Article Text

Abstract
BACKGROUND Cystic fibrosis (CF) is the most common life threatening autosomal recessive disorder in the white population. Wasting has long been recognised as a poor prognostic marker in CF. Whether it predicts survival independently of lung function and arterial blood gas tensions has not previously been reported.
METHODS 584 patients with CF (261 women) of mean (SD) age 21 (7) years were studied between 1985 and 1996, all of whom were being followed up in a tertiary referral centre. Lung function tests, body weight, arterial blood oxygen (Pao 2) and carbon dioxide (Paco 2) tensions were measured. The weight was calculated as a percentage of the ideal body weight for age, height, and sex.
RESULTS Forced expiratory volume in one second (FEV1) recorded at the start of the study was 1.8 (1.0) l (52 (26)% predicted FEV1), Pao 2 9.8 (1.9) kPa, Paco 2 5.0 (0.9) kPa, and % ideal weight 92 (18)%. During the follow up period (45 (27) months) 137 patients died (5 year survival 72%, 95% CI 67 to 73). FEV1, % predicted FEV1, Pao 2, % ideal weight (all p<0.0001), and Paco 2 (p=0.04) predicted survival. In multivariate analysis, % predicted FEV1 (p<0.0001), % ideal weight (p=0.004), and Paco 2 (p=0.02) were independent predictors of outcome. Patients with >85% ideal body weight had a better prognosis at 5 years (cumulative survival 84%, 95% CI 79 to 89) than those with ⩽85% ideal weight (survival 53%, 95% CI 45 to 62), p<0.0001. Percentage predicted FEV1 (area under curve 0.83; 95% CI 0.78 to 0.87) and % ideal weight (area under curve 0.74; 95% CI 0.68 to 0.79) were accurate predictors of survival at 5 years follow up (receiver-operating characteristic analysis).
CONCLUSIONS Body wasting is a significant predictor of survival in patients with CF independent of lung function, arterial blood oxygen and carbon dioxide tensions.
- cystic fibrosis
- wasting
- survival
Statistics from Altmetric.com
Cystic fibrosis (CF) is the most common life threatening autosomal recessive disorder in the white population, occurring at a frequency of approximately 1:2000 to 1:2500 live births.1Advances in medical treatment have resulted in an improvement in prognosis and symptoms with increasing numbers of patients surviving into adult life. However, as the disease progresses, patients develop disabling lung disease with the main cause of death in adults being respiratory failure.2 For patients with advanced CF, lung or heart-lung transplantation represents an important treatment for improving survival and quality of life.3 In view of the shortage of donor organs and to assess the suitability of patients for transplantation, reliable prognostic indicators that can accurately define groups of patients at high risk are needed.
Wasting has long been recognised as a marker of impaired survival in CF,4 but it has not been previously shown to be independent of established prognostic indicators. Keremet al 5 showed that body wasting was predictive of impaired survival but this was not independent of lung function or arterial blood gas tensions. It has been demonstrated that cachexia is a strong and independent risk factor for mortality in patients with chronic heart failure,6 as well as other chronic diseases.7 ,8 We have examined whether body wasting is an independent prognostic marker in CF.
Methods
STUDY POPULATION AND FOLLOW UP
Between 1985 and 1996, 584 patients (261 female) with CF, of mean age 21 (7) years (range 7–45), who attended the Royal Brompton Hospital were studied. The diagnosis of CF was based on positive sweat tests with typical clinical findings, with or without genotype confirmation. The patients underwent routine testing of pulmonary function during their follow up, with forced expiratory volume in one second (FEV1) expressed as a percentage of the normal predicted values for height and sex (% predicted FEV1), as previously described.9 ,10 Height, weight, arterial blood oxygen and carbon dioxide tensions (Pao 2, Paco 2) were also measured. Weight was calculated as a percentage of the ideal body weight for age, height, and sex using the standards of Tanner et al 11 for patients aged ⩽19 years and the Metropolitan height and weight tables12 for patients >19 years of age.
As all the above investigations were part of the routine assessment of patients with CF attending our hospital, informed consent from the patients studied or ethics committee approval was deemed unnecessary.
STATISTICAL ANALYSIS
All results are presented as mean (SD) values. Cox proportional hazard analysis was performed using baseline values to assess the association between variables and all-cause mortality. Previous studies have shown that % predicted FEV1, age, and sex all relate to survival. The interaction between the effects of each of these variables and % ideal weight in determining survival was therefore evaluated initially in two variable models. Subsequently, these parameters (together with arterial blood gas levels) were included in a six variable model (table 3). Hazard ratio (RR) and 95% confidence interval (CI) for risk factors as well as significance levels for χ2 (likelihood ratio test) are given, and Kaplan-Meier cumulative survival plots were constructed (StatView 5, Abacus Concepts, Berkeley, USA). The receiver-operating characteristic curves for % predicted FEV1, % ideal weight, and Paco 2 were drawn and the areas under the curves calculated (MedCalc 5.0, MedCalc Inc, Belgium). The cut off level that resulted in the highest product of sensitivity and specificity was considered the optimal level for predicting outcome.
Cox proportional hazards analysis of survival in 584 patients with cystic fibrosis: multivariate analysis
The probability of death within 5 years of patients with CF (according to % predicted FEV1 and % ideal weight) was calculated using a logistic regression analysis technique.13
Results
Of the 584 patients who were followed up for a mean of 45 (27) months, 137 (23.5%) died after 2.4–89.9 months (mean 31.0 (21.0); median 25.0). The mean (SD) follow up period of the 447 survivors was 48.0 (27.1) months (range 1.6–94.7). The cumulative survival of all patients was 96.3% at 1 year (95% CI 94.7 to 97.9), 82.8% at 3 years (95% CI 79.4 to 86.2), 71.9% at 5 years (95% CI 67.3 to 76.5), and 62.7% at 7 years (95% CI 56.9 to 68.5). For all the 584 patients the mean FEV1 recorded at the start of study was 1.8 (1.0) l (52 (26)% predicted FEV1), Pao 29.8 (1.9) kPa, Paco 2 5.0 (0.9) kPa, and % ideal weight 92 (18)% (table 1).
Baseline clinical characteristics of 584 consecutive patients with cystic fibrosis (CF)
FEV1, % predicted FEV1, % ideal weight, Pao 2 (all p<0.0001) and Paco 2 (p=0.04) predicted survival (table 2). In multivariate analysis including these measurements, % predicted FEV1 (p<0.0001), % ideal body weight (p=0.004), and Paco 2 (p=0.02) were found independently to predict outcome after 5 years (table 3). Age and sex were not predictive of survival in univariate or multivariate analyses.
Cox proportional hazards analysis of survival in 584 patients with cystic fibrosis: univariate analysis
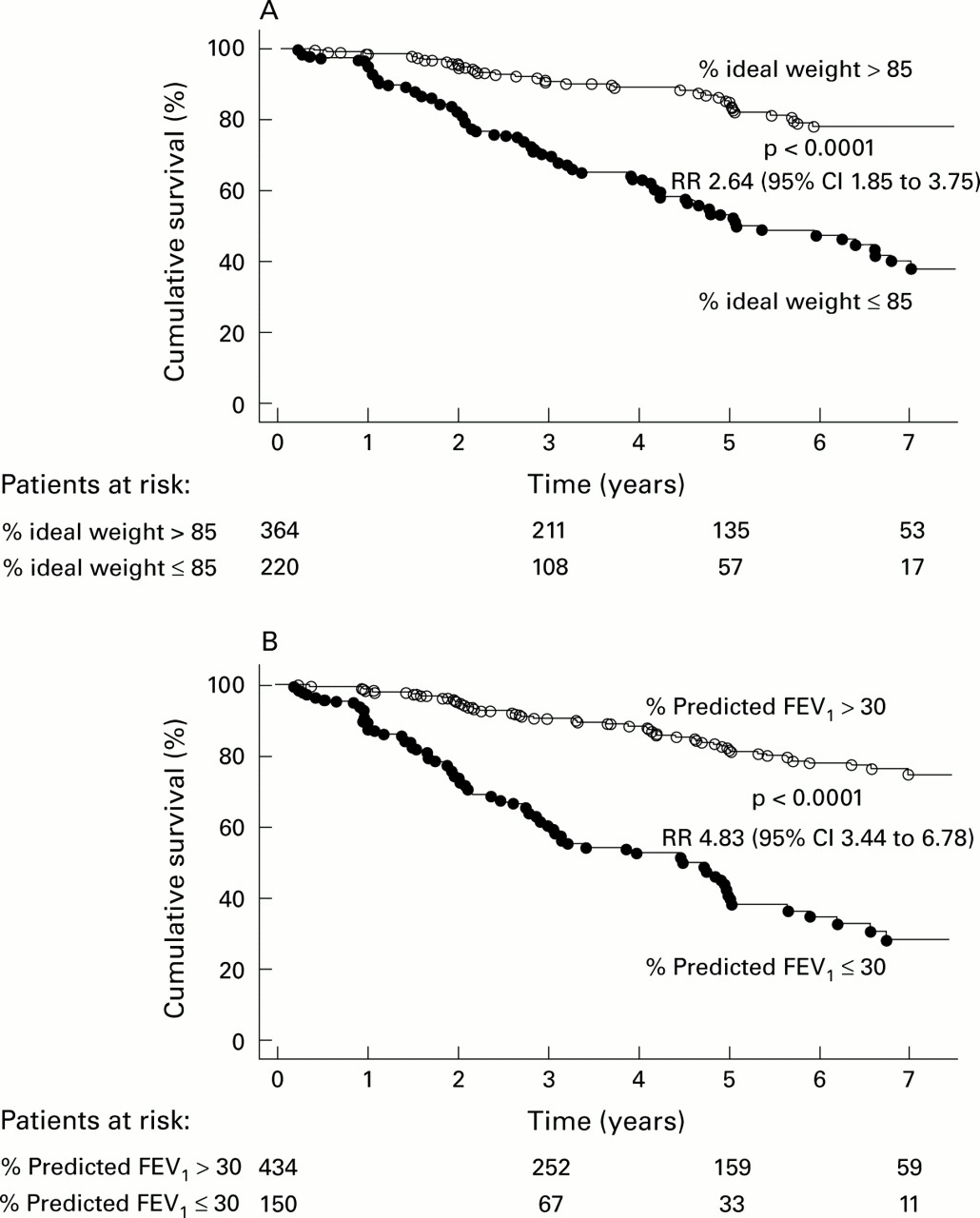
Kaplan-Meier survival analysis shows that patients with >85% ideal body weight had a better prognosis at 5 years (cumulative survival 83.8%; 95% CI 78.8 to 88.8) than those with ⩽85% ideal weight (survival 53.4%; 95% CI 45.2 to 61.6; p<0.0001, fig 1A). Furthermore, patients with FEV1 >30% predicted were found to have a significantly better prognosis than those with FEV1 ⩽30% predicted (fig 1B).

Kaplan-Meier survival plot for 584 patients with cystic fibrosis: patients subgrouped according to (A) percentage ideal weight and (B) percentage predicted forced expiratory volume in one second (FEV1).
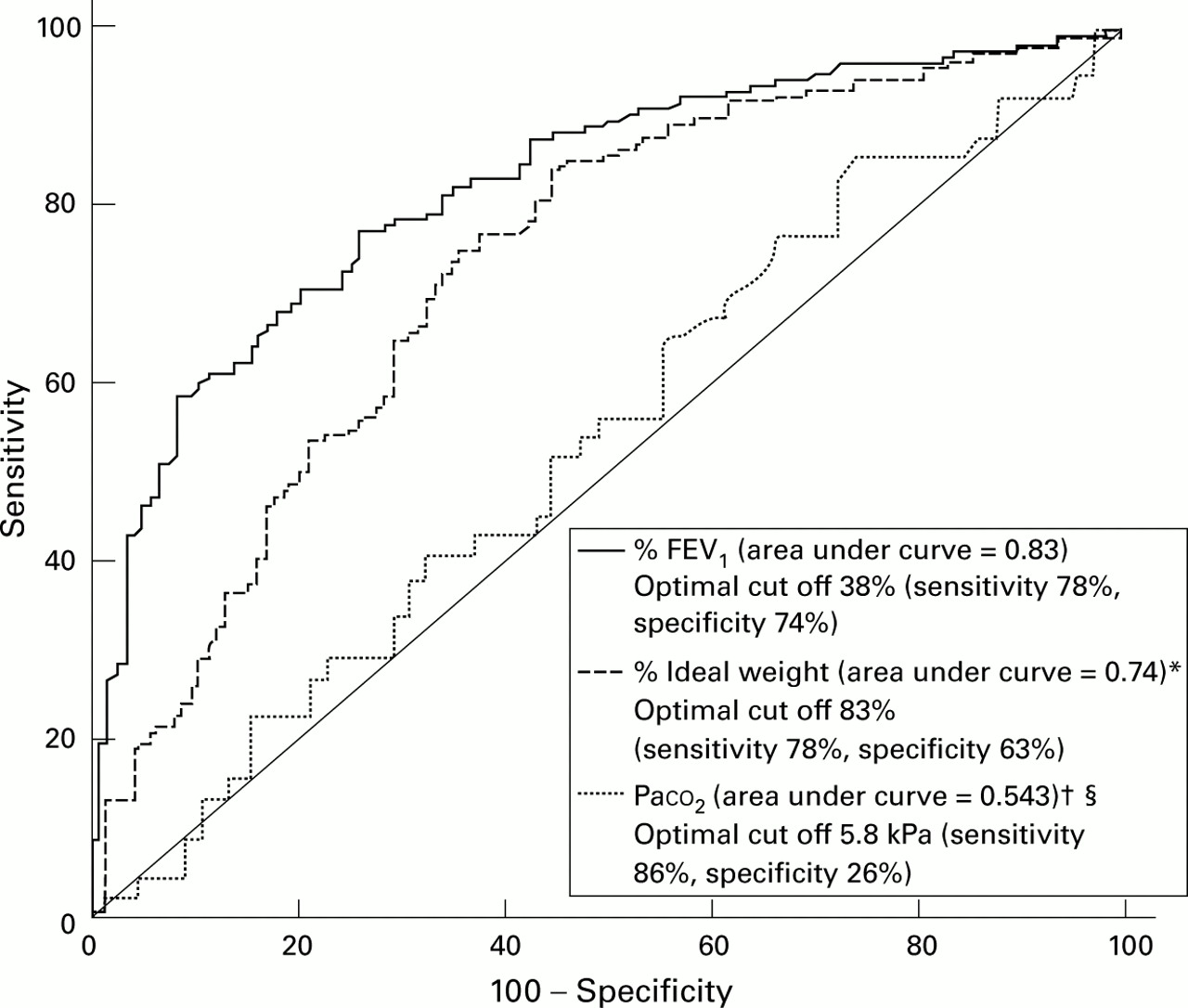
Receiver-operating characteristic (ROC) curves were plotted for % predicted FEV1, % ideal weight, and Paco 2 (fig 2). Both % predicted FEV1 (area under the curve 0.827; 95% CI 0.780 to 0.867) and % ideal weight (area under the curve 0.736; 95% CI 0.684 to 0.785) were found to be highly accurate predictors of 5 year survival, with the former being significantly better than the latter (p=0.002). In contrast, Paco 2 was not shown to be an accurate prognostic indicator (area under the curve 0.543; 95% CI 0.445 to 0.639). ROC curves were also drawn for 1, 2, 3, and 7 years follow up which resulted in similar results to those above (data not shown). The optimal cut off value for predicting death at 5 years was 38% for predicted FEV1 and 83% for ideal weight.

Receiver-operating characteristic curves of 5 year survival for percentage predicted forced expiratory volume in one second (FEV1), % ideal weight, and Paco 2 in patients with cystic fibrosis. *Percentage ideal weight v percentage predicted FEV1: p = 0.002; †percentage ideal weight v Paco 2: p = 0.011; §Paco 2 v percentage predicted FEV1: p<0.0001.
The probability of death within 5 years was estimated according to % predicted FEV1 and % ideal weight (fig 3). For any given % predicted FEV1, the probability of death was found to increase markedly as the % ideal weight decreased. The probability of death within 2 and 7 years was also calculated, resulting in similar findings (data not shown).

Estimated probability of death within 5 years of patients with cystic fibrosis according to percentage predicted FEV1 and percentage ideal weight.
Discussion
This study has shown that body wasting is an important predictor of impaired survival in CF. It provides prognostic information independently of established risk factors such as lung function (% predicted FEV1) and arterial blood gas tensions (Pao 2 and Paco 2). Although it has long been recognised that wasting is a predictor of survival in CF,4 it has not been previously shown to be an independent prognostic indicator.
In a study by Kerem et al,5 % ideal weight was not found to be an independent predictor of survival, in contrast to the present study. One reason for this may be that our data are more recent (patients followed up between 1985 and 1996) than those of Kerem et al (patients followed up between 1977 and 1989). During the last two decades there have been major improvements in the nutrition of patients with CF, with the introduction of high calorie diets and the development of better pancreatic enzymes in the mid 1980s.14 It may be hypothesised that, in the past, if a patient with CF was cachectic this was simply due to poor nutrition, which is why body weight was a relatively weak marker of disease severity in the study by Keremet al. However, since the advances in nutritional support, the development of weight loss (or failure to thrive in children) is likely to be due to a serious deterioration in the metabolic status of the patient as a result of the disease process itself. As a result, a low % ideal body weight has become a more powerful and independent predictor of survival in patients with CF who are managed using present day treatment strategies. It must be borne in mind that, as new therapies for chronic diseases emerge, the prognostic value of certain markers may change, as has been observed in other disease states.15
In the present study, age and sex were not significant predictors of mortality in CF. Although there have been some previous studies in which these parameters were found to be of prognostic value, there have also been several studies in which this was not the case.4 ,16-18 In particular, in one of the largest epidemiological studies to date in CF which investigated over 21 000 patients, sex was noted to be a significant predictor of mortality only in patients below 20 years of age.18 Furthermore, in the same study there was a trend within the 1–20 year age group for the relative risk to diminish with increasing age. As the mean age of our study population was 21 years, this may explain why we did not find sex to be a significant prognostic marker for CF.
One of the major problems of research into cachexia is in defining the degree of wasting. The body mass index is routinely used for assessing weight in relation to height in adults, but this method gives only limited information and cannot be applied to children. Instead, calculating the weight as a percentage of the ideal weight (according to height, age and sex) is more appropriate.11 ,12 ,19Percentage ideal weight measurements are generally considered superior to the % average weight of the respective populations when performing survival studies, as the former refer to the weight associated with the lowest mortality rate.20 The present study has shown that % ideal weight is a highly accurate prognostic indicator, with the optimal cut off level being 83% for predicting 5 year survival. This finding is in keeping with a consensus report on nutritional assessment in CF19 which defined nutritional failure as a % ideal weight of <85. The marked difference in survival between patients subdivided according to 85% ideal weight is shown in fig 1.
As % predicted FEV1 and % ideal weight were the only two risk factors that predicted death independently and accurately in our study, the probability of death within 5 years was estimated using a model based on these two variables (fig 3). Graphs were also constructed based upon the probability of death within 2 and 7 years which yielded similar results (data not shown). In fig 3, patients were divided into subgroups according to % ideal weight using a classification system modified from Waterlow and Rutishauser.21 The range of body size for normal nutritional status is 90–110% of ideal weight. Patients with 85.0–89.9% of ideal weight are defined as having early malnutrition, 80.0–84.9% as mild malnutrition, and <80% as moderate to severe malnutrition.19 From fig 3, the probability of death within 5 years can be estimated for any patient provided their % predicted FEV1 and % ideal weight are known, both of which can be readily assessed in the outpatient clinic. As a patient's nutritional status worsens, the probability of death for any given % predicted FEV1 increases markedly. The development of cachexia in CF should therefore be considered an ominous clinical sign. Interestingly, patients in our study who were overweight (>110% ideal weight) had a better prognosis than patients with normal nutritional status.
There are several reasons for weight loss in patients with CF, including uncontrolled malabsorption, the development of diabetes mellitus, or the progression of respiratory disease. Recurrent episodes of pulmonary sepsis can result in wasting due to an increase in metabolic rate and because the patient may become too breathless to eat properly. Cachexia is also known to be a poor prognostic sign in patients with other medical conditions such as cancer, AIDS, and chronic heart failure.6-8 Although there are different mechanisms responsible for the wasting process in these conditions, the common finding appears to be that cachexia is a strong predictor of impaired survival. Furthermore, it is known that improvements in nutrition can lead to increased survival of patients with CF. In a study comparing the survival rates of two large CF centres in North America, there was a higher median survival rate among patients in Toronto than in those in Boston because of better nutrition in the former centre.22
The present study shows that CF patients with wasting represent a high risk group which should be considered for transplantation at an earlier stage than patients who are not cachectic. Previous work has shown that preoperative body mass index does not influence survival following transplantation, suggesting that cachectic patients should not be denied transplantation unduly while attempts are being made to increase weight.17 Percentage ideal weight represents a simple and cost effective measurement which, in addition to % predicted FEV1, provides an accurate and independent prediction of prognosis in CF.
Acknowledgments
The authors are grateful to Ms J Turner for her statistical advice.
References

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Footnotes
RS is supported by the Robert Luff Foundation, APB and the Department of Cardiac Medicine are supported by the British Heart Foundation, AJSC is supported by the Viscount Royston Trust Fund, SDA holds a postgraduate fellowship of the Max-Delbrück-Centrum for Molecular Medicine, Berlin, Germany.