Article Text

Abstract
BACKGROUND Talc and tetracyclines induce pleurodesis by directly injuring the pleura. The injury results in intense inflammation which subsequently leads to fibrosis. Corticosteroids can inhibit talc pleurodesis by reducing the inflammatory process. We hypothesised that transforming growth factor β2 (TGFβ2), a fibrogenic cytokine with immunomodulatory functions, could induce effective pleurodesis without generating significant pleural inflammation and therefore remain effective despite co-administration of corticosteroids.
METHODS Thirty rabbits were divided into two groups. Rabbits in the steroid group received weekly intramuscular injections of triamcinolone diacetate (0.8 mg/kg). Ten rabbits in each group were given 5.0 μg TGFβ2 intrapleurally via a chest tube while the remaining five received 1.7 μg TGFβ2. Pleurodesis was graded macroscopically after 14 days from 1 (none) to 8 (>50% symphysis).
RESULTS TGFβ2produced excellent pleurodesis at both 5.0 μg and 1.7 μg doses. The pleural effusions produced after the injection were low in all inflammatory markers. No significant differences were seen between the steroid group and controls in macroscopic pleurodesis scores (7.2 (1.3)v 7.1 (1.2)), levels of inflammatory markers in the pleural fluids (leucocyte 1107 (387)/mm3 v 1376 (581)/mm3; protein 3.1 (0.3) mg/dl v 2.9 (0.3) mg/dl, and LDH 478 (232) IU/l v 502 (123) IU/l), and the degree of microscopic pleural fibrosis and pleural inflammation.
CONCLUSIONS TGFβ2can induce effective pleurodesis and remains effective in the presence of high dose parenteral corticosteroids.
- transforming growth factor β
- pleurodesis
- corticosteroids
- pleural effusion
Statistics from Altmetric.com
Pleurodesis remains an important treatment option in the management of malignant pleural effusions and recurrent pneumothorax. Commonly used pleurodesing agents such as talc and tetracycline derivatives produce pleurodesis by inducing acute pleural injury and hence inflammation and fibrosis.1 This intense inflammatory process is essential to pleurodesis as we recently showed that co-administration of high dose parenteral corticosteroids reduced the inflammation and inhibited talc pleurodesis.2 It is also likely that chest pain and fever, common side effects after chemical pleurodesis, are the results of intense pleural inflammation.
The ideal pleurodesing agent would be one that can produce fibrosis without inducing pleural inflammation. Transforming growth factor beta (TGFβ), with its unique capabilities of being a strong fibrogenic activator as well as a potent anti-inflammatory cytokine, provides an attractive option as a novel treatment for producing pleurodesis.
TGFβ regulates fibrosis by increasing extracellular matrix formation and plays a vital role in fibrotic processes, including pulmonary fibrosis and wound healing.3 It is also a potent anti-inflammatory cytokine and can downregulate tumour necrosis factor α (TNFα) and inhibit lymphocyte function.4 We have recently reported that a single intrapleural injection of TGFβ2 produces excellent pleurodesis in rabbits5 ,6 and in sheep.7 The effusion produced was significantly less inflammatory than those resulting from talc or doxycycline.
In the present study we have investigated the effect of high dose systemic corticosteroids on TGFβ2 induced pleurodesis. We hypothesised that TGFβ2 produces pleurodesis without inducing significant pleural inflammation and hence systemic corticosteroids would have little or no inhibitory effect on TGFβ2 induced pleurodesis.
Methods
TRANSFORMING GROWTH FACTOR β2
A recombinant human TGFβ2 (Genzyme Corporation, Framingham, MA, USA) produced in Chinese hamster ovary cells was used. TGFβ2 was formulated in a vehicle consisting of 20 mM sodium phosphate, 130 mM sodium chloride, 15% (w/w) propylene glycol, and 20% (w/w) polyethylene glycol 400. The pH of the solution was 7.2. The vehicle was prepared using USP/NF grade reagents in water for injection and sterile filtered through a 0.2 μm filter. The TGFβ2 concentration was determined by the manufacturer with a sandwich enzyme linked immunosorbent assay using two monoclonal antibodies that cross react with both TGFβ2 and TGFβ3, and the activity of TGFβ2 was determined using a mink lung cell (Mv1Lu) antiproliferation assay modified from the method described by Ogawa.8
ANIMAL EXPERIMENT
The method used was similar to that described in our previous studies.5 ,6 ,9 The study protocol was approved by the Vanderbilt University Institutional Animal Care and Use Committee. New Zealand white rabbits weighing 1.5–2.0 kg were anaesthetised with an intramuscular injection of 35 mg/kg ketamine hydrochloride (Fort Dodge Animal Health, Iowa, USA) and 5 mg/kg xylazine hydrochloride (Fermenta, Kansas City, MO, USA). The chest was shaven and the skin sterilised with 10% povidone iodine (Baxter, Deerfield, IL, USA). The rabbit was placed in the lateral decubitus position and a small (<3 cm) skin incision was made midway between the tip of the scapula and the sternum approximately 2 cm above the costal margin. Chest tubes were made from intravenous solution set tubes (Baxter, Deerfield, IL, USA) with three extra openings near the distal end of the tube to enhance drainage. The chest tube was inserted by blunt dissection into the right pleural cavity while the left was used for control. The chest tube was secured at the muscle layers with purse string sutures. The proximal end of the chest tube was then tunnelled underneath the skin and drawn out through the skin posteriorly and superiorly between the two scapulae. The exterior end of the chest tube was sealed with a one way valve with cap (Medexinc, Hilliard, OH, USA) via an adapter and sutured to the skin. A three way stopcock was attached to the end of the chest tube through which any aspirated air was evacuated from the pleural space.
Thirty rabbits were divided into two groups of 15. Rabbits in the steroid group received an intramuscular injection of triamcinolone diacetate (Fujisawa Inc, Deerfield, IL, USA) 0.8 mg/kg at the time of chest tube insertion and then weekly afterwards. Rabbits in the control group received no steroid injections. All rabbits received an intrapleural injection of TGFβ2 (Genzyme Corporation, Framingham, MA, USA) on the day following the chest tube insertion. Ten rabbits in each group received a TGFβ2 dose of 5.0 μg in 2.5 ml while the remaining five in each group received a lower dose of 1.7 μg in 2.5 ml via the chest tube. This was followed by the injection of 1.0 ml of 0.9% sodium chloride (Baxter, Deerfield, IL, USA) to clear the dead space of the chest tube. The results of the five rabbits that received 1.7 μg TGFβ2 without steroid have previously been included in another study.10 These doses of TGFβ2 were chosen as they were shown to be the lowest effective doses in our previous studies.5 ,6
After the intrapleural injection the chest tube was aspirated at 24 hour intervals for any pleural fluid. The chest tube was withdrawn under light sedation if the pleural fluid drainage was <5 ml over the preceding 24 hours. Rabbits that developed signs of inflammation or infection at the skin wound were given daily intramuscular injections of 12.5 mg gentamicin (Fermenta, Kansas City, MO, USA) for two consecutive days. Rabbits that showed evidence of reduced oral intake or dehydration after the anaesthesia were given subcutaneous injections of 50 ml 5% dextrose and 50 ml 0.9% sodium chloride (Baxter, Deerfield, IL, USA) every 24 hours.
The volume of the pleural fluid collected was recorded. The total leucocyte count was measured using an automated counter (Coulter Electronics, Luton, UK) which was calibrated daily. The first reading was ignored and the mean of the next three readings was recorded. The protein, glucose, and lactate dehydrogenase (LDH) levels were determined with an automated analyser (Johnson & Johnson, Rochester, NY, USA). The upper limit of normal serum LDH concentrations in our laboratory is 618 IU/l.
At day 14 the rabbits were sedated and euthanised with carbon dioxide. The thorax was removed en bloc. The lungs were expanded by the injection of 50 ml 10% neutral buffered formalin into the exposed trachea via a plastic catheter. The trachea was then ligated with a silk suture and the entire thorax submerged into 10% neutral buffered formalin solution for at least 48 hours.
Grading of pleurodesis score
The degree of pleurodesis was graded on a scale of 1 to 8. Adhesions were defined as fibrous connections between the visceral and parietal pleurae. Symphysis was present if the visceral and parietal pleurae were difficult to separate as a result of adhesions.
1 = no adhesions between the visceral and parietal pleurae
2 = rare adhesions between the visceral and parietal pleurae with no symphysis
3 = scattered adhesions between the visceral and parietal pleurae with no symphysis
4 = many adhesions between the visceral and parietal pleurae with no symphysis
5 = many adhesions between the visceral and parietal pleurae with symphysis
involving <5% of the hemithorax
6 = many adhesions between the visceral and parietal pleurae with symphysis
involving 5–25% of the hemithorax
7= many adhesions between the visceral and parietal pleurae with symphysis
involving 25–50% of the hemithorax
8 = many adhesions between the visceral and parietal pleurae with symphysis
involving >50% of the hemithorax
Grading of haemothorax
0 = no evidence of haemothorax
1 = haemothorax involving <15% of the hemithorax
2 = haemothorax involving 15–33% of the hemithorax
3 = haemothorax involving 33–75% of the hemithorax
4 = haemothorax involving >75% of the hemithorax
Box 1 Grading of pleurodesis scores and haemothorax.
PLEURODESIS SCORING SCHEME
Necropsy was performed by two blinded investigators (KBL and RWL). A consensus grading was reached by the investigators on the degree of pleurodesis and on the extent of any haemothorax using the semi-quantitative scheme shown in box 1. Any evidence of infection or empyema was also assessed and recorded if present.
MICROSCOPIC EXAMINATION OF THE PLEURA
At the time of necropsy, samples of the visceral pleura and lung from each hemithorax were obtained and placed in 10% neutral buffered formalin. The tissue samples were stained with haematoxylin-eosin (H&E) and picrosirius stains. The degree of microscopic inflammation and fibrosis was graded from the H&E slide by an experienced examiner (LRT) blinded to the treatment agent. The pleural inflammation and fibrosis were graded as none (0), equivocal (1), mild (2), moderate (3), or severe (4), as in our previous studies.2 ,11 The thickness of the pleura was measured using the Leica Q500IW Imaging Workstation, Image Processing and Analysis System (Leica Ltd, Cambridge, UK). With this system, the image obtained was transformed from pixels to μm. Measurements were obtained at 10 different points on three different high power fields on each sample and the mean result was reported.
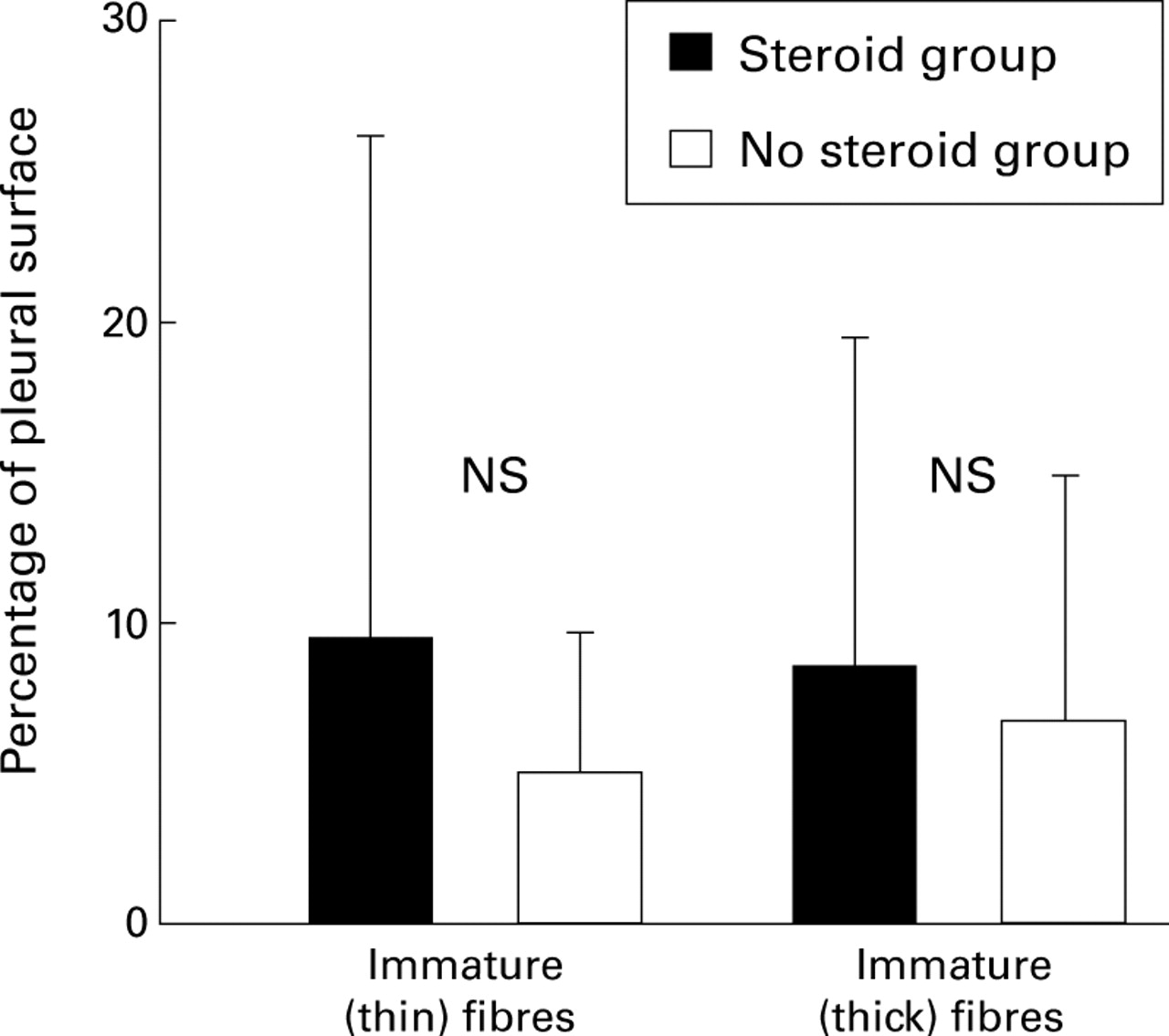
Collagen fibres were subdivided into immature (thin) and mature (thick) fibres using picrosirius staining as reported by Andradeet al.12 With this method the tissue blocks were sectioned at 5 μm and stained for 1 hour in a 0.2% solution of Sirius Red, Direct Red 80 (Aldrich, Milwaukee, WI, USA) dissolved in aqueous saturated picric acid. The enhancement of collagen birefringence elicited by picrosirius staining is specific for collagen and discloses its distinct patterns of physical aggregation. Immature (thin) fibres, as those present in early granulation tissue, are shown as weakly birefringent green structures while mature (thick) fibres, characteristic of mature fibrotic lesions, are identified by their strong birefringence and their yellow or red colour. The areas covered by mature and immature collagen fibres were also measured by the Leica Q500IW Imaging System (Leica Ltd, Cambridge, UK). All pixels in the image that are equivalent to, or nearly equivalent to, the colour levels of the select area were detected. The percentages of the total area of pleura covered by mature and immature fibres in the same field were measured. For each sample, readings were taken from six representative fields and the mean result used for analysis.
STATISTICAL ANALYSIS
Normality of the data was determined using the Kolmogorov-Smirnov test. The Student's t test (for parametric data) and Mann-Whitney rank sum test (for non-parametric data) were used to compare the values between subgroups. The pleural fluid parameters were normally distributed, while the data on pleural fibrosis and inflammation, alveolar fibrosis and inflammation, pleural thickness, and collagen fibre deposition were not normally distributed. For the pleurodesis scores, those of the 5.0 μg TGFβ2groups (both steroid and control groups) were normally distributed, but those of the 1.7 μg groups were not normally distributed. A p value of <0.05 was considered significant. Data were presented as mean (SD) unless otherwise stated. All data were analysed with a Sigma Stat V2.03 statistic software program (Jandel Scientific; San Rafael, CA, USA).
Results
Intrapleural injection of TGFβ2 in doses of both 5.0 μg and 1.7 μg produced effective pleurodesis in rabbits with mean pleurodesis scores of 7.3 (1.3) and 6.9 (1.2), respectively. There was no difference in the pleurodesis scores between rabbits that received TGFβ2 and systemic corticosteroids and rabbits that received TGFβ2 alone (7.2 (1.3) and 7.1 (1.2), respectively, p=NS, Mann-Whitney rank sum test). The results of the rabbits in each subgroup are presented in table 1.
Macroscopic pleurodesis scores in different subgroups
The injection of TGFβ2 stimulated the production of a large quantity of pleural fluid in all rabbits. The effusion produced was relatively non-inflammatory as evidenced by the low protein and LDH levels and total leucocyte count (table 2). The production of the fluid was transient and did not hinder the development of effective pleurodesis.
Pleural fluid characteristics
Rabbits that received TGFβ2 and corticosteroids showed no significant difference from those given only TGFβ2 in the amount of effusion produced and the biochemical analysis of the pleural fluid by the Student's t test (table 2). The only exception was the effusion protein level which was higher in the steroid group (mean 3.1 mg/dl v2.9 mg/dl, p=0.02), although the difference is unlikely to be of clinical significance. There was no difference in the other markers of inflammation (LDH level and total leucocyte count) between the two groups. The inflammatory indices of the pleural fluid from both groups of rabbits were significantly lower than previously published results of pleural fluids induced by intrapleural injections of talc, doxycycline, and mitoxantrone (table 3).
Pleural fluid characteristics in the present study compared with published data of pleural fluids induced by other pleurodesing agents
There was no difference in the effusion protein, LDH, and total leucocyte counts between rabbits given 5.0 μg TGFβ2and those given 1.7 μg. Interestingly, although the mean volumes of effusion at 24 hours were not different (26.6 ml in the 5.0 μg group and 28.9 ml in the 1.7 μg group), rabbits that received the higher dose of TGFβ2 had a significantly lower amount of total effusion drained (44.0 ml v 65.6 ml; p=0.02, Student's t test).
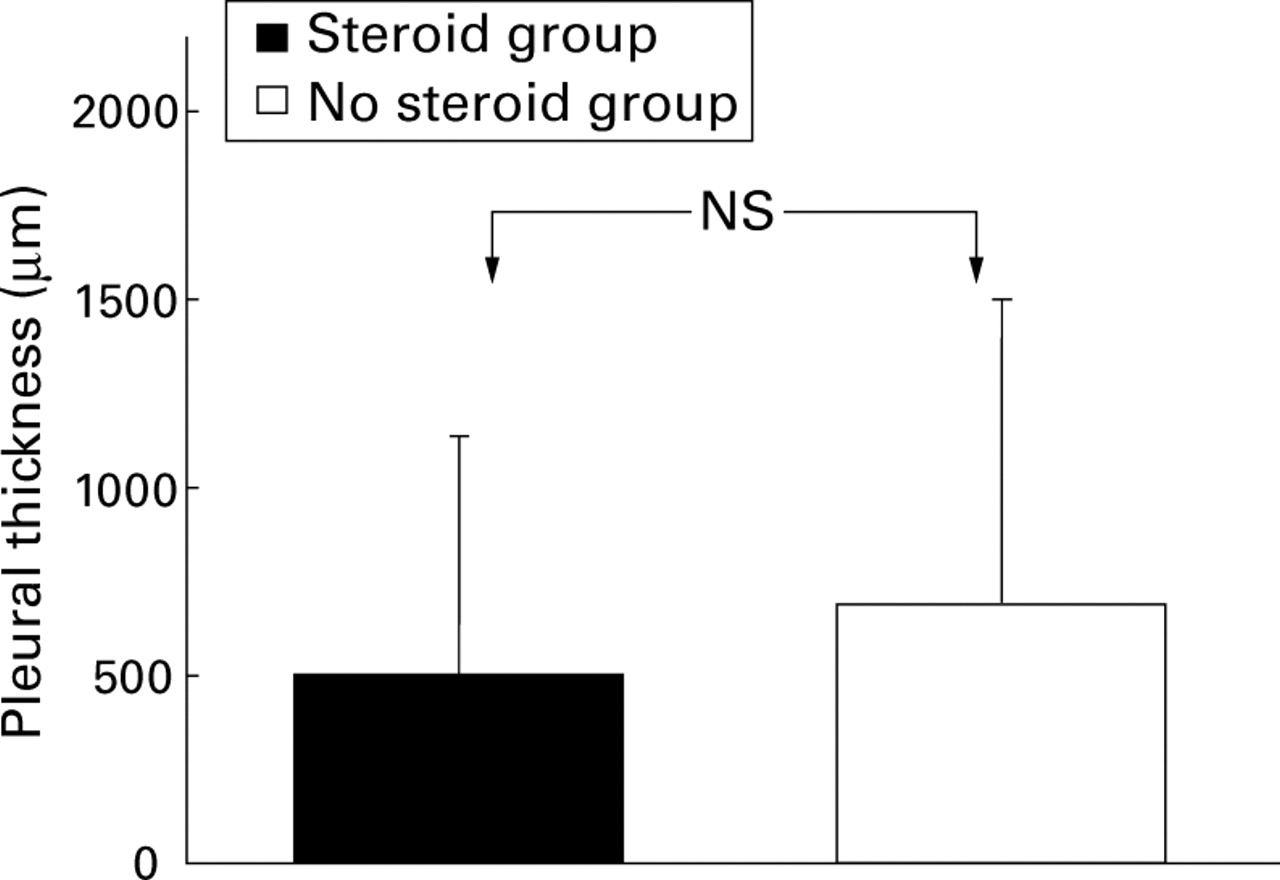
There were no significant differences in the microscopic grading scores for pleural fibrosis, pleural inflammation (fig 1), or in pleural thickness (fig 2) and collagen deposition (fig 3) between pleural tissues of the rabbits that received TGFβ2 and steroid and the tissues of rabbits given only TGFβ2 (Mann-Whitney rank sum test). The degree of alveolar inflammation and alveolar fibrosis was minimal in both groups (fig 1).

Comparison of histological changes in rabbits given TGFβ2 + corticosteroids v rabbits given TGFβ2 only.

Pleural thickness of rabbits given TGFβ2+ corticosteroids v rabbits given TGFβ2 only.

{kind=link}
{kind=link}
{kind=link}
Collagen deposition in rabbits given TGFβ2 + corticosteroids v rabbits given TGFβ2 only.
Four rabbits died and were replaced. Three of them died from causes related to surgery such as pneumothorax or pulmonary contusion during or within 48 hours of chest tube insertion. The fourth rabbit had a blocked chest tube and died from a tension hydrothorax 3 days after the injection of TGFβ2 (5.0 μg). Six rabbits in both groups had evidence of a haemothorax at the time of necropsy, although most of them were mild. The median (25–75% range) score of haemothorax was 0 (0.0–2.7) in rabbits given TGFβ2 + corticosteroids and 0 (0.0–2.0) in rabbits given TGFβ2only. None of the rabbits had evidence of empyema at necroscopic examination. The weight gain was comparable in rabbits that received corticosteroids and those that did not (0.18 (0.16) kgv 0.22 (0.19) kg; p=NS, Student'st test). Rabbits that received the lower dose gained more weight than rabbits that received the higher dose of TGFβ2 (0.14 (0.16) kg v 0.34 (0.12) kg; p=0.001, Student's t test). Three rabbits (all in 5.0 μg group; two had corticosteroids) required gentamicin for skin wound infections. One rabbit (in the no steroid group) required treatment with supplementary subcutaneous fluid.
Discussion
This study shows that TGFβ2 is effective in producing pleurodesis in a validated rabbit model. Systemic corticosteroids, at a dose that inhibits talc pleurodesis, did not affect the efficacy of TGFβ2 induced pleurodesis nor the inflammatory indices in the effusion fluid. The study provides further evidence that TGFβ2 induces pleurodesis via a pathway that involves minimal inflammation of the pleura and thus remains effective in the presence of high dose parenteral corticosteroids.
Conventional pleurodesing agents such as talc and tetracycline derivatives generate pleurodesis by creating acute pleural injury with subsequent inflammation and fibrosis.1 The intense inflammation is likely to be the cause of pain and fever which commonly complicate pleurodesis. The inflammatory process is, however, essential to the pleurodesis they produce. We have previously shown that the concurrent use of corticosteroids markedly decreases the inflammatory reaction and inhibits the development of pleurodesis after the intrapleural injection of talc.2
TGFβ is a ubiquitous cytokine notable for its potent profibrotic and anti-inflammatory properties, both of which make TGFβ an attractive option as a novel class of pleurodesing agent. Of the known growth factors, TGFβ is the most potent in stimulating extracellular matrix production and also readily inhibits its degradation.4Increased production and accumulation of TGFβ is an important feature in fibrotic diseases including pulmonary fibrosis and glomerulosclerosis.3 At the same time, TGFβ is a potent immunomodulatory cytokine. It can inhibit the production of TNFα, interleukin(IL)-1,3 and IL-813 and is more potent than cyclosporin as an inhibitor of lymphocyte functions.4
In the present study we have confirmed that direct administration of TGFβ2 to the pleura creates excellent pleurodesis. The doses of TGFβ2 we used were the lowest effective doses that stimulated pleurodesis in our previous studies.5 ,6We found that the pleurodesis induced by 5.0 μg TGFβ2was not inhibited by systemic corticosteroids at a dose that blocks talc pleurodesis. We also showed that corticosteroids did not inhibit the TGFβ2 induced pleurodesis even when we applied a lower dose of TGFβ2 (1.7 μg) which produced lower pleurodesis scores. The results of this study provide further evidence that TGFβ2 induces pleurodesis without necessitating pleural injury and inflammation. This is also confirmed by the low inflammatory indices (protein, LDH, and leucocyte counts) in the pleural fluids induced after TGFβ2 injection compared with pleural fluids induced after the intrapleural administration of conventional pleurodesing agents such as talc, doxycycline, or mitoxantrone (table 3).
Interestingly, the intrapleural injection of TGFβ2induced the production of large volumes of effusion. TGFβ can alter the morphology of mesothelial cells in vitro and increase the permeability of the mesothelial cell monolayer.14 It is also a potent stimulator for the release of vascular endothelial growth factor (VEGF) which, in turn, increases vascular permeability.15 We found that concurrent administration of corticosteroids made no difference to the amount of fluid produced, indicating that the production of fluid after TGFβ injection is unlikely to be due to inflammation. The total amount of effusion drained was significantly higher in rabbits receiving lower dose of TGFβ2 than in those receiving the higher dose, although there was no difference in the amount drained at 24 hours. We speculate that higher doses of TGFβ2 may induce more fibrosis and loculations in the first few days which impair pleural fluid drainage.
In our study rabbits that received 5 μg TGFβ2 gained less weight than those given 1.7 μg. Terrell et al 16 observed that rabbits treated with a single intravenous bolus of mid or high dose human recombinant TGFβ1 had a transient reduction in food consumption and weight. There was an associated slight decrease in albumin and total protein on day 3 which was reversed by 2 weeks. Similar findings were observed in rats given repeated injections of high doses of intravenous TGFβ1 16 or intraperitoneal TGFβ2.17 Increased serum levels of TGFβ and reduced levels of insulin-like growth factor 1 have recently been shown in mice with poor food intake and weight loss.18 The relationship between high doses of TGFβ and weight loss requires further investigation.
TGFβ is multifunctional and its actions on target cells are critically dependent on the cell type, its state of differentiation, and the particular set of growth factors and hormones acting on the cell.19 Its interactions with corticosteroids are complex. While TGFβ can reduce cortisol20 and mineralocorticoid21 synthesis, glucocorticoids in turn are potent regulators of the expression of TGFβ isoforms.22These regulations are again cell and stimulus specific.22 ,23 For example, glucocorticoids enhance accumulation of TGFβ mRNA in some cell lines including fibroblasts,24 osteoblasts,25 and T lymphocytes26 ,27 but inhibit the production of TGFβ in others.28 ,29
Our study is the first to examine the effects of corticosteroids on the action of TGFβ in pleural tissues. Previous studies of the in vivo effects of corticosteroids and TGFβ are limited and yielded conflicting results. In one study dexamethasone blocked the profibrotic effect of TGFβ in the abdominal wounds of rats.30 In another study, using a rat model of bleomycin induced pulmonary fibrosis, corticosteroids reduced the influx of inflammatory cells but the alveolar macrophage production of TGFβ was not inhibited by the corticosteroids.31 Conversely, other authors have also demonstrated that both local32 ,33 and systemic34 administrations of TGFβ could reverse the steroid induced impairment in wound healing. Little, however, is known of the in vivo interactions between corticosteroids and TGFβ in other organ systems.
In summary, TGFβ2 induces pleurodesis through a novel pathway whereby it induces pleural fibrosis without provoking excessive inflammation. We confirmed this by demonstrating that corticosteroids, at the same dose which blocks talc pleurodesis, did not impair the effectiveness of TGFβ2 in inducing pleurodesis. If these data can be extrapolated to humans, then TGFβ2 (as a non-inflammatory pleurodesing agent) may be less likely to induce pain and fever than talc and will remain effective in patients receiving corticosteroids.
Acknowledgments
This study was supported by the Saint Thomas Foundation, Nashville, TN, USA. We thank the Genzyme Corporation (Framingham, MA, USA) for providing the TGFβ2 used in the experiments. Dr Lee is a recipient of a United States-New Zealand Fulbright Graduate Award.