Article Text

Abstract
BACKGROUND The incidence of malignant mesothelioma is increasing. There is the perception that survival is worse in the UK than in other countries. However, it is important to compare survival in different series based on accurate prognostic data. The European Organisation for Research and Treatment of Cancer (EORTC) and the Cancer and Leukaemia Group B (CALGB) have recently published prognostic scoring systems. We have assessed the prognostic variables, validated the EORTC and CALGB prognostic groups, and evaluated survival in a series of 142 patients.
METHODS Case notes of 142 consecutive patients presenting in Leicester since 1988 were reviewed. Univariate analysis of prognostic variables was performed using a Cox proportional hazards regression model. Statistically significant variables were analysed further in a forward, stepwise multivariate model. EORTC and CALGB prognostic groups were derived, Kaplan-Meier survival curves plotted, and survival rates were calculated from life tables.
RESULTS Significant poor prognostic factors in univariate analysis included male sex, older age, weight loss, chest pain, poor performance status, low haemoglobin, leukocytosis, thrombocytosis, and non-epithelial cell type (p<0.05). The prognostic significance of cell type, haemoglobin, white cell count, performance status, and sex were retained in the multivariate model. Overall median survival was 5.9 (range 0–34.3) months. One and two year survival rates were 21.3% (95% CI 13.9 to 28.7) and 3.5% (0 to 8.5), respectively. Median, one, and two year survival data within prognostic groups in Leicester were equivalent to the EORTC and CALGB series. Survival curves were successfully stratified by the prognostic groups.
CONCLUSIONS This study validates the EORTC and CALGB prognostic scoring systems which should be used both in the assessment of survival data of series in different countries and in the stratification of patients into randomised clinical studies.
- malignant mesothelioma
- prognosis
- staging
Statistics from Altmetric.com
The incidence of malignant mesothelioma is increasing in the UK and the number of cases may treble over the next 20 years.1 ,2 Management in the UK generally involves little more than a closed or surgical pleurodesis, typically with talc. Surgical intervention has fallen in the UK over the last 10 years despite the increasing incidence of malignant mesothelioma. The UK Thoracic Surgical Register of the Society of Cardiothoracic Surgeons of Great Britain and Ireland recorded eight extrapleural pneumonectomies and 19 pleurectomies in 1998 compared with 35 and 88, respectively, in 1989. Chemotherapy for malignant mesothelioma is not common in the UK, although phase II studies indicate good symptom control3 ,4 and a phase III British Thoracic Society (BTS)/Medical Research Council (MRC) trial is planned. Radiotherapy is usually given to intercostal drain or thoracoscopy sites only, rather than as radical treatment to the hemithorax. Despite encouraging results for multimodality approaches combining surgery, radiotherapy and chemotherapy, no randomised studies have been performed and a survival benefit has not been established.5
The current nihilism towards malignant mesothelioma in the UK is due to the perception that therapeutic interventions have little to offer. Survival from time of diagnosis is typically 7–10 months6 ,7 which appears to be worse than the 12–19 months typically quoted in European and American series.8 ,9 It is not clear whether the apparent poor survival in the UK is a reflection of less aggressive management or later tumour stage at the time of diagnosis.
There have been increased efforts to devise accurate staging systems for malignant mesothelioma in recent years.10 The International Mesothelioma Interest Group (IMIG) staging system was proposed in 199511 and validated by Rusch and Venkatraman.12 However, the IMIG system was not successful as a survival predictor in the radical multimodality treatment series of Sugarbaker et al. 9 They amended the Brigham staging system to include assessment of resection margins and revised the nodal variable, but this surgical staging system is only applicable after extrapleural pneumonectomy. It is therefore difficult to assess the survival of the vast majority of patients with malignant mesothelioma in the UK by a Tumour/Nodes/Metastasis (TNM) staging system alone, although an accurate assessment of prognosis must be a central part of entry into future phase III trials.
Prognostic scoring systems have been proposed by the European Organisation for Research and Treatment of Cancer (EORTC)8and by the Cancer and Leukaemia Group B (CALGB).13 These systems were derived from statistical analysis of large series of patients within chemotherapy trials. Two EORTC risk groups were identified after multivariate analysis of prognostic variables from 204 patients entered into five consecutive trials. The factors included in the model were: white blood cell count >8.3 × 109/l, Eastern Cooperative Oncology Group (ECOG) performance status ⩾1, sarcomatoid tumour cell type, probable or possible histological diagnosis, and male sex. The high risk group was defined by the presence of three or more of these factors. The CALGB system is more complex and derives from the analysis of 337 patients. A regression tree leads to 11 groups of which those with similar survival characteristics are combined to form six prognostic groups.
We have analysed data from 142 patients with malignant mesothelioma presenting to the Cardiothoracic Surgical Service in Leicester since 1988. The aims of this study were to assess prognostic variables, to validate the EORTC and CALGB prognostic scoring systems, and to evaluate the survival data of our series when split into relevant prognostic risk groups.
Methods
DATA COLLECTION
The Department of Pathology at Glenfield Hospital provided a list of all pathological specimens with a diagnosis of malignant mesothelioma since 1988. Most of these cases represented patients passing through the Department of Cardiothoracic Surgery at Groby Road Hospital, and latterly Glenfield Hospital, Leicester. Patients were referred for surgical biopsy, management of pleural effusion or empyema, or radical surgery. Case notes were identified and original notes or stored microfilm copies were reviewed. Case notes from referring hospitals were also reviewed, where possible. Relevant demographic, clinical, and pathological data, as well as management and survival data, were retrieved and entered into a computer database (Microsoft Access). The detailed histopathological report was reviewed, but tissue sections were not re-examined as part of this study. From August 1998 data have been collected prospectively. Survival was calculated from the date of the diagnostic biopsy and pre-diagnostic variables such as performance status and haematological indices were taken from immediately before this time.
STATISTICAL ANALYSIS
Statistical analysis was performed using the SPSS software (SPSS Inc, USA). Complete data retrieval was only possible in 101 of the total of 142 patients because of missing or destroyed case notes, or missing data within case notes that had been inspected. Univariate analysis was performed on all 142 cases. All parameters were analysed as categorical variables except age which was assessed as a continuous variable. The cut off points chosen were based on those used in the CALGB and EORTC series. Haemoglobin and white cell count were also analysed as continuous variables. Survival curves were estimated using the Kaplan-Meier method. A Cox proportional hazards regression model14 was used to identify statistically significant differences in survival and to estimate hazard ratios and 95% confidence intervals (CI). The assumption of proportional hazards was assessed graphically by plotting log[–log(survivor)] against log(time) for each of the prognostic groups. In the case of the multivariate models the final model was re-estimated, stratifying for each variable in turn. Statistically significant variables identified by the univariate analysis, and for which data were complete (n = 101), were analysed in a multivariate model. A forward stepwise selection procedure was used, with variables being added to the model according to a partial likelihood ratio test using an entry criterion of p<0.05.
EORTC AND CALGB PROGNOSTIC SCORING GROUPS
The appropriate prognostic groups according to EORTC8and CALGB13 criteria were identified for each patient where relevant data were complete. Survival curves were plotted and median, one year, and two year survival rates were calculated from life tables, together with the respective 95% CI. Survival differences between, and hazard ratios for, each prognostic group were calculated using a univariate Cox model, as above.
Results
One hundred and forty two patients were identified (13 women, 129 men); survival data were available for 138 patients. The median age at the time of diagnosis was 64 years (range 42–86). The median time from onset of symptoms to hospital referral by the general practitioner (GP) was 4.3 weeks (range 1–74) and from GP referral to surgical referral was 3.7 weeks (range 0.1–58). Although closed pleural biopsy specimens were taken in 47 patients, this was the sole histological material in only eight cases. Immunohistochemistry was required in 56% of cases to confirm the diagnosis. The most commonly used markers were CEA, BerEP4, AUA-1, HBME-1, cytokeratin, thrombomodulin, and CAM 5.2 in 58, 54, 37, 29, 29, 29, and 23 cases, respectively. The time from surgical referral to the date of diagnostic biopsy was 3.0 weeks (range 0.1–122). Overall median survival from the date of histological diagnosis was 5.9 months (range 0–34.3). One and two year survival rates were 21.3% (95% CI 13.9 to 28.7) and 3.5% (0 to 8.5), respectively. There was no significant change in survival between sequential cohorts of patients over the 10 year period (data not shown).
Univariate analysis of the 142 cases is presented in table 1. Poor clinical prognostic factors that were statistically significant were male sex, old age, weight loss of >5%, presence of pleuritic chest pain, and ECOG performance status of >0. A history of exposure to asbestos was given in 81% of patients but was not a poor prognostic factor. Low haemoglobin, high white blood cell count, and thrombocytosis were significantly associated with poor prognosis. Epithelial cell type had a better prognosis than mixed cellularity and sarcomatoid types (p<0.0001). The degree of certainty of histological diagnosis was not associated with survival. The hazard ratios for performance status >0 and for non-epithelial cell type, the variables for which the differences in survival were greatest, were 3.33 and 2.7, respectively. Biopsy alone was performed in 47 patients, whereas surgical resection of tumour was carried out in 72 patients (parietal pleurectomy in 22, visceral decortication in 42, and extrapleural pneumonectomy in eight patients). It was not possible to determine the exact surgical procedure in 23 patients. Although there was a trend towards longer survival in patients who underwent surgical resection, this did not reach statistical significance (p = 0.09).
Prognostic factors for malignant mesothelioma (MM) analysed in a univariate Cox proportional hazards model (n = 142)
Five variables emerged as statistically significant from the multivariate Cox model (table 2). In order of decreasing significance these were histological cell type, haemoglobin, white blood cell count, performance status, and sex. Non-epithelial cell type was associated with a hazard ratio of 2.33 (95% CI 1.46 to 3.72). For each rise in haemoglobin of 1 g/dl there was a fall in risk of 21%, whereas each rise in white blood cell count of 1 × 109/l increased the risk by 11%. An ECOG performance status of 1 or 2 was associated with a hazard ratio of 2.01 (95% CI 1.24 to 3.28) in the multivariate model.
Analysis of prognostic variables in a forward, stepwise multivariate Cox proportional hazards model. Only cases with complete data for all prognostic variables were included in this model (n = 101)
There was a significantly greater proportion of patients in the EORTC high risk group in the Leicester series than in the EORTC series (60% versus 42%, p = 0.002, χ2 test). However, χ2 for trend analysis revealed that there was not a statistically significant shift towards the high CALGB groups in our series (p = 0.27).
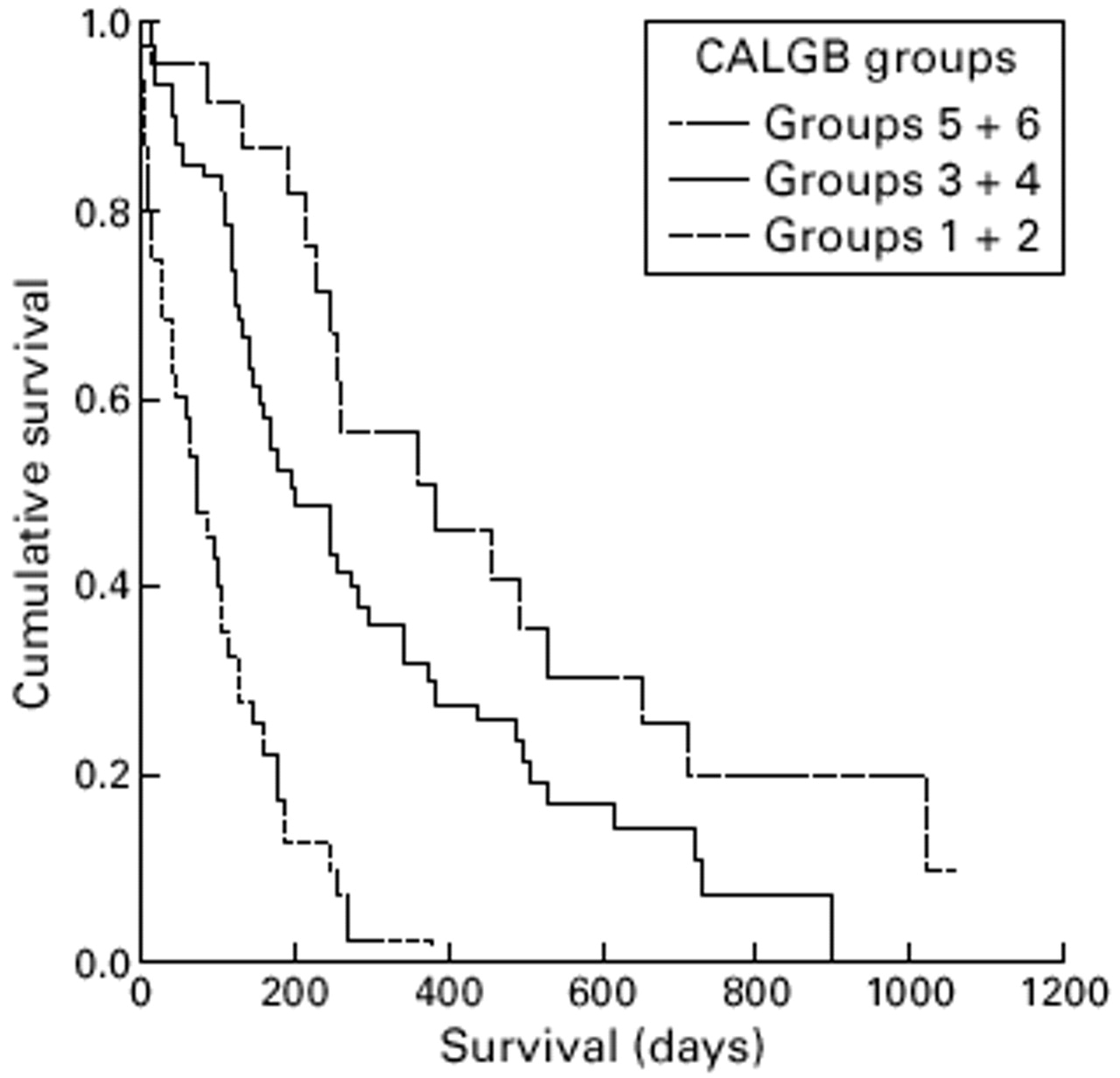
EORTC risk groups were correctly correlated with survival in this series of patients (fig 1). The same was broadly true for the CALGB groups, but there were only two, five and nine cases in groups 2, 4 and 6, respectively. When groups 1 and 2, 3 and 4, and 5 and 6 were combined, good stratification in the Kaplan-Meier plot was achieved (fig 2). Median survival rates were generally comparable to the EORTC series (table 3), with the EORTC data within the 95% CI of our series for the low risk group and just outside for the high risk group. The one and two year survival rates were equivalent in Leicester and the EORTC series in both high and low risk groups. Similarly, median, one, and two year survival of our series, when grouped according to the CALGB criteria, were comparable to the published series (table 4).

Kaplan-Meier survival plot showing the difference in survival between patients within EORTC high and low risk groups (p = 0.0001, Cox's proportional hazards).
{kind=link}
{kind=link}
Kaplan-Meier survival plot showing the difference in survival between patients within CALGB prognostic groups (p <0.0001, Cox's proportional hazards). Groups have been combined because of the small numbers in the even numbered groups.
Survival of patients in the Leicester series compared with the EORTC series when classified by prognostic group
Survival of patients in the Leicester series compared with the CALGB series when classified by prognostic group
Discussion
The poor prognostic factors identified in univariate analysis are consistent with those of other studies. Specifically, we confirm that male sex, older age, weight loss, chest pain, poor ECOG performance status, abnormal haematological indices, and non-epithelial cell type are poor prognostic factors. Similarly, stepwise multivariate analysis yielded as significant prognostic factors cell type, haemoglobin, white cell count, performance status and sex. These results are similar to other studies in which multivariate models have been used (table 5). Clinical features such as the presence of pleuritic chest pain or weight loss and haematological indices have been examined in fewer studies than cell type and performance status. However, these variables were incorporated into the EORTC and CALGB prognostic systems.
Review of previous multivariate analyses of prognostic factors in malignant mesothelioma and comparison with this series
One of the initial aims of this study was to evaluate the IMIG stage in our patients. Despite reviewing operation notes and computed tomographic (CT) scans, it was felt that retrospective TNM staging would not be sufficiently accurate. We therefore rejected the possibility of assessing stage-specific survival in this series. We decided to analyse survival according to EORTC and CALGB prognostic criteria. Figures 1 and 2 show the success of both systems in stratifying survival. There were relatively few patients in the even numbered CALGB groups and so groups were combined to aid clarity.
Analysis of the results revealed that the median survival time and one and two year survival rates for the Leicester patients, when grouped appropriately into the EORTC and CALGB groups, were comparable. Therefore, whereas this study confirms that overall survival from malignant mesothelioma in the UK is poor in comparison with other European series, this is not the case when analysis by prognostic groups is performed. This may also be of relevance in other solid tumours when survival in the UK is compared with other countries.
Recent work has identified angiogenesis and other biological markers to be of prognostic value in malignant mesothelioma.27-29The value of new molecular markers should be analysed with respect to existing factors in order to assess their prognostic relevance.
In conclusion, this study is the first independent series to validate the effectiveness of the EORTC and CALGB systems. Survival in our series is no worse than in the two chemotherapy based series in which patients are stratified into prognostic groups. In view of the difficulty of accurate TNM staging, assessment of these prognostic groups should be incorporated into the planning of future clinical trials, including the proposed BTS/MRC trial of chemotherapy and radiotherapy.
Acknowledgments
We acknowledge the Institute of Cancer Studies and the Glenfield Hospital NHS Trust, Leicester, UK for their support.