Article Text

Abstract
A 41 year old woman presented with community acquired pneumonia (CAP) which failed to resolve following treatment with amoxycillin and cefaclor prior to referral. Quantitative culture of sputum revealed a pure growth of Haemophilus parainfluenzae and, following antibiotic susceptibility testing of the isolate, ciprofloxacin was prescribed resulting in resolution of the infection. Immunological investigations showed that the patient had a high titre of H parainfluenzae specific IgM. The combination of a pure growth of H parainfluenzae, a response to appropriate antimicrobial therapy, and the presence of a specific antibody response indicated that this organism had a pathogenic role in the patient's pneumonia and should be considered in the differential diagnosis of CAP.
- Haemophilus parainfluenzae
- pneumonia
Statistics from Altmetric.com
Respiratory tract infections remain a common cause of morbidity and mortality worldwide and pneumonia in particular is the leading cause of death due to infectious diseases in developed countries. The microbiological aetiology of community acquired pneumonia (CAP) has changed over the last 20–30 years and, althoughStreptococcus pneumoniae is still the most prevalent pathogen, recent studies indicate an increasing incidence of pathogens such as Legionella spp,Mycoplasma spp,Chlamydia pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, and viruses.1 In as many as 33% of cases, however, the microbial aetiology of the disease remains unidentified.2 Haemophilus parainfluenzae has been implicated in pneumonia but its role remains uncertain in view of its assumed low pathogenicity.3 We report details of a patient with pneumonia in whom an immune response was demonstrated to an isolate of H parainfluenzae recovered as a pure growth from her sputum. The evidence indicates that this was the causative organism.
Case report
A 41 year old woman presented to her GP with a 10 day history of pyrexia, cough with purulent sputum, and general malaise. Past medical history was unremarkable, she had given up smoking eight years ago, and only consumed alcohol occasionally. She was treated with amoxycillin 500 mg three times a day for five days with no effect. Two days before her referral to the respiratory department in secondary care she developed some chest discomfort and was started on a slow release preparation of cefaclor.
When seen she looked reasonably well and clinical examination was normal apart from some fine middle lobe crackles. Her full blood count and biochemical profile were normal but the erythrocyte sedimentation rate (ESR) and C reactive protein level were raised (105 mm/h and 102 mg/l, respectively). The chest radiograph showed consolidation of the middle lobe and, in view of these findings, she was commenced on clarithromycin 500 mg twice a day and sputum was collected for culture.
Quantitative sputum culture4 revealed a pure growth ofH parainfluenzae at a concentration of 2.2 × 108 colony forming units/ml. No evidence ofStreptococcus pneumoniae colonies was seen using this sensitive technique which involves the culture of serial dilutions of the homogenised sputum sample on blood and chocolate agar for 48 hours. The H parainfluenzae isolate was fully susceptible to amoxycillin, augmentin, trimethoprim, cefuroxime, and ciprofloxacin, but resistant to erythromycin and clarithromycin. Treatment was therefore changed to ciprofloxacin 750 mg twice daily. One week later she was much improved, producing only small amounts of clear sputum from which no recognised respiratory pathogens were recovered. Repeat ESR was 96 mm/h but the C reactive protein level had fallen to 6 mg/l. Two weeks later antibiotic treatment was stopped when ESR and C reactive protein had fallen to 37 mm/h and 1 mg/l, respectively.
A serum sample obtained before starting treatment with ciprofloxacin was tested for the presence of IgG, IgA and IgM antibodies toH parainfluenzae by an ELISA in which the capture antigen was prepared “in house” according to the method of Suzuki et al.5 In brief, the capture antigen consisted of eight distinct isolates ofH parainfluenzae (distinguished by differences in outer membrane protein profiles on SDS-PAGE) that were grown overnight in broth, harvested by centrifugation, and washed by resuspension in phosphate buffered saline (PBS, pH 7.4) followed by centrifugation as before. Isolates were resuspended in PBS, combined, sonicated (Soniprobe, Lucas Dawe Ultrasonics, UK), and centrifuged as before to remove whole cells. Total protein content was measured using a modified Lowry method and the sonicate was stored frozen in aliquots. Serum H parainfluenzae specific IgG and IgA levels were 0.41 and 0.40 absorbance units respectively, which were within the ranges measured in nine healthy control subjects (IgG mean (SD) absorbance units 0.26 (0.15), range 0.12–0.58; IgA mean (SD) absorbance units 0.15 (0.11), range 0.02–0.35). The IgM titre of 0.65, however, was raised compared with the range in healthy controls (mean (SD) 0.08 (0.07), range 0–0.24).
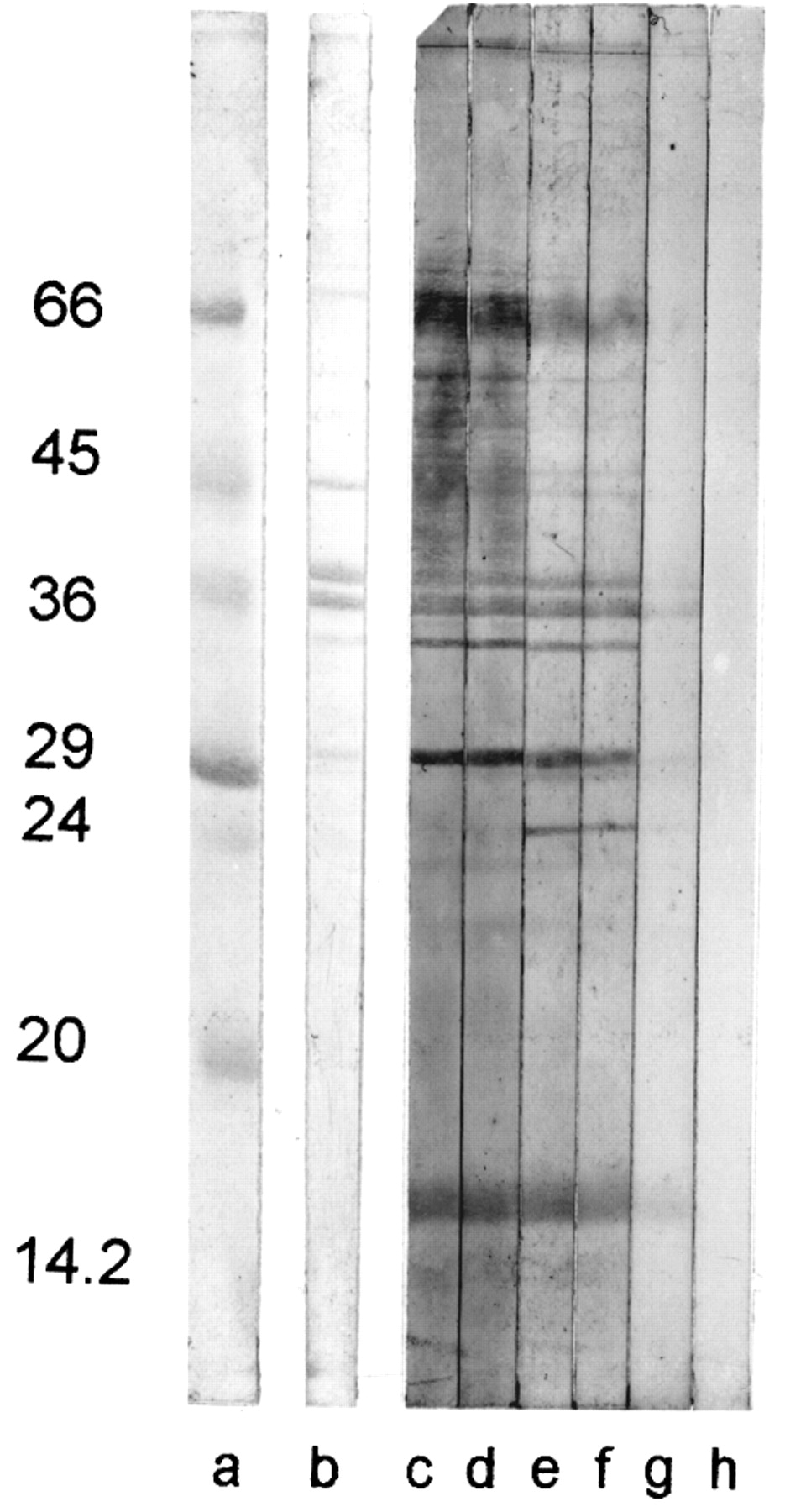
A western blot assay was used to confirm that outer membrane proteins prepared according to the method of Murphy and Apicella6from the isolate of H parainfluenzaerecovered from the subject were recognised by specific IgM in the patient's serum up to a dilution of 1/500 (fig 1). Serological testing by complement fixation revealed no other evidence of infection byM pneumoniae,Chlamydia spp, Coxiella burnetii, influenza virus A or B, respiratory syncytial virus, or adenovirus.

{kind=link}
Outer membrane proteins of H parainfluenzae isolated from the sputum of a patient with pneumonia. Proteins were separated on a 12.5% SDS-PAGE gel, transferred to nitrocellulose, and immunoassayed for the presence of specific IgM in serum from the patient. Lane a = low molecular weight markers; lane b = total protein stain; lanes c–g = serum diluted 1/5, 1/10, 1/50, 1/100 and 1/500, respectively; lane h = no serum control.
Discussion
Traditionally, H parainfluenzae has not been regarded as a respiratory tract pathogen. It has previously been identified in pneumonia7 ,8 but it remains unclear whether it was a contaminant or the actual pathogen involved. There have, to our knowledge, been no serological studies which clarify the role of this organism in lung infection. In the case we present there was a pure growth in high numbers of H parainfluenzae from the sputum (>108 cfu/ml), a specific IgM antibody response to H parainfluenzaeantigens, and a clinical response. The failure to respond to the initial course of amoxycillin prescribed by the GP may reflect the inadequate length of treatment (five days) in a patient with an invasive infection. Given the therapeutic failure of amoxycillin in this case, and the data showing that H parainfluenzae isolates often display reduced susceptibility to amoxycillin,9 ,10 the use of a quinolone may be an appropriate second line of treatment in pneumonias from whichH parainfluenzae has been isolated.
It is possible that H parainfluenzae could have been a secondary pathogen following the initial pneumonia due to another aetiological agent; however, by the time the patient was referred to secondary care, only H parainfluenzae was recovered despite extensive quantitative culture in a research laboratory specialising in respiratory infection. There was no evidence, based on serological testing, of either a viral or atypical aetiological agent. Nevertheless, whatever the sequence of events, the immune response in this patient indicates thatH parainfluenzae had played a pathogenic role in the illness.
This case suggests that H parainfluenzae can cause pneumonia with systemic features in the community, even in apparently immunocompetent individuals. It should be considered as a possible pathogen, especially when conventional first line treatment fails.