Article Text

Abstract
BACKGROUND Small cell lung cancer (SCLC) represents about 20% of primary lung tumours and the costs associated with the management of SCLC can be significant. The main objective of this study was to obtain information on current patterns of care and associated resource use and costs for patients with SCLC from initial diagnosis and treatment phase, throughout disease progression and terminal care.
METHODS A 4 year retrospective patient chart analysis (1994–7) was conducted on a consecutive series of 109 patients diagnosed with SCLC in two Newcastle hospitals. For this consecutive series of patients all details about care received including tests and procedures, treatment, and medication from diagnosis till death were recorded. Pathways of care and forms were designed to enable resource use to be captured for different disease phases. Unit costs were determined from a variety of sources including the Newcastle Hospitals NHS Trust Finance Department and the British National Formulary.
RESULTS The average total cost per patient calculated for the full cohort of 109 patients was £11556. Initial treatment was the most resource use intensive constituting 48.2% of the total cost. The major cost element throughout all disease phases was hospitalisation. Twenty eight percent of the total costs of care occur after recurrence of the disease until death, of which 73% are generated by terminal care.
CONCLUSION The results of this retrospective medical chart analysis show that the costs of care of SCLC are considerable, although the variability between patients in terms of the type and quantity of resource use is very high. Analyses such as this provide a useful insight into resources used in actual clinical practice.
- small cell lung cancer
- cost analysis
- resources
Statistics from Altmetric.com
Small cell lung cancer (SCLC) represents about 20% of primary lung tumours and the costs associated with its management can be significant. A review of the literature on the cost of managing SCLC produced 13 papers with relevant information. The most comprehensive analyses were from Canada1 ,2 and Australia.3 ,4 Seven US studies were found using data from a variety of health insurance organisations.5-11The only European studies with most data on SCLC were not primarily focused on the management of the disease. A Dutch study12 compared diagnostic methods and the one UK study13 was concerned with the use of granulocyte colony stimulating factors in patients with lung cancer.
In the absence of comprehensive studies of the costs associated with SCLC in the UK, the main objective of our analysis was to obtain information on the current patterns of treatment and the associated resource use and costs for patients with SCLC. Resource use was linked to phase of the disease, from initial diagnosis and treatment until confirmation of disease progression and terminal care. In this way a time profile of expected resource use could be constructed as a basis for subsequent comparison with similar data on new treatments for SCLC.
Methods
The complexity of this study required a multi-step approach. Firstly, the study sites were selected and a focus group meeting was conducted with clinicians to clarify the pathways of care and to agree on the design and implementation of forms for retrospective data extraction from the clinical records. Secondly, detailed data were collected from the medical records. Thirdly, patient resource use data were entered in a database and unit costs of all resource use items were collected. Finally, resource use data were analysed in association with appropriate unit costs. Details of the methods that were employed are given below.
STUDY DESIGN
The Freeman Hospital and Royal Victoria Infirmary in Newcastle upon Tyne were selected as the study sites for data collection. A focus group meeting was conducted to clarify the expected pathways of SCLC care to allow the design and implementation of forms for retrospectively recording data extracted from the clinical records. The focus group included a lead clinician, three respiratory physicians, one clinical oncologist, one palliative medicine specialist, and one lung cancer nurse.
It was decided that a suitable time frame for the retrospective study of patient management would be from 1994 to 1997. This would allow retrospective tracking of the full course of the disease for patients in a period without major changes in treatment approaches.
For the purposes of the study, a patient was assumed to progress through various phases of disease management. Drawing on the results of the literature review, a characterisation was made of the different steps in the diagnostic and treatment process. The group of clinicians agreed that management of all patients generally involves a mixture of active intervention and palliative care. The type of treatment would be determined more by the patient's performance status, general health, and preferences than just by time since diagnosis and stage of the disease.
The following separate steps in the management process that were considered to have different resource implications were identified:
Referral and diagnosis
Active treatment (chemotherapy and radiotherapy)
Follow up until relapse
Re-treatment
Follow up until further progression
Terminal care
This approach allowed a breakdown of the constituent costs of the different disease phases of SCLC, and consequently gives a greater insight to the potential impact of different treatment regimens administered to patients. The sections of the forms included the most likely items of resource use at each stage with space for less frequent items.
The data collection forms were pilot tested and some minor adjustments were made. The revised forms were used to record information on the full cohort.
DATA COLLECTION AND PLAN OF ANALYSIS
All patients diagnosed with SCLC at the Freeman Hospital and Royal Victoria Infirmary during 1994–7 were eligible for this retrospective chart analysis. For this consecutive series of patients, all details about care received including tests and procedures, treatment, and medication from diagnosis till death were recorded.
At completion of data collection the per patient data were entered into a database using the software program of the Centre for Disease Control and Prevention and the World Health Organisation public health data entry program Epi info 6 (Epi 6). All data were analysed in SAS and the results were transferred into Excel.
Analyses were made by disease phase including the following type of resource use:
Total number of days of hospitalisation stratified according to type of ward
Total number of outpatient visits stratified according to type of clinic
Total number of investigations according to type of investigation
Total number of laboratory tests according to laboratory test type
Total doses of chemotherapy according to chemotherapy drug
Total doses of drugs for the management of side effects and/or other medical therapies
Total number of radiotherapy fractions
Total number of hospice day visits and inpatient days
Total number of community nursing visits
Total number of social service support consultations
To allow the quantities of resource use to be translated into costs of treatment, the unit cost of each item of resource use was collected from a number of sources.
Inpatient hospitalisation
Costs per bed day according to ward type were obtained directly from the Newcastle Hospitals NHS Trust Finance Department.
Outpatient visits
The cost per outpatient consultation according to ward/physician type was obtained directly from the Newcastle Hospitals NHS Trust Finance Department.
Investigations, procedures, radiotherapy, blood transfusions, and surgery
The unit costs for these were collected from a number of sources including published literature, internal MEDTAP reports and databases, and directly from the Newcastle Hospitals NHS Trust Finance Department.
Chemotherapy, maintenance and side effect medication
All drug unit costs were calculated from the British National Formulary (1998–9 costs). For each drug the cost was calculated as either cost per μg, mg, g, or ml, as appropriate. When more than one formulation of a drug was listed, the cost of a generic version was taken in preference to the proprietary drug costs where possible. Where this was not possible, judgement was used to find the proprietary drug which is either most commonly prescribed or the cost of which reflects the median cost of the proprietary drugs available. There was no need to add a hospital administration charge to these costs as all such charges are incorporated into the hospitalisation bed day costs.
Hospice and community nursing
The hospice costs (both day visits and inpatient stays) were obtained directly from two hospices used by the patient cohort. Similarly, community nursing costs were supplied directly by the local providers.
Social work support
Costs for each type of service were calculated on a per patient basis by the service providers.
The average cost per patient was calculated, as well as the minimum and maximum costs of treatment for each treatment phase on a per patient basis. Patients who received the least and most resource intensive regimens per treatment phase were identified and their total costs calculated. Finally, the total costs and average costs per patient were calculated per treatment phase and for the major categories of resource use.
Results
PATTERNS OF CARE
Diagnostic phase
All patients had routine haematology and biochemistry tests, and urine analysis was usually done by dipstick. Histological or cytological diagnosis was on samples taken by fibreoptic bronchoscopy, fine needle aspiration, or mediastinoscopy. Staging was on clinical and chest radiographic findings, aided by ultrasonic or computed tomographic examination. If a patient was to have intravenous chemotherapy, renal function was examined before starting treatment.
First line treatment
For those patients with good performance status, initial chemotherapy consisted of intravenous carboplatin (dose in mg = 5 × glomerular filtration rate by 51Cr EDTA clearance + 25) on day 1 and oral etoposide 50 mg twice daily from day 1 for 5–10 days administered on a 4 week cycle to a maximum of six cycles.14 ,15 Anti-emetics were given at each cycle if nausea and vomiting occurred.
Between cycles patients were monitored at a weekly clinic visit which included haematological tests and chest radiography 1 week before each treatment cycle. Side effects sometimes necessitated admission to hospital and haematological side effects such as thrombocytopenia and neutropenia required administration of intravenous antibiotics and limited use of granulocyte colony stimulating factor (G-CSF). Anaemia was mainly treated with blood transfusions and occasionally by recombinant human erythropoietin.
Patients with limited disease and a good partial response were given mediastinal radiotherapy (four treatments on alternate days to a total of 20 Gy) and possibly prophylactic cranial irradiation (10 daily treatments over 2 weeks to a total of 30 Gy). Patients with extensive disease received in principle the same types of management as those with limited disease if their condition allowed, but did have more palliative care from the outset. Those with good performance status received chemotherapy but did not receive prophylactic cranial radiotherapy. Radiotherapy was used for the palliation of bone pain.
Follow up
Once the initial treatment was finished, patients made regular follow up visits to the clinic. Tests consisted mainly of chest radiographs with regular visits to a chest physician.
Recurrence and second line treatment
If recurrence of the disease occurred more than 1 year after first line chemotherapy, the same regimen was likely to be tried again before switching to an alternative regimen. The alternative regimen during the study period was intravenous vincristine 1.4 mg/m2 to a maximum dose of 2 mg, intravenous doxorubicin 45 mg/m2, and intravenous cyclophosphamide 1 g/m2 all on day 1 of a 21 day cycle, repeated for up to four cycles. In case of distant metastases, radiotherapy was used. Surgery was only used for specific indications such as shunts for obstructive hydrocephalus, bronchial stents and intravascular stents.
Terminal care
Bone pain was treated with radiotherapy and/or intravenous bisphosphonates, spinal cord compression mainly with radiotherapy and steroids. Short stays in hospital or hospice became more frequent over time once the disease became progressive. The palliative care service provided support for patients at home through district nurses, palliative care physicians, dietary advice, and psychological support. Social services provided in home assistance of various kinds and day hospice care was also available.
UNIT COST DATA
Over 250 separate items of resource use (procedures, tests, medicines) were identified in the study and unit costs were collected for each individual item. The most important unit costs used to convert the resource use estimates to costs are listed in table 1.
Key unit costs data
PATIENT CHARACTERISTICS AND COURSE OF THE DISEASE
The case notes were retrieved for 109 patients, 53 of whom were female. The median age at diagnosis was 66.4 years (interquartile range 58–73). The time course of each phase of the disease is shown in table2. Seventy four patients had two or more cycles of carboplatin and etoposide, 63 patients had four or more cycles, and 47 patients received a full six cycles.
Patient distributions and duration of disease phases
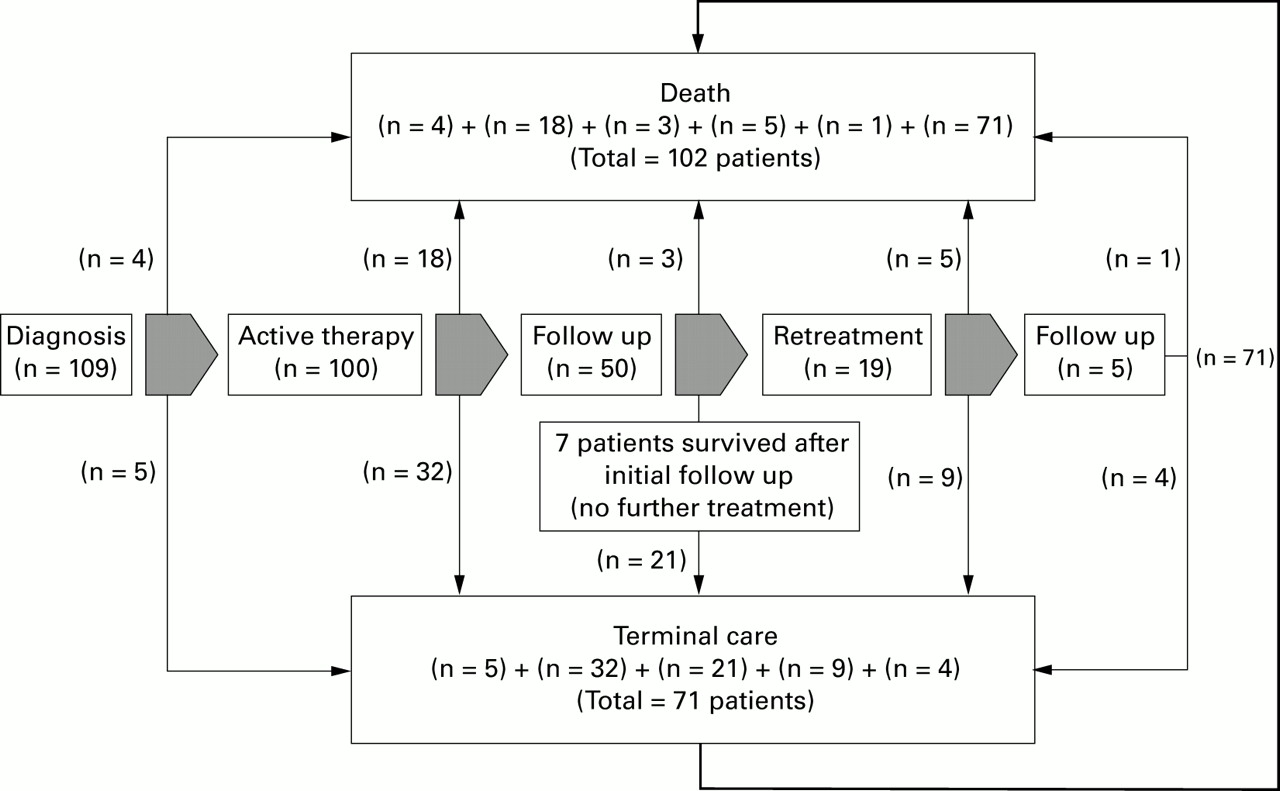
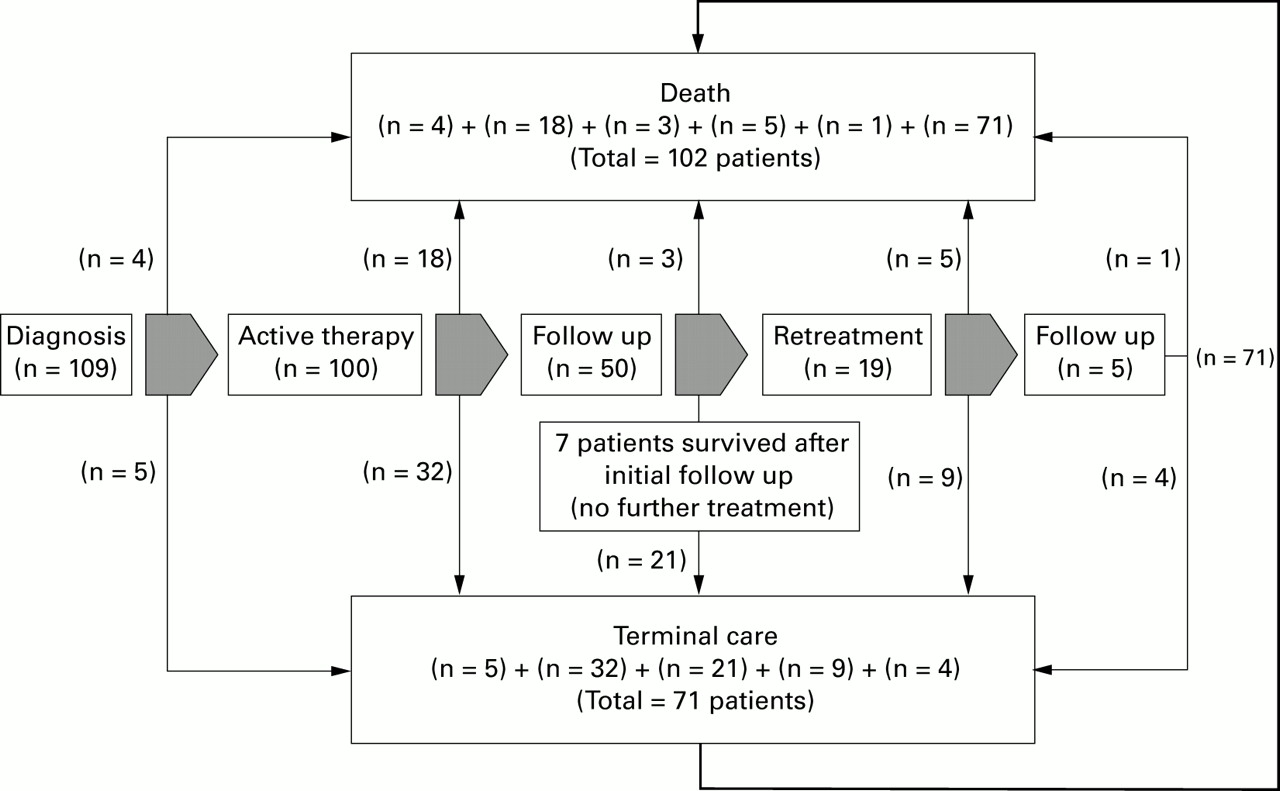
Figure 1 shows a flow chart of the cohort distributions according to phases of the disease. Of the full cohort of 109 patients who were diagnosed with SCLC during the period 1994–7, 102 had died by the end of 1997. Seven patients were still alive at the time of data collection. Most patients who progressed to terminal care did so after having received active treatment (n=32) or during the first follow up period (n=21). Most patients (n=71) received a defined period of terminal care before death.
{kind=link}
Flow chart of treatment phases and distribution of cohort.
TOTAL COSTS
The total cost, calculated by multiplying the measured quantities of resources used by their unit costs, is presented in table 3. By far the major cost element was hospitalisation, while outpatient visits, chemotherapy, and tests and procedures also contributed significantly. Management of side effects of treatment, radiotherapy, surgery, other medication, and blood transfusions played a relatively small part in the costs of management of patients with SCLC. The average total cost per patient calculated for the full cohort of 109 patients is £11556.
Overall disease costs by resource type
COSTS PER TREATMENT PHASE
Table 4 shows the mean costs per patient during each treatment phase, with the range of values and the costs adjusted for the number of patients in each phase. The breadth of the ranges is a consequence of the variability of length of hospital stay, which ranged from 0 to 30 days for referral and diagnosis, 0 to 89 days for active treatment, and 0 to 84 days for follow up. The average costs per patient reaching each stage were highest for first line treatment and second line treatment at £6128 and £5008, respectively. This is indicative of the typical cost of a course of chemotherapy treatment, although some of the patients in the re-treatment group received more than one extra course of chemotherapy.
Overview of cost per disease phase
Table 5 lists the actual costs per treatment phase broken down over the major categories of resource use and their percentages. For all but one phase of the disease (follow up after second line treatment), hospitalisation was the major cost driver. In the final phase of the disease hospitalisation for terminal care accounted for 77% of all costs.
Distribution of costs by disease phase and type of resource use
SOCIAL SERVICES DATA
Patients with SCLC may receive care outside the hospital, especially when the disease progresses, the patient's health deteriorates, and active treatment is no longer an option. We were able to collect data on care funded by hospices, the community, and social services from 56 patients. Of these patients, 24 received some form of social care. Although these costs may be important in individual cases, their inclusion in the overall cost analysis added only 3% to the average per patient cost.
The uncertain representativeness of this sample of 56 patients for which we could collect social services data, as well as the fact that we did not have data on all types of extramural care (such as care that these patients have received from general practitioners), we decided to exclude these data from the overall cost calculation.
SENSITIVITY ANALYSIS ON UNIT COSTS
Resource costs are known to vary considerably between hospital sites in the UK. As a result, the generalisability of data collected in single site studies is sometimes called into question. In our study most of the unit costs used in the main analysis came from the hospital finance departments and are therefore subject to local accounting conventions.
For these reasons we carried out a second analysis using unit costs from national average data. Sources used for this analysis are the Chartered Institute of Public Finance and Accountancy (CIPFA),16 Personal Social Services Research Unit (PSSRU),17 and the NHS reference costs 2000.
The sensitivity analysis did not change the results with regard to the relative costs of different treatment phases, but the absolute cost levels using the national figures were higher. This was largely due to lower local costs of hospitalisation and laboratory tests in Newcastle compared with the national average.
Discussion
In this retrospective study we collected full details of the type and quantity of care of 109 patients diagnosed with SCLC during 1994–7 in two hospitals in Newcastle upon Tyne. As expected, the medical charts data revealed significant variation in both type and quantity of care and resource use. The major cost driver for SCLC treatment in this study was hospitalisation. The per patient direct costs of SCLC care peaked in the months immediately following diagnosis and in the final months of life due to extensive and relatively expensive diagnostic procedures in the early phase of the disease, initial treatment, and intense care during the last phase of the disease. Patients with advanced disease at diagnosis generally incurred lower treatment costs than patients diagnosed with less extensive disease due to rapid progression and short survival time.
Although the variability between patients in terms of length of life with SCLC and resource use was very high, the results of this cohort of 109 patients showed that active treatment accounted for 48.2% of the total cost of care. Twenty eight percent of the total costs of care occurred after recurrence of the disease until death, of which 73% were generated by terminal care. However, it should be noted that the terminal care figures in the report are an underestimation of the costs as the care received by patients outside hospital was not included in this analysis. The partial dataset available on the earlier patients in the cohort indicated that the inclusion of these costs could increase the post-recurrence costs by approximately 10%.
To our knowledge, this study is the first attempt to produce a comprehensive overview of the cost borne by the hospital sector associated with the management of patients with SCLC in the UK. In the absence of other similar studies, a comparison of data is not possible and it is difficult to judge the generalisability of the results to other areas or to the whole of the UK. This study was undertaken in a well defined geographical area with all patient services well coordinated. The management of care in Newcastle upon Tyne is organised around the hospitals with follow up appointments as well as active treatment being undertaken in hospital rather than a hospice or other community setting. This greatly facilitated data collection and ensured a comprehensive overview of the cost associated with the management of patients with SCLC in this area.
Since most of the care of patients with SCLC was hospital based, the results are highly dependent on the accuracy of the unit costs assigned to hospital stays and outpatient visits. The true marginal cost of a hospital stay varies with the length of stay—that is, the first day is more expensive than the 20th—because of variations in tests and procedures and nursing intensity. In our study we tried to separate the “hotel” costs of hospitalisation, which do not vary with length of stay, from the tests and procedures by costing these separately. Although several patients had prolonged hospital stays, this was generally because they were in need of constant care (particularly in dealing with side effects of treatment and in the terminal care phase). The use of average hospital hotel costs may therefore not be a serious problem in this case. If the figures were to be used in a comparative evaluation of different treatments where the hospitalisation rate is variable between comparators, then this issue would have to be further examined.
This retrospective study is based on treatment patterns used recently in Newcastle and on local unit costs. To generalise from these results to the whole of the UK requires comparative data on treatment patterns and unit costs in other centres. Sensitivity analysis carried out on the unit costs indicated that replacement of local Newcastle unit costs with national equivalents had little impact on the results. The most important determinant of resource use is therefore likely to be the pattern of care provided. Before making any claims on the generalisability of the results of this study, one would have to investigate whether the treatment pattern seen in our study is representative of the (current) national approach. Further research of treatment patterns and resource use at other UK cancer centres would be a valuable extension of this study.