercise testing at a low workload. The number of patients presented is small because of difficulties encountered in recruiting frail patients in respiratory failure for invasive haemodynamic monitoring but, nevertheless, we found significant changes in haemodynamics.
Previous studies of PAP in patients with COPD have shown that values are modestly increased and progression slow.8 However, most of these measurements have been of resting pressure which has been shown to be of relatively poor prognostic value.9 Furthermore, it has also been shown that even routine daily activities in patients with mild COPD and normal resting oxygen saturations are associated with reductions in oxygen saturation.5
In this study we have measured PAP in a variety of situations in patients with respiratory failure receiving LTOT and the higher levels of PAP observed are therefore not surprising. Patients with COPD receiving LTOT had significantly higher levels of PAP than those of a control group when measured over 24 hours. These patients also had significantly higher PAP when the periods of sleep or exercise were excluded—that is, when performing normal daily activity breathing supplementary oxygen. We have not defined specific activities of daily living in this study so these data are not presented. When studied during sleep without oxygen, the COPD group had a further rise in PAP which was greater than that measured on exercise and which was abolished by breathing oxygen during sleep. Others have previously reported increased pulmonary vascular resistance during REM sleep and the beneficial effects of oxygen in patients with moderate pulmonary hypertension and severe COPD.10 However, as far as we are aware, the extent of these rises compared with those seen during other activity has not been studied.
The normal group did not show any change in PAP during sleep (which is not surprising); however, there was no significant rise in PAP during exercise which others have predicted.2 This is probably because the workload chosen for the exercise test (30 watts) was too low to put the pulmonary circulation of normal individuals sufficiently under stress. Furthermore, there was no variation in the PAP of this group during normal daily activity.
The number of patients with COPD in this study is small and therefore it is difficult to reach firm conclusions. However, for these individuals the rise in PAP seen during sleep may be an important contribution to the overall work facing the right heart and constitutes at least as great a haemodynamic burden as low level exercise.
In this study we have shown considerable variations in PAP during 24 hour ambulatory monitoring with normal daily activity, on exercise, and during sleep, and this may have implications for the way COPD is assessed. Measurement of PAP is difficult in ambulant patients because of the restrictions inherent in conventional cardiac catheterisation and may be unrepresentative because of the circumstances in which these are made—that is, at rest in the laboratory. Furthermore, non-invasive measurement with echocardiography in patients with COPD is often limited by the poor signal obtained. The technique of ambulatory PAP monitoring described in this paper allows the time course and extent of rises in PAP to be measured and correlated with symptoms in patients carrying out normal daily activities. Such knowledge of the pulmonary circulation under stress or during sleep in patients with COPD may be useful in assessing the contribution of pulmonary hypertension to overall morbidity and mortality. We have observed and quantified transient rises in PAP during sleep and exercise during ambulatory monitoring in the hospital environment in patients treated with LTOT. We speculate that similar increases in PAP may also be important in patients with milder COPD, which might have implications for future interventions.
Footnotes
-
Supported by a British Heart Foundation project grant.