Article Text

Abstract
Background: We have developed a method of high magnification bronchovideoscopy that enables improved observation of subepithelial vascular patterns of the bronchial mucosa. A study was undertaken to investigate the value of high magnification bronchovideoscopy in the detailed examination of dysplasia in the bronchial mucosa of patients with abnormal mucosal fluorescence.
Methods: Thirty one patients with sputum cytology specimens suspicious or positive for malignancy were entered into the study. Conventional white light examination was first performed under local anaesthesia and fluorescence bronchoscopy was also carried out using a light induced fluorescence endoscopy (LIFE) lung system. A high magnification bronchovideoscope (XBF 200HM2) was then used to examine the microvascular network in the bronchial mucosa at sites of normal and abnormal fluorescence and the images obtained were compared with pathological diagnoses from bronchial biopsy specimens. Vascular area ratios were calculated using image analysing apparatus.
Results: Vascular networks with regular patterns were observed at 20 of 22 abnormal fluorescence sites in biopsy specimens from patients with bronchitis. However, vascular networks with increased vessel growth and complex networks of tortuous vessels of various sizes were observed in 15 of 21 abnormal fluorescence sites in dysplasia specimens. There was a significant difference between bronchitis and dysplasia specimens (OR=25, 95% CI 5.5 to 113, p<0.0001). Mean vascular area ratios from 16 normal bronchial epithelium specimens with normal fluorescence, and 22 bronchitis and 21 dysplasia specimens with abnormal fluorescence were 0.054 (95% CI 0.039 to 0.07), 0.095 (95% CI 0.072 to 0.118), and 0.173 (95% CI 0.143 to 0.203), respectively. The results indicate a statistically significant increase in vascular area in the three groups (p<0.0001).
Conclusion: Areas of increased vessel growth and complex networks of tortuous vessels in the bronchial mucosa detected using a high magnification bronchovideoscope at sites of abnormal fluorescence may enable discrimination between bronchitis and dysplasia.
- high magnification bronchovideoscopy
- bronchial dysplasia
- neovascularisation
Statistics from Altmetric.com
The application of fluorescence bronchoscopy has made it possible to diagnose bronchial dysplasia locally, and some cases are thought to represent the precancerous lesions of squamous cell carcinoma.1–3 Centrally arising squamous cell carcinoma of the tracheobronchial tree, especially in heavy smokers, is thought to develop through multiple stages from squamous metaplasia to dysplasia, followed by carcinoma in situ, and finally to invasive cancer.4,5 A new strategy for the treatment of squamous cell carcinoma of the tracheobronchial tree might therefore involve the detection and eradication of preinvasive bronchial lesions defined as dysplasia and carcinoma in situ according to recent World Health Organization criteria,6 before progression to invasive cancer.7,8 Observations made by fluorescence bronchoscopy have revealed that preinvasive bronchial lesions have abnormal brown or reddish brown fluorescence which can distinguish precancerous tissues from normal bronchial tissue.9–11
As the lesions are very small, few studies have examined dysplasias in detail by conventional white light bronchoscopy,12,13 and the only descriptions are of swelling and redness at bronchial bifurcations. We recently examined dysplastic lesions in the bronchial mucosa by white light bronchoscopy using a bronchovideoscope together with fluorescence bronchoscopy using a light induced fluorescence endoscopy (LIFE) lung system.3 However, it remained impossible to obtain findings other than swelling and redness at bronchial bifurcations.
Increased thickening of the bronchial epithelium and increased vessel growth are thought to be related to the appearance of areas of abnormal fluorescence, suggesting roles for neovascularisation or increased mucosal microvascular growth in bronchial dysplasia. Recently, a new morphological entity—angiogenic squamous dysplasia—was identified in large airways by fluorescence bronchoscopy,14–16 characterised by collections of capillary blood vessels closely juxtaposed to and projecting into dysplastic bronchial epithelium.
We have developed a direct viewing high magnification bronchovideoscopy system which enables detailed observations of dysplasia in the bronchial mucosa to be made.17 The bronchovideoscope has an outer diameter of 6 mm and can easily be inserted into the tracheobronchial tree. To examine microvascular networks in the bronchial mucosa, observations were made using the high magnification bronchovideoscope primarily at sites of abnormal fluorescence previously established by fluorescence bronchoscopy. The observed microvessel vascular patterns were used to calculate vascular area ratios and the results obtained from bronchitis and dysplasia biopsy specimens were compared by objective evaluation using image analysing apparatus.
METHODS
High magnification bronchovideoscope
A high magnification bronchovideoscope (XBF 200HM2) developed in conjunction with the Olympus Optical Corporation, Tokyo, Japan was used in the study. This bronchovideoscope combines two systems—a video observation system for high magnification observation and a fibre observation system for orientation of the bronchoscope tip. For the video observation system an objective optical system, in fixed focus mode rather than zoom mode, was used to give an outer diameter of about 6 mm to allow for the bronchoscope and the observation depth of 1–3 mm. Magnification was about fourfold higher than that of the BF240 bronchovideoscope, and the bronchial mucosa could be observed minutely on a 14-inch TV monitor at a high magnification at the nearest point 110×.
The high magnification bronchovideoscope was inserted into the tracheobronchial tree while observing progress using the fibre observation system for orientation until it could be confirmed that the tip had reached the target area. The tip was then brought close to the bronchial mucosa and the mucosa observed at high magnification on a TV monitor (fig 1).

High magnification bronchovideoscope. The bronchovideoscope is a combination of two systems, a video observation system for high magnification observation and a fibre observation system for bronchoscope tip orientation.
Patients and procedure
Thirty one patients (29 men) of mean age 67 years (range 47–77) with sputum cytological specimens which were suspicious or positive for malignancy were entered into the study between January 1999 and May 2000. Their smoking history ranged from 28 to 153 pack years (mean 62). Twenty seven of the patients were current smokers and four were ex-smokers.
Conventional white light bronchoscopy (BF-240, Olympus Optical Corporation, Tokyo, Japan) was first performed under local anaesthesia with sedation by intravenous midazolam and oxygen inhalation. fluorescence broncoscopic examination was performed using the LIFE lung system (Xillix LIFE-Lung Fluorescence Endoscopy System; Xillix Technologies Corporation, Richmond, BC, Canada). Observations by high magnification bronchovideoscopy were made primarily at sites of normal and abnormal fluorescence established by fluorescence bronchoscopy to examine microvascular networks in the bronchial mucosa. Bronchial biopsy specimens for pathological examination were obtained from 16 normal and 43 abnormal areas of the bronchial mucosa. Images obtained by high magnification bronchovideoscopy were compared with the pathological diagnoses of the bronchial biopsy specimens.
All participants provided written informed consent before enrollment into the study. Ethical approval was granted by the Chiba University ethics committee.
High magnification bronchovideoscopy of the bronchial mucosa
High magnification bronchovideoscopy enabled the microvascular networks in the bronchial mucosa to be visualised. Typical bronchoscopic findings from sites of normal and abnormal fluorescence are shown in fig 2. While only a few subepithelial microvessels were observed at sites of normal fluorescence (fig 2A), microvessels of various sizes were observed at sites of abnormal fluorescence (fig 2B). Thus, using our system it was possible to discern the distribution of microvessels, ranging from a few subepithelial microvessels to complicated vascular networks.

High magnification bronchovideoscopy of bronchial mucosa. The high magnification bronchovideoscope enabled the microvascular networks in the bronchial mucosa to be seen. Typical comparative bronchoscopic findings between sites of (A) normal and (B) abnormal fluorescence are shown. (A) Site of normal fluorescence with few subepithelial microvessels. (B) Site of abnormal fluorescence showing microvessels of various grades. Using this method it is possible to discern different patterns of microvessel distribution such as low numbers of subepithelial microvessels and complex vascular networks.
Histopathology and immunohistochemistry
Biopsy specimens were fixed in 10% neutral formalin, embedded in paraffin, and stained with haematoxylin-eosin for histological examination. The specimens were first evaluated by a pathologist in our department and then all slides were reviewed by two expert pulmonary pathologists in our department (KH and HO) according to recent World Health Organization criteria.6 Angiogenic squamous dysplasia was characterised by microscopic projections into the bronchial lumen surface by squamous bronchial epithelium exhibiting variable degrees of squamous dysplasia.14,16
Endothelial cells were highlighted in tissue sections by immunohistochemical staining using the endothelial marker CD34. This marker was used to identify capillary cores in the angiogenic squamous dysplasia lesions. To demonstrate this antigen, paraffin sections were stained with mouse anti-CD34 antibody (Immunotech, Marseille, France) and labelled with streptavidin biotinylated antibody (Nichirei Corporation, Tokyo, Japan) for detection.
Calculation of vascular area ratios using image analysing apparatus
For examination of the vascular patterns obtained by high magnification bronchovideoscopy, vascular area ratios were calculated as follows using image analysing apparatus with special software developed by the Olympus Optical Corporation, Tokyo, Japan.
Areas of interest: areas of interest were selected from original images.
Green images: for the extraction treatment of vascular images, red (R), green (G) and blue (B) images were obtained by high magnification bronchovideoscopy and G images were used to give the highest contrast against vessels. Noise reduction was applied to suppress the electrical noise effect and de-gamma correction was performed to make the image data linear.
Filter treatments: in addition, filter treatments using a digital filter for G images were applied to extract the vascular images according to the diameters.
Threshold treatment: candidate vascular areas were separated from surrounding areas by threshold treatment of the data after filter treatment.
Eliminating small non-vascular areas: after eliminating small non-vascular areas, the remaining areas were used as vascular images.
Vascular area ratios: vascular area ratios were determined as the ratio of the number of picture elements in the vascular area after exclusion of areas of halation to the number of picture elements in the area of interest (fig 3).

Calculation of vascular area ratios using image analysing apparatus. (A) Areas of interest selected from original images. (B) For the extraction of vascular images green images obtained by high magnification bronchovideoscopy were used to give the greatest contrast with vessels. Noise reduction was applied to suppress the electrical noise effect and de-gamma correction was performed to make the image data linear. (C) Filter treatments using a digital filter for green images were applied to extract the vascular images according to the diameter. (D) Candidate vascular areas were separated from surrounding areas by threshold treatment of the data after filter treatment. (E) After eliminating small non-vascular areas, the remaining areas were used as vascular images. (F) Vascular area ratios were determined as the ratio of the number of picture elements in the vascular area after exclusion of areas of halation to the number of picture elements in the area of interest.
It takes 0.9 seconds to process the data to achieve a vascular area ratio with 140 × 190 pixels using Pentium II, 450 MHz.
Calculation of vessel diameter observed as scattered red dots using high magnification bronchovideoscopy
The observation depth with high magnification bronchovideoscopy (XBF 200HM2) is 1–3 mm. Using known charts, magnification on a 14-inch TV monitor was calculated at 110× to 55×. If L = actual size of the vessel targeted, K (conversion factor) = 9.1 × 102 μm/pixel (calculated from the number of pixels on the XY coordinates measured using actual measurement values (μm) on the TV monitor and Adobe Photoshop 6.0 (Adobe Systems Incorporated, CA, USA)), D (distance between two points on Adobe Photoshop 6.0) pixel = √[(X1 – X2)2 + (Y1 – Y2)2], and M = magnification, L is expressed as K × D/M.
Calculation of diameter of capillary blood vessels in angiogenic squamous dysplasia
Using an image cytometry (CAS 200) cell analysis system (Becton Dickenson, San Jose, CA, USA) micrometer program, we calculated the diameter of capillary blood vessels in angiogenic squamous dysplasia identified histologically on a biopsy slide stained with haematoxylin-eosin.
Statistical analysis
Fisher’s exact probability test and the ANOVA test were used to evaluate the significance of differences between results, with p values of <0.05 being considered statistically significant. Significances of individual differences were evaluated using the Bonferroni/Dunn test if ANOVA was significant. Odds ratios (OR) and mean values are presented with 95% confidence interval (CI). Calculations were performed using the statistical software package StatView 5.0 (SAS Inc, Cary, NC, USA).
RESULTS
Pathological diagnoses of biopsy specimens
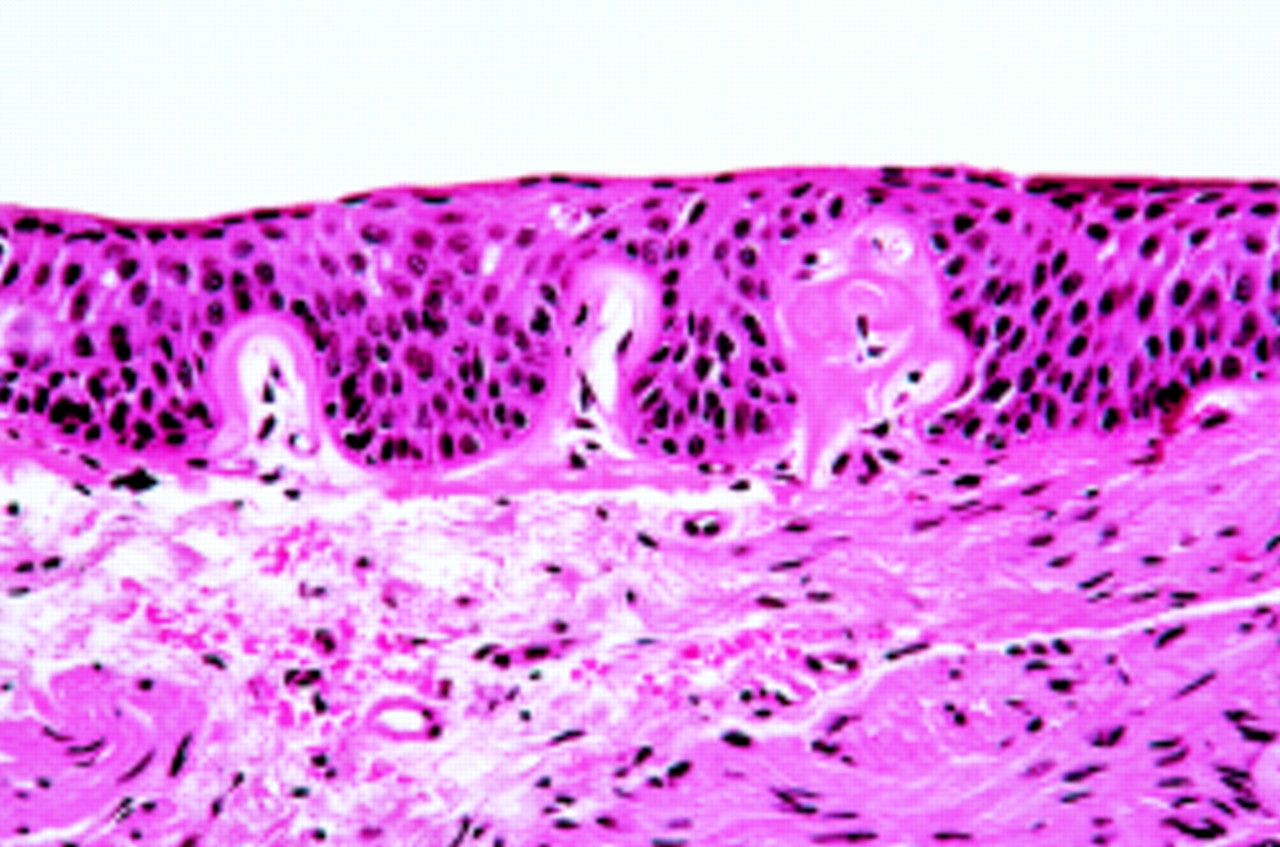
All the biopsy specimens from 16 normal fluorescence sites were found to consist of normal bronchial epithelium. Biopsy specimens from 43 abnormal fluorescence sites were diagnosed as 22 bronchitis and 21 dysplasia. Of the 21 bronchial dysplasia specimens, 17 lesions had morphological changes characteristic of angiogenic squamous dysplasia reported by Keith and coworkers.14 Collections of capillary sized blood vessels closely juxtaposed to and projecting into dysplastic bronchial epithelium were observed in the biopsy specimens (fig 4). Immunohistochemical stains for CD34 confirmed the presence of endothelial cells lining the capillaries in the core of the papillary projections and subepithelial lamina propria (fig 5). Micropapillary invasion of capillaries was not seen in the bronchitis biopsy specimens.

Photomicrograph of angiogenic squamous dysplasia showing collections of capillary sized blood vessels closely juxtaposed to, and projecting into, dysplastic bronchial epithelium.

Angiogenic squamous dysplasia lesion stained for endothelial cells with the endothelial marker CD34 antibody.
High magnification bronchovideoscopy of bronchial mucosa at sites of abnormal fluorescence
Figure 6A shows three different bronchoscopic views of the right basal bronchus under white light, fluorescence bronchoscopy, and high magnification bronchovideoscopy in a patient with sputum cytology suspicious of malignancy. Swelling at the bifurcation of rt B7 and B8,9,10 was present under white light examination, and an abnormal brown area was noted during the following fluorescence examination. Vascular networks with regular patterns were observed at sites of abnormal fluorescence by high magnification bronchovideoscopy and the pathological diagnosis of the biopsy specimen was bronchitis. Similar vascular networks with regular patterns were observed in 20 of 22 abnormal fluorescence sites with bronchitis.

Magnified view of the bronchial mucosa by high magnification bronchovideoscopy at sites of abnormal fluorescence established by fluorescence bronchoscopy. (A) In a patient with bronchitis a regular vascular network pattern is observed. (B) In a patient with dysplasia increased vessel growth and complex networks of tortuous vessels of various sizes are seen.
Figure 6B shows three different views of the left upper bronchus under white light, fluorescence bronchoscopy, and high magnification bronchovideoscopy in a patient with sputum cytology positive for malignancy. Redness and swelling at the bifurcation of lt B1+2a,b and B1+2c were seen under white light examination and an abnormal reddish brown area was identified by fluorescence bronchoscopy. Increased vessel growth and complex networks of tortuous vessels were observed at sites of abnormal fluorescence by high magnification bronchovideoscopy. The pathological diagnosis of the biopsy specimen was dysplasia. Similar vascular networks with increased vessel growth and complex networks of tortuous vessels of various sizes were observed in 15 of 21 abnormal fluorescence sites with dysplasia. There was a significant difference between bronchitis and dysplasia (OR=25, 95% CI 5.5 to 113; p<0.0001, Fisher’s exact probability test).
Calculation of vascular area ratios from vascular patterns using image analysing apparatus
Vascular area ratios were compared between sites of normal fluorescence from the 16 normal bronchial epithelium specimens and at sites of abnormal fluorescence in the 22 bronchitis and 21 dysplasia specimens (mean values of 0.054 (95% CI 0.039 to 0.07), 0.095 (95% CI 0.072 to 0.118), and 0.173 (95% CI 0.143 to 0.203), respectively). The results indicated a statistically significant increase in vascular area in the three groups (p<0.0001, Bonferroni/Dunn test; fig 7).

Vascular area ratios of normal bronchial epithelium, bronchitis, and dysplasia biopsy specimens.
Comparison of vessels in angiogenic squamous dysplasia
The size of vessels L1, L2, and L3 was calculated as 42.2–84.3 μm, 41.4–82.7 μm, and 50.3–100.6 μm, respectively, at an observation depth of 1–3 mm. The diameter of capillary blood vessels C1, C2, C3, and C4 in angiogenic squamous dysplasia was calculated by an image cytometry (CAS 200) cell analysis system as 49.9 μm, 47.6 μm, 34.4 μm, and 26.5 μm, respectively. Thus, the actual diameters seen in the histopathological samples roughly matched the vessel diameters seen by high magnification bronchovideoscopy, especially at an observation depth of 1 mm (fig 8).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison between vessels observed as scattered red dots using high magnification bronchovideoscopy and capillary sized blood vessels projecting into dysplastic epithelium microscopically (angiogenic squamous dysplasia).
Comparison of sensitivity and specificity of high magnification bronchovideoscopy for the detection of bronchial dysplasia
We examined the usefulness of high magnification bronchovideoscopy for the detection of bronchial dysplasia at sites of abnormal fluorescence established by fluorescence bronchoscopy. Specimens showing vascular networks with increased vessel growth and complex networks of tortuous vessels of various sizes by high magnification bronchovideoscopy were assumed to be positive for dysplasia, and specimens showing vascular networks with a regular pattern by high magnification bronchovideoscopy were assumed to be negative for dysplasia (may be bronchitis). The sensitivity and specificity of the magnified images were 71.4% (15/21) and 90.9% (20/22), respectively.
DISCUSSION
Progress in the field of fluorescence bronchoscopy has made it possible to locally diagnose bronchial dysplasia, thought sometimes to be the precancerous lesions of squamous cell carcinoma. We have recently reported the results of extensive studies of dysplasia in bronchial mucosa using white light bronchoscopy combined with fluorescence bronchoscopy.3 However, it proved impossible, even with a BF240 bronchovideoscope, to obtain findings other than swelling and redness in bronchial bifurcations, as previously reported.12,13 Because of the difficulty in diagnosing dysplasia by white light bronchoscopy, we attempted to obtain detailed white light observations of bronchial dysplasia using a direct viewing high magnification bronchovideoscope with the aim of developing a new method of bronchoscopic diagnosis.
In gastrointestinal endoscopy, high magnification endoscopy has been developed for observing and analysing epithelial microstructures. Moreover, there have been several recent reports on the usefulness of high magnification endoscopy in other clinical applications including pit pattern analysis of large bowel tumours18,19 and observation of normal mucosa and carcinoma in situ of the oesophagus.20,21 However, in the field of bronchoscopy the size of the outer diameter of the tube inserted into the bronchus has made it difficult to load a bronchoscope with a zooming mechanism such as the one used in high magnification gastrointestinal endoscopy. We have therefore developed a high magnification bronchovideoscope consisting of two systems—a video observation system for high magnification viewing and a fibre observation system for the orientation of the bronchoscope tip using a fixed focus eyepiece. The bronchial mucosa could then be observed at high magnifications up to 100–110×.
With the aim of elucidating the mucosal findings of bronchial dysplasia, high magnification observations were made primarily at sites of abnormal fluorescence established by fluorescence bronchoscopy. Examination of microvascular networks in the bronchial mucosa using our system proved to be simple and effective. At sites of normal fluorescence only a few subepithelial microvessels were observed, while at sites of abnormal fluorescence microvessels of various sizes were found. Our findings showed that many cases of dysplasia had vascular patterns of increased vessel growth and complex networks of tortuous vessels. To obtain an objective evaluation of our findings, vascular area ratios were calculated using an image analysing apparatus. The vessel networks in specimens of bronchial dysplasia had significantly increased vascular area ratios compared with those of bronchitis.
In addition to increased thickening of the bronchial epithelium, increases in blood content or vessel growth are thought to be involved in areas of abnormal fluorescence in precancerous and cancerous lesions. Abnormal fluorescence of dysplastic lesions, as observed by fluorescence bronchoscopy, has been associated with increased blood content due to increased mucosal microvascularity.14 The results of our study confirmed these findings; increased vessel growth and the presence of complex networks of tortuous vessels were associated with dysplasia in heavy smokers and suggested a strong correlation between these areas and sites of abnormal fluorescence. To our knowledge, this is the first report to show that neovascularisation of bronchial mucosa is associated with bronchial dysplasia by in vivo examination using high magnification bronchovideoscopy.
A comparison between vessels observed as scattered red dots using high magnification bronchovideoscopy and capillary sized blood vessels projecting into dysplastic epithelium microscopically revealed the sizes to be almost identical. We doubted that many of the vessels projected into the dysplastic epithelium, and considered that not only were many of the vessels detected by high magnification bronchovideoscopy vessels of various diameters in subepithelial lamina propria, but also that some of the vessels detected as scattered red dots were capillary sized blood vessels in angiogenic squamous dysplasia.
Fluorescence bronchoscopy appears to be significantly more sensitive at detecting preinvasive bronchial lesions than white light examination but has low specificity. In future, quantitative fluorescence imaging or combined fluorescence-reflectance imaging may also be helpful to improve specificity.22 In this study we have shown that, at sites of abnormal fluorescence established by fluorescence bronchoscopy, high magnification bronchovideoscopy detects bronchial dysplasia more accurately than fluorescence bronchoscopy alone.
Several studies have examined the role of neovascularisation in dysplasia of the bronchus or uterine cervix using pathological specimens.14,23–25 For bronchial dysplasia it was found that a pathological condition suggestive of neovascularisation was associated with the early stages of multistage carcinogenesis in squamous cell carcinoma.14 Our study population included heavy smokers in whom increased vessel growth or complex networks of tortuous vessels were frequently observed in areas of dysplasia. This suggests a role for neovascularisation in the maintenance and progression of dysplasia. In dysplasia of the uterine cervix, observation of vessels by colposcopy has also shown that neovascularisation contributes to the progression from dysplasia to carcinoma in situ and finally to invasive cancer.22 It is therefore interesting to speculate that neovascularisation may be required for the maintenance and progression of dysplasia.
In conclusion, the use of high magnification bronchovideoscopy revealed microvessels of various sizes at sites of abnormal fluorescence. Increased vessel growth and complex networks of tortuous vessels were observed in regions of bronchial dysplasia, and the vascular area ratios of these regions were significantly higher in dysplasia than in bronchitis. Thus, there was an association between neovascularisation and bronchial dysplasia. High magnification bronchovideoscopy may therefore enable the discrimination between bronchitis and dysplasia.
Acknowledgments
The authors thank Sakae Takehana, Takeshi Takigawa, Yuichi Morizane, and Kenji Yamazaki (Olympus Optical Corporation, Tokyo, Japan) for technical assistance.
REFERENCES
Footnotes
-
Supported in part by Grant-in-Aid for Scientific Research (C) 13671376 from Japan Society for the Promotion of Science.