Article Text

Abstract
BACKGROUND Increased ambient levels of particulate matter <10 μm (PM10) from fossil fuel combustion are associated with an increased prevalence of respiratory symptoms in children. However, it is unknown whether, and to what extent, pollutant particles penetrate the paediatric lower airway. The capacity of alveolar macrophages (AM) to phagocytose inhaled material was used to directly assess exposure of normal children to particles.
METHODS AM from 22 children aged 3 months to 16 years with no respiratory symptoms were obtained by non-bronchoscopic bronchoalveolar lavage prior to elective surgery. In each child the size and composition of environmental particles within single sections from 100 separate AM was determined by electron microscopy and microanalysis.
RESULTS Single and clusters of particles were seen in AM from all children. The percentage of particle-containing AM ranged from 1% to 16% per child. Particles consisted of a carbonaceous core and all were ultrafine (<0.1 μm). Other elements such as metals and silicon were not detected. The percentage of particle-containing AM did not change with age, but was increased in children whose parents lived on a main road compared with those living on a quiet residential road (median 10%v 3%, p = 0.014).
CONCLUSIONS All children had AM containing ultrafine carbonaceous particles. The predominant source of these particles is most likely to be from the combustion of fossil fuels.
- alveolar macrophages
- ultrafine particles
- pollution
- children
Statistics from Altmetric.com
One of the major air pollutants associated with adverse respiratory health is particulate matter <10 μm diameter (PM10), the most important source of which is road traffic.1 PM10 represents a heterogeneous distribution of particles ranging from coarse (<10–>2.5 μm) and fine (<2.5–>0.1 μm), to ultrafine (UF, <0.1 μm). Primary PM10 emitted by traffic is composed of a carbonaceous core surrounded by organic and inorganic material.2 Children may be especially susceptible to its adverse effects since the modelled deposition of respirable particles is increased compared with adolescents and adults.3
Attention has recently focused on the toxicity of the UF fraction of PM10.4 However, the intercorrelation between the different size fractions contributing to PM10 makes it difficult in epidemiological studies to identify the component causing respiratory disease. One way of resolving this uncertainty would be to analyse the size and composition of particles within the lower airway of normal subjects. Alveolar macrophages (AM) move on the air/tissue interface of the lung and are a natural reservoir for inhaled material.5 Furthermore, substantial numbers of UF particles have been reported in AM from three non-industrially exposed healthy adults.6 In the present study we aimed to use the phagocytic capacity of AM to identify which environmental particles impact on the bronchoalveolar surface of normal children. We also aimed to generate preliminary data on whether exposure to road traffic influences exposure of the lower respiratory tract to particles.
Methods
Children with no respiratory symptoms undergoing elective surgery were recruited for bronchoalveolar lavage (BAL). BAL fluid samples were excluded from analysis if there were insufficient cells for analysis or if bacteria were present. Parents were asked: “is your home on a busy main road, or is it on a residential street/ quiet road?” The study had ethics committee approval and written informed consent was obtained from parents of all children participating in the study. Where appropriate, verbal consent was obtained from the child.
Immediately after intubation children underwent non-bronchoscopic BAL as previously described.7 Briefly, 1 ml/kg body weight of sterile saline at room temperature was instilled via a wedged suction catheter and immediately aspirated into a suction trap. The procedure was repeated twice (total instilled volume 3 ml/kg, maximum total 60 ml). The cell differential count was determined on cytocentrifuged BAL fluid (Shandon, Runcorn, Cheshire, UK) stained with Diff-Quik (Dade Behring, Deerfield, IL, USA). The BAL fluid cell differential count was determined by counting >300 leucocytes by light microscopy. For electron microscopy, BAL fluid was centrifuged at 250g for 5 minutes at 4°C. After removal of the supernatant the cell pellet was resuspended in phosphate buffered saline. This procedure was repeated twice. The cell pellet was then resuspended in fixative (2% glutaraldehyde with 0.1 M cacodylate buffer, pH 7.3) and repelleted at 8000g for 10 minutes. Fixation of the resulting pellet was continued for at least 24 hours before postfixation with 1% osmium tetroxide, dehydration, and embedding in Taab epoxy resin (Taab Ltd, Aldermaston, UK). Sections were cut perpendicular to the base of the pellet.
100 nm thick sections of AM were mounted on titanium grids and examined unstained in a Jeol 100-CXII electron microscope (Jeol Ltd, Welwyn Garden City, UK) at ×100 magnification to identify suitable areas for analysis. The selected area was then examined at a magnification of ×5800 to locate particles. Single sections from 100 different AM were examined for each child. The percentage of particle-containing AM was determined for each child, and particle size was measured by comparison with reference standards.
The composition of the particles was determined by microanalysis. Firstly, the elemental composition of particle aggregates >500 nm in diameter was determined by Energy-Dispersivex ray spectrometry in the Jeol electron microscope at 80 kV using a Model 860-2 system (Oxford Instruments, High Wycombe, UK). Secondly, serial sections (<50 nm thick) were examined unstained in a Zeiss 902A electron microscope (Leo Electron Microscopy Ltd, Cambridge, UK) using electron spectroscopic imaging and analysed by electron energy loss spectrometry.
DATA ANALYSIS
Data were analysed using a statistical package for microcomputers (Minitab release 13.1, PA, USA). Significance was tested using the Mann-Whitney U test and associations by Spearman rank correlation. A p value of <0.05 was considered statistically significant.
Results
Twenty nine BAL fluid samples were excluded prior to analysis because of insufficient numbers of AM or bacterial contamination. AM from the remaining 22 children (age range 3 months to 16 years) were examined by electron microscopy. Seven children lived on a main street and 15 children lived on a quiet residential road. The BAL fluid leucocyte differential was within the normal paediatric range in all children.7
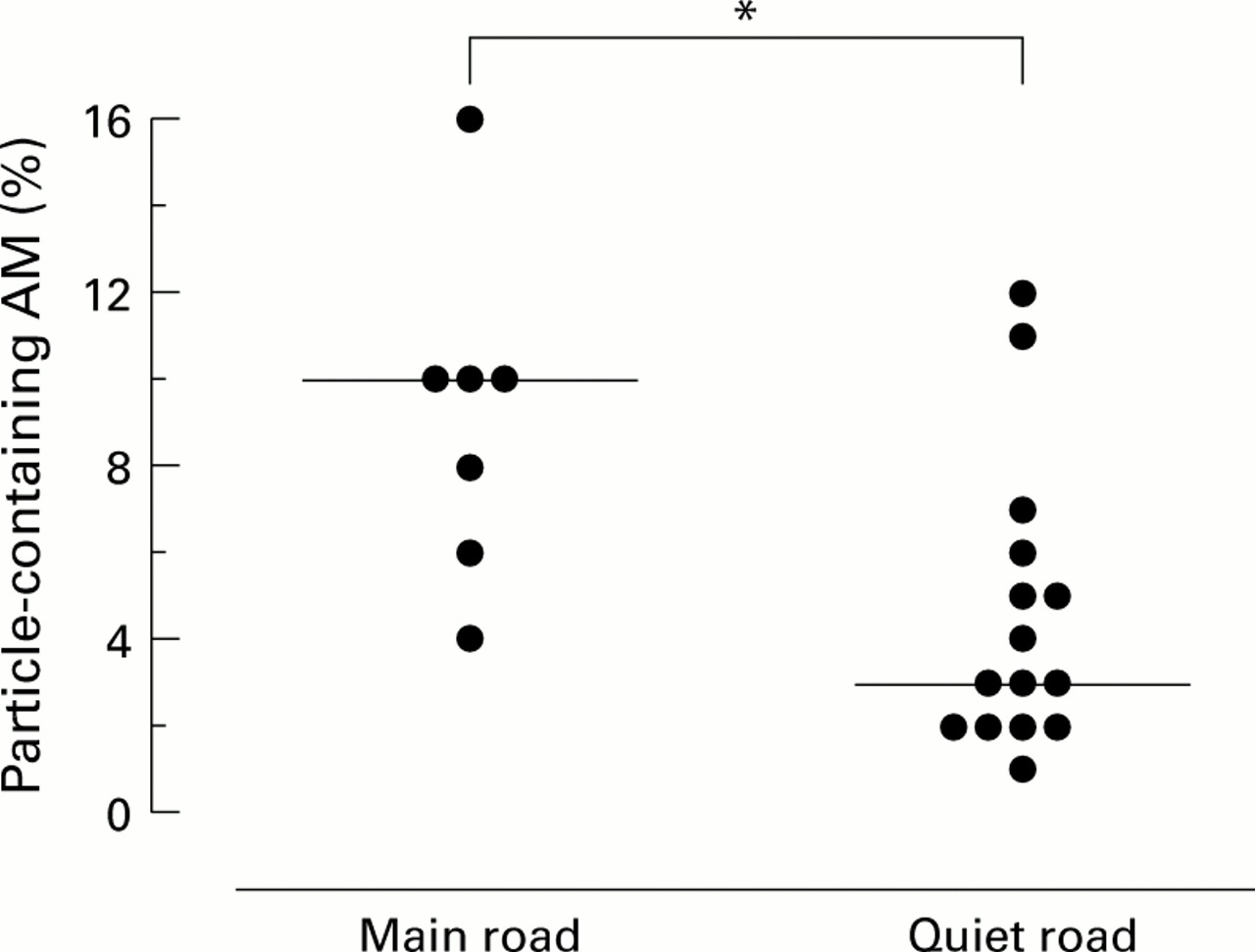
AM containing environmental particles were seen in all children. The percentage of particle-containing AM ranged from 1% to 16% per child (median 5%). All particles were ultrafine (<0.1 μm diameter) and were present either singly or as aggregates (fig 1). Microanalysis showed that all particles were carbonaceous. Metals and silicon were not detected. Particles collected from ambient Leicester city air and embedded in resin were indistinguishable in size and composition from those found within paediatric AM (data not shown). There was no correlation between age and the percentage of particle-containing AM. The percentage of particle-containing AM was significantly higher (p =0.014) in children living on a main road than in those living on a residential street (10% versus 3%, confidence interval for median difference 1.0 to 7.9; fig 2).

Elecronmicrograph showing carbonaceous ultrafine particles within a phagosome of an alveolar macrophage from a child aged 3 months. Bar = 1000 nm.
{kind=link}
{kind=link}
Percentage of particle-containing alveolar macrophages from children living on a main road and those living on a quiet road/residential street. *p<0.05 versus living on a main road (Mann-Whitney U test). Horizontal bars represent median values.
Discussion
This study presents the first conclusive evidence that carbonaceous particles are deposited in the lower airway of normal children. Furthermore, the ultrafine carbonaceous composition of the particles in AM strongly suggest that they are derived from road traffic.8 Since all of the particles in paediatric AM were composed of UF elements, these data are consistent with the selective penetration of smaller size fractions of PM10 into the distal airway,9 and the hypothesis that UF particles are a major determinant of the adverse health effects associated with PM10.4 However, it is possible that children have also inhaled agglomerations of UF particles which have subsequently disaggregated within AM in vivo. Metals are a common component of PM10 10 and are regularly encountered in samples from ambient air and from adult patients examined in our laboratory (data not shown). The absence of any metal compounds associated with particles within paediatric AM is therefore surprising. We speculate that some metals have leached from carbonaceous particles either in AM in vivo or during resin embedding.
An inhalation study has reported a 35% increase in the rate of deposition of 2 μm particles (normalised for lung surface area) in the lower airway of children compared with adolescents and adults.3 However, we found that the proportion of particle-containing AM did not change across the paediatric age range. Under normal exposure conditions other variables such as activity level and time spent outdoors may therefore confound any developmental change in deposition. By contrast, we found that the percentage of particle-containing AM was higher in children living on a main road, a finding compatible with the epidemiological association between increased road traffic density near the home and respiratory symptoms in children.11 The excluded samples are unlikely to have biased this observation since the proportion of excluded children living on a main road was similar to the study group.
In summary, AM from normal children contain particles, the size and composition of which suggest a fossil fuel origin. The association of an increased proportion of AM containing particles with increased traffic density near the home provides preliminary evidence for a direct relationship between exposure of the paediatric lower airway to particles and proximity to road traffic.
Acknowledgments
The authors are grateful to Judy McWilliam for preparing samples for electron microscopy and to Neil Cooper of the Pollution Control Group, Leicester City Council, AEA Technology and the DETR for the supply of ambient particle samples. Thanks are due to the Henry Smiths Charity and Medisearch for funding this work, and the paediatric surgeons and anaesthetists of the Leicester Royal Infirmary.