Article Text

Abstract
Background: A study was undertaken to investigate the clinical practice, yield, and costs of preoperative staging in patients with suspected NSCLC and to obtain baseline data for prospective studies on the cost effectiveness of 18F-fluorodeoxyglucose positron emission tomography in the management of these patients.
Methods: A retrospective study of the medical records of all patients with suspected NSCLC was performed during a 2 year interval (1993–4) in an academic and a large community hospital.
Results: Three hundred and ninety five patients with suspected NSCLC were identified; 58 were deemed to be medically inoperable and 337 patients proceeded to the staging process. Staging required a mean (SD) of 5.1 (1.5) diagnostic tests per patient (excluding thoracotomy) carried out over a median period of 20 days (IQR 10–31). Many of the tests (including both invasive and non-invasive) were done because previous imaging tests had suggested metastases, and in most cases the results of initial tests proved to be false positives. After clinical staging, 168 patients were considered to be resectable (stage I/II) and 144 patients underwent surgery with curative intent. At surgery 33 patients (23% of those who underwent surgery) were found to have irresectable lesions and 19 (13%) had a benign lesion. Surgery was also considered to be futile in 22 patients (15%) who developed metastases or local recurrence within 12 months following radical surgery. Hospital admission was responsible for most of the costs.
Conclusion: In many patients staging involved considerable effort in terms of the number of diagnostic tests, the duration of the staging period and the cost, with limited success in preventing futile surgery. Failures relate to the quality of diagnostic preparation at every level of the TNM staging system.
- non-small cell lung cancer (NSCLC)
- cost effectiveness
- staging
- CT, computed tomography
- NSCLC, non-small cell lung carcinoma
- PET, positron emission tomography
- IQR, interquartile range
- FDG, 18F-fluorodeoxyglucose
Statistics from Altmetric.com
- CT, computed tomography
- NSCLC, non-small cell lung carcinoma
- PET, positron emission tomography
- IQR, interquartile range
- FDG, 18F-fluorodeoxyglucose
The selection of candidates for appropriate treatment, particularly for curative surgery, is the key issue in staging patients with NSCLC.1 A battery of diagnostic tests pertaining to each aspect of the TNM staging system is potentially available. On the other hand, there are societal concerns and economic restraints. The cost of staging lung cancer is increasing because of an increase in newly diagnosed cases of NSCLC. Not surprisingly, guidelines for staging have been developed which can be adapted to include new therapeutic and diagnostic developments.2–4 In the past decade new diagnostic methods such as magnetic resonance imaging (MRI) and positron emission tomography (PET) have emerged, claiming a role in the staging process.5 The initial step in assessment of such new technologies should be the evaluation of prevailing clinical practice and its residual inefficiency.6 Evaluation of the prevailing clinical practice based simply on the estimated use of guidelines is less desirable since adherence to such guidelines is unpredictable.7 Studying actual patient data may be more accurate than questionnaires8 or medical audits9; it also avoids the potential selection bias of socially desirable answers and accounts better for heterogeneity.
We have systematically investigated the manner, yield, and costs of NSCLC staging as carried out in two major Dutch hospitals. In addition, this study provided baseline data for prospective studies on the cost effectiveness of PET using 18F-fluorodeoxyglucose (FDG).10
METHODS
The medical records of all patients with diagnosed or suspected NSCLC referred by their family physicians to the pulmonologists at the academic hospital VU University Medical Center, Amsterdam (VUMC) and the community hospital Medical Centre Alkmaar (MCA) between January 1993 and January 1995 were reviewed. Patients were identified by crosslinking databases of the Dutch Cancer Registry, the Pathological Anatomical National Register (PALGA), local surgery records, and the minutes from regular multidisciplinary rounds. The following information was extracted: demographic data, pathological data, the number and type of diagnostic investigations (excluding laboratory and lung function tests), the duration of the diagnostic process until definitive clinical TNM staging, postoperative TNM classification, and follow up data. Imaging tests, punctures/biopsies (not requiring mediastinoscopy, thoracotomy, video assisted thoracoscopy, or rigid bronchoscopy) and flexible bronchoscopy were classified as non-invasive investigations. Surgical staging procedures (such as mediastinoscopy and video assisted thoracoscopy) and rigid bronchoscopy were classified as invasive investigations.
Surgery was considered futile in cases of benign lesions, T4 lesions, macroscopic mediastinal lymph node involvement, or pleural metastasis. In addition, patients in whom a pneumonectomy was necessary to perform a complete resection but whose poor lung function allowed for only a less extended resection (such as (bi-) lobectomy) were also considered to have undergone futile surgery. Finally, the diagnosis of distant metastases or local relapse during the 12 months after surgery with curative intent were also regarded as futile surgery.
Cost methodology
A cost analysis was performed to assess the costs of the staging procedures in both hospitals, including that of surgical resection and the resulting number of hospital admission days. Costs of any additional treatment were not included. The total cost of the diagnostic strategies was obtained by multiplying the number of procedures performed by their individual costs. Detailed price calculations were made in the two hospitals to estimate unit costs accurately. This included the costs of personnel, materials, equipment, and overheads.
Analysis of data
Statistical analyses were performed using the Student's t test, Fisher's exact test, and the Mann-Whitney U test.
RESULTS
Three hundred and ninety five patients with suspected NSCLC were identified; 58 were medically inoperable because of severe comorbidity, leaving 337 patients (220 and 117 from the community hospital and university hospital, respectively) for further analysis; 271 (80.5%) were men, and the mean age was 64 years (range 27–88). The age and sex distribution were comparable in the two institutions.
Staging procedures
Chest radiography and flexible bronchoscopy were performed in all patients. A CT scan of the chest was performed in 315 patients. In 17 patients metastatic disease was found prior to CT scanning. In one patient the chest lesion proved to be a metastasis of urothelial carcinoma and further diagnostic tests were directed in search of the primary tumour. Four patients refused a chest CT scan. Between the first visit and the final clinical stage classification patients underwent a mean (SD) of 5.1 (1.5) diagnostic tests, with the number in the academic hospital (5.5 (1.7)) being higher than in the general hospital (4.8 (1.5); p=0.001). However, there was no significant difference in the number of diagnostic tests between patients considered to be operable and those deemed to be inoperable (5.0 (1.6) and 5.1 (1.6), respectively).
Apart from chest (and upper abdomen) CT scans, investigations carried out to find distant metastases in decreasing order of frequency (table 1) were: ultrasound and abdominal CT scan (48%), bone scan (36%), and CT/MRI scan of the brain (16%). Further diagnostic tests were necessary to evaluate suspicious lesions in 116 of the 337 patients (34%) which resulted in an additional 112 imaging procedures and 71 biopsies (excluding invasive mediastinal procedures). Bone scintigraphy accounted for 49% of the additional imaging tests. In 46% of the 68 patients from whom biopsy specimens were taken, suspicious lesions proved to be benign and thus false positive. Bone scanning had the highest proportion of inconclusive results (36%) compared with CT scanning of the abdomen/brain (4%) and ultrasound (3%). Twenty two (49%) of the 45 patients with inconclusive bone scans underwent surgery with curative intent.
Staging procedures aiming at nodal or distant metastases
Invasive procedures aimed at nodal and primary tumour staging were performed in 39% of all patients. In 65% of these investigations no malignant tissue was sampled. Mediastinoscopy was performed more often in the community hospital (59/99 patients, 60%) than in the academic hospital (9/69, 13%). In the latter, mediastinoscopy was performed only in cases with enlarged (>1 cm) lymph nodes on chest CT scanning.
Overall, 50% (169/337) of the patients proved to be ineligible for surgery with curative intent as a result of clinical staging.
Duration of staging and costs
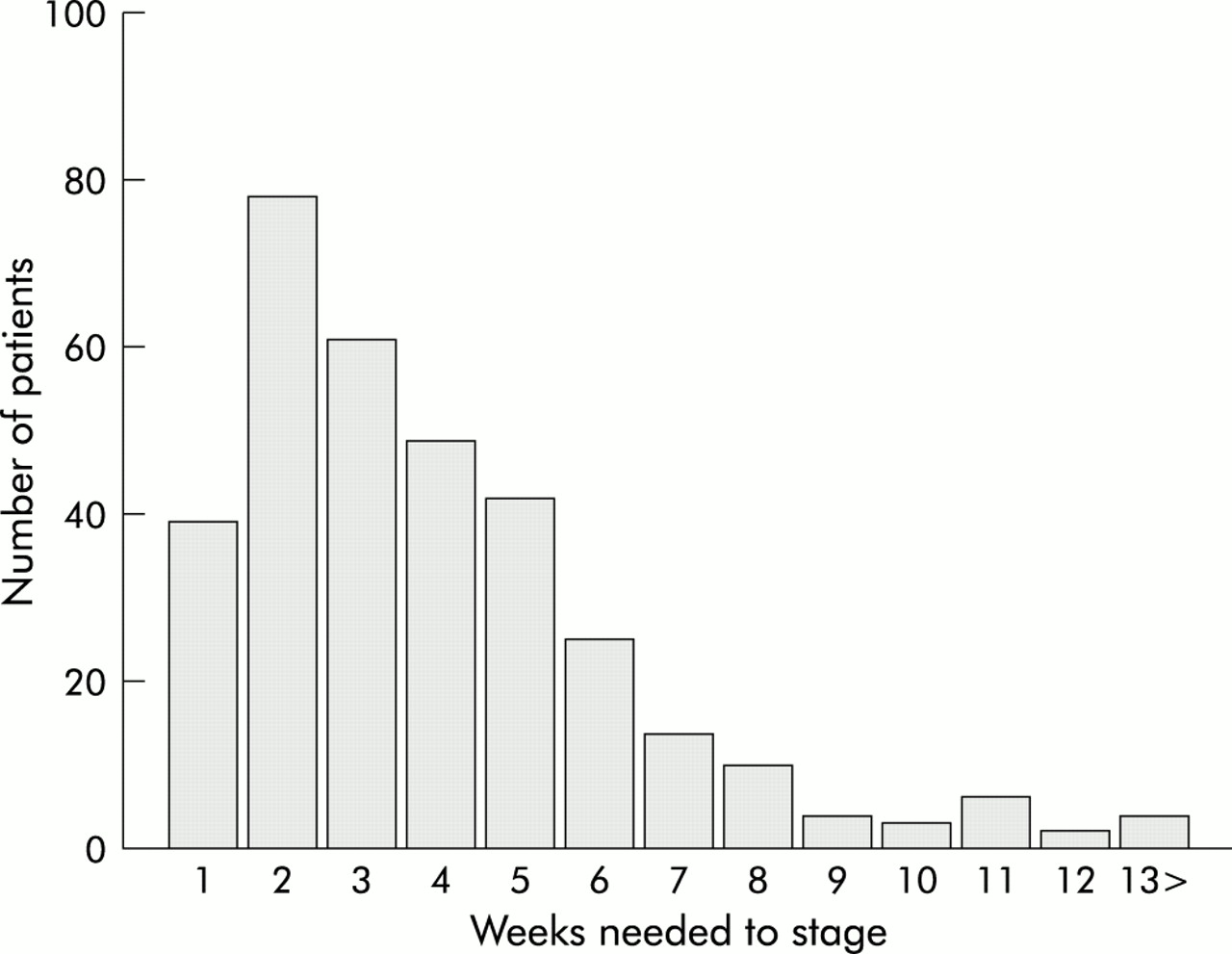
The frequency distribution of the duration required for clinical staging was positively skewed towards longer durations (fig 1). In 50% of the patients the diagnostic work up lasted more than 3 weeks (median 20 days (IQR 10–31)) where IQR = the numerical difference between the 25th and 75th centiles. This was especially true for patients who were eventually deemed to be operable (median 25 days (IQR 16–34) v 14 days (IQR 8–26) for clinically inoperable patients, p<0.001). The majority of patients were admitted to hospital for staging (academic hospital 61%, community hospital 95%). The mean hospital stay was approximately 1 week (median 9 days (IQR 2–15) for operable patients, 8 days (IQR 3–14) for inoperable patients).

{kind=link}
Time between first visit and finalising clinical staging.
Hospital stay for staging and for postoperative care accounted for most of the costs (table 2). The median postoperative hospital stay was 11 days in the academic hospital (IQR 9–16) compared with 15 days in the community hospital (IQR 12–17). Overall, the costs for staging were about one third that of the costs associated with thoracotomy. Higher costs were noted in the community hospital related to more hospital admissions for staging and the performance of more mediastinoscopies. Costs were similar in patients undergoing futile or non-futile surgery.
Mean costs (euro) per patient (1 euro = DFl 2.20)
Surgery and follow up
Planned thoracotomy was cancelled in 24/168 patients. In three the suspected lesion proved to be benign (sarcoidosis (n=2), pneumonia (n=1)), six refused thoracotomy, and the remainder were deemed to be medically unfit for surgery either because of comorbidity (CVA (n=3), cardiac events (n=6)) or deterioration of performance status (n=6). The exact time interval between finalising the clinical staging and the occurrence of the event precluding the planned thoracotomy could not be extracted from the medical records. Overall, in operated patients the median time interval between the finalisation of clinical staging and thoracotomy was 7 days (IQR 0–17). According to our criteria, surgery was futile in 74 of the remaining 144 patients (51%, 95% CI 43 to 60; table 3). Intraoperative staging consisted of lymph node sampling in the community hospital and mediastinal lymph node dissection in the academic hospital. Twenty patients underwent exploratory thoracotomy due to T4 lesions. Of these, two patients had brachial plexus involvement, seven had direct extension into the heart and/or main stem of the pulmonary artery, six had tumours invading mediastinal structures, and five patients could not tolerate the pneumonectomy which at surgery proved to be necessary to achieve a complete resection due to poor lung function. Eleven patients had gross mediastinal lymph node involvement which had not been detected during the preoperative work up. In two patients thoracotomy was also considered explorative due to pleural metastasis. There was no significant correlation between the time between clinical and intraoperative staging for patients in whom the tumour was irresectable (median 34 days, IQR 28–49) and those with resectable tumours (median 31 days, IQR 23–45). Nineteen patients proved to have benign lesions (nine hamartomas, seven reactive lesions, two fibrotic lesions, one cyst). Tumour histology other than NSCLC was found in seven patients (two metastases of other primary tumours, three carcinoid tumours, one SCLC, and one mesothelioma). Three patients had bronchoalveolar cell carcinoma.
Yield of clinical staging
Within 12 months after apparently curative surgery 22 patients were found to have recurrent disease: symptomatic distant metastases in 14, lymph node metastases in four, local recurrence in one, and “clinically evident” relapse (as reported by the general practitioner) in three patients (table 3). Preoperatively, 10 of the 14 patients with a distant relapse (71%) had undergone dissemination tests aimed at the affected organ. In the seven patients with tumour histology other than NSCLC, two with metastases of other primary tumours (colon, embryonic cell cancer) also proved to have metastases within 1 year of surgery. The other five patients remained disease-free during the follow up period and were not therefore considered to have undergone futile surgery. Five of the 144 patients who underwent curative surgery died within 3 months, one patient died after 3–12 months without evidence of disease, and six patients were lost to follow up.
Of all the patients with NSCLC, 21% (95% CI 16 to 25) were alive and clinically disease free at 12 months follow up. This was not significantly different for the two hospitals (VUMC 18% (95% CI 11 to 25), MCA 23% (95% CI 17 to 28)).
DISCUSSION
In this systematic retrospective study staging of patients with NSCLC proved to be an intensive and often protracted effort with a disappointingly high proportion of futile thoracotomies. However, this failure rate is comparable to that reported by others.11 VUMC is a tertiary referral centre for thoracic oncology so more patients with advanced tumours were considered for resection at this hospital. Unlike MCA (a community hospital), VUMC has a policy of staging central T3 and T4 lesions intraoperatively.
Even though attempts by the clinicians to minimise the delay due to staging were successful in many patients, a considerable subset went through a more protracted process. Tumour negative test results were abundant, which is obviously useful if they alter the pretest perception of curability. Unfortunately, most procedures were simply the sequel of earlier imaging tests suggesting metastases. This reflects specificity problems of these techniques and, in the case of mediastinoscopy, also the limited sensitivity of chest CT scans. It is possible that clinicians may have ordered dissemination tests at the same time as the initial work up tests in an effort to maintain momentum in the diagnostic process. For example, it is unclear what the impact of a chest CT scan might have been in patients already diagnosed with brain metastases on MRI. However, in 77% of cases dissemination tests were performed in compliance with the 1994 guidelines of Goldstraw et al3 (69% VUMC, 81% MCA). More imaging tests than are indicated by this guideline were performed in 15% of patients (26% VUMC, 9% MCA) and fewer than recommended were performed in 8% (4% VUMC, 10% MCA). With respect to mediastinal staging procedures, practices at both hospitals were compatible with prevailing guidelines.3,4 Even though differences in peroperative and postoperative failure patterns between hospitals appeared to reflect the differences in staging practice, the final result of diagnosis and treatment in terms of disease free 1 year survival between the two hospitals was identical.
From an economic perspective, the cost of the diagnostic tests themselves was only part of the problem. In the Netherlands costs mainly result from hospital admission for the staging procedures rather than from the tests themselves. This practice of hospitalisation is mainly intended to keep the staging process within acceptable time limits for patients. However, surveys carried out before this study (unpublished data) have shown that clinicians were under the impression that staging lasted a maximum of 2 weeks. The measurement of the actual time frame in this study confirms that questionnaires would probably have provided incorrect data in this respect.
Whole body PET allows for staging of the entire patient with a single scan, with the exception of assessment of local tumour infiltration and brain metastases. Whether its application in daily clinical practice will simplify the staging process and improve the final selection of patients for appropriate treatment is currently under study in clinical trials. There is evidence to suggest that mediastinoscopy can be omitted in cases with a negative PET scan of the mediastinum (with the exception of central tumours).12,13
In summary, many patients with suspected NSCLC undergo extensive investigations for clinical staging with ultimately disappointing results which apply to every level of the TNM system. Whether the current multistep process can be improved in terms of cost effectiveness by comprehensive techniques such as PET scanning remains to be shown in clinical trials. This study provides important baseline data for such trials.
Acknowledgments
The authors are grateful to Urvi Joshi MD, Department of Nuclear Medicine, VU University Medical Center, Amsterdam, the Netherlands for critical review of the manuscript.