Article Text

Abstract
BACKGROUND An inverse association between tuberculin responses and atopy has been observed in Japanese children, indicating that BCG immunisation, subclinical exposure to Mycobacterium tuberculosis without clinical disease, or host characteristics may influence the T helper (Th) lymphocyte balance with decreased atopy as a result. This study was undertaken to determine whether tuberculin reactivity is inversely related to atopy in young adults vaccinated with BCG at the age of 14.
METHODS Men and women aged 20–44 years were tested using the adrenaline-Pirquet test with Norwegian produced synthetic medium tuberculin (n = 891). In addition, their serum total and specific IgE antibodies against mite, cat, timothy grass, mould and birch were measured.
RESULTS Of the 574 subjects with complete examinations, 64% had a positive adrenaline-Pirquet tuberculin test (⩾4 mm) and 27% exhibited IgE antibodies (⩾0.35 kU/l) to one or more of the five specific allergens. The geometric mean of total serum IgE in the population was 30.2 kU/l. Tuberculin reactivity and log IgE were not correlated (r = 0.043, p = 0.30). The mean tuberculin reactivity was 4.6 mm, 4.9 mm, and 5.0 mm in the lower, middle and upper tertile of IgE distribution (<14 kU/l, 14–61 kU/l, >61 kU/l). The prevalence of atopy, as assessed by either the presence of any of the five specific IgE antibodies or by each specific IgE antibody separately, did not differ between subjects with a positive and those with a negative tuberculin test. These results persisted after adjustment for age, sex, and smoking status in multivariate logistic regression analyses.
CONCLUSIONS In this young adult population, BCG vaccinated at the age of 14, no significant relationship between a positive tuberculin reaction and atopy was observed. If a true relationship had been found, our study suggests that it may be limited to populations immunised in early childhood when a substantial modulation of the immune system can occur.
- atopy
- asthma
- tuberculosis
- immunisation
- BCG vaccination
Statistics from Altmetric.com
T helper (Th) lymphocytes have a central regulatory role in allergic inflammation and can be subdivided according to their production of cytokines.1 When stimulated by some respiratory infections or immunisation with attenuated bovineMycobacterium tuberculosis vaccine (BCG), Th1 can secrete interferon (IFN)-γ and interleukin (IL)-2 which can inhibit B lymphocyte production of IgE.2 By contrast, Th2 cells, when stimulated by allergens such as house dust mite, grass and pollen, release IL-4 which promotes IgE production by the B lymphocytes. Th2 responses dominate in atopic individuals and may infer subsequent expression of disease including asthma.3Furthermore, the absence of infections in childhood might, according to the microbial stimulation hypothesis, release Th2 immune mechanisms and thus promote allergic asthma.4
Shirakawa et al reported an inverse association between tuberculin responses and atopic disorders in Japanese children5 which suggested that BCG immunisation or subclinical exposure to M tuberculosisfrom birth up to the age of 12 years may influence the Th lymphocyte balance with decreased atopy as a result. An alternative explanation is that host characteristics such as the genetically determined balance of Th1 and Th2 responsiveness may generate a non-causal inverse relationship between tuberculin response (Th1) and atopy (Th2). Swedish investigators, however, have not observed a significant relationship between BCG vaccination during the first year of life and development of atopy in children, assessed either by a questionnaire6or by skin prick tests and measurement of serum specific IgE antibodies.7 Although the evidence for an association between BCG vaccination and atopy is inconsistent, one could question whether such a relationship may be extended to immunisation in adolescence or whether it is limited to vaccinations given early in infancy. The plasticity of the immune system and the gains of immune deviation may at that time be greater than later in life.8We have used tuberculin reactivity as an indicator of the effect of the previous BCG vaccination, which is the only one except assessing the presence of a scar. Previous observation in our area showed that about 80% of the subjects were positive tuberculin reactors three months after BCG vaccination, while the figures were reduced to 70% and 60%, respectively, one and 10 years after BCG vaccination.9 In Norway mandatory BCG vaccination is given at the age of 14 and therefore all children are exposed to mycobacterial antigen at this time. We investigated whether a stronger tuberculin reactivity during adult life was related to lower levels of total and specific serum IgE when examined cross sectionally in young adults. A lack of association would argue against the “host characteristic” interpretation of the Japanese findings.
Methods
STUDY POPULATION
A random sample of 1200 men and women aged 20–44 years living in Bergen, Norway was invited to participate in the Norwegian part of the European Community Respiratory Health Survey,10 and 903 subjects (75.3%) attended the study from September 1992 to June 1993. Twelve subjects were excluded from skin testing due to eczema. Of the 891 subjects who underwent tuberculin and allergy testing, including measurements of serum total and specific IgE antibodies, 574 (64%) returned after 2–7 days (42–171 hours) to have their tuberculin reactions read. Of these, nine were tuberculin converters and had never received BCG vaccination, seven had no information on their BCG status, while 558 subjects had been vaccinated with BCG at the age of 14.
TUBERCULIN AND ALLERGY TESTING
Each subject was tested using the Norwegian reference method of adrenaline-Pirquet in duplicate on the volar side of the forearm. The adrenaline-Pirquet test is a modification of von Pirquet's skin scarification method11 that uses Norwegian produced synthetic tuberculin (SMT 14) and adrenaline.12 ,13 The repeatability of the test is comparable to that observed for the Mantoux test.14 The adrenaline-Pirquet reactions are recommended to be read at 48–72 hours, but the test appeared to be independent of time of reading within four days.14 The adrenaline-Pirquet tuberculin reaction should be read as the highest value at 90° to the scratch line and a diameter of ⩾4 mm is taken as a positive result.15 The larger of the duplicate adrenaline-Pirquet reactions is used for screening16 as well as for the analyses in the present study. Every subject was offered a miniature chest radiograph and no subjects had findings indicating active or inactive tuberculous disease.
For measurements of serum IgE, 10 ml of venous blood was taken from each subject, coagulated at room temperature, centrifuged, stored at –20°C, packed, and sent on dry ice to Pharmacia Diagnostics AB (Uppsala, Sweden). Serum specific and total IgE levels were measured using the Pharmacia CAP system.17 The working range for the total IgE assay was 2–2000 kU/l. All subjects had detectable IgE, and one subject had a value of more than 2000 kU/l (assigned as 2050 kU/l). All assays for specific IgE were judged to be positive if they had more than 0.35 kU/l of the specific allergen. Specific IgE levels were measured against house dust mite (Dermatophagoides pteronyssinus), timothy grass, cat, mould (Cladosporium herbarum), and a local allergen (birch). Tuberculin and allergy testing as well as the reading of all skin tests was performed by the same experienced public health nurse who was blinded to the serological outcome of serum IgE results at the time of the tuberculin reading.
ENVIRONMENTAL EXPOSURES
Participants were categorised as non-smokers, ex-smokers, or smokers according to the ECRHS questionnaire.10 Smokers were those who had smoked at least one cigarette a day or one cigar a week for as much as one year or who had smoked at least 400 cigarettes or 360 g tobacco during their lifetime; ex-smokers were those who had stopped smoking more than one month previously; and non-smokers had never smoked, using the above definitions. Occupational exposure was assessed by asking: “Have you ever worked in a job which exposed you to vapours, gas, dust or fumes?” The answers were given as yes (n = 261) or no (n = 313).
DATA MANAGEMENT AND ANALYSIS
Serum total IgE values were log transformed in order to obtain a Gaussian distribution. To investigate bivariate relationships between tuberculin positivity and specific IgE antibodies we used a corrected χ2 test. The power was generally too low (55%) to detect an odds ratio of 1.5 but was adequate (96%) for an odds ratio of 2.0 when using the any of the five specific IgE antibodies as variables. For the individual allergens the power was somewhat lower. Standard methods for contingency tables such as χ2 tests and logistic regression analysis were used to compare proportions. One way analysis of variance and general linear models were used to compare continuous outcomes. In the multivariate analyses we used the variable “any of the five specific antibodies” rather than the individual specific IgE antibodies variable to obtain more statistical power.
When examining positive predictors for the presence of a positive tuberculin reaction, a multiple logistic regression model was applied including sex, age, smoking status, occupational exposure to dust or gas, level of total IgE antibodies, any of the five specific IgE antibodies, and first order interactions between these variables. Interactions were checked for statistical significance in a backward stepwise manner. From previous knowledge it was decided to include sex, smoking status, and occupational exposure in the model regardless of their statistical significance in the final analysis. All the statistical analyses were performed with the BMDP package.18
Results
PARTICIPATION RATES AND STUDY POPULATION
The characteristics of the study population are presented in table1. Subjects invited to the clinical examination who did not attend even after two reminders were defined as non-attenders. Non-attenders were slightly younger than attenders and were more often men. Of those with complete examinations, 95% had been BCG vaccinated while 2% were tuberculin converters when examined before the scheduled BCG vaccination at the age of 14. All subsequent analyses were restricted to the 574 participants for whom complete tuberculin reactivity and IgE data were available.
Characteristics of the study population by response status in 20–44 year old Norwegian men and women1-150 (n = 1200)
DISTRIBUTION OF TUBERCULIN REACTIVITY
The distribution of tuberculin reactivity in these young adults is shown in fig 1. A positive test, defined as a reaction of ⩾4 mm diameter, was obtained in 357 subjects (64%). The mean (SD) tuberculin reaction for all subjects was 4.8 (3.0) mm. A significant increase in tuberculin reactivity was observed with increasing age (regression coefficient 0.037, p<0.01), ranging from 3.1 mm in those aged 20–24 years to 4.9 mm in those aged 40–44 years. Tuberculin reactivity was also higher in men than in women (5.2 versus 4.4 mm, p<0.01) and in smokers than in non-smokers (5.1 versus 4.3 mm, p<0.01).

{kind=link}
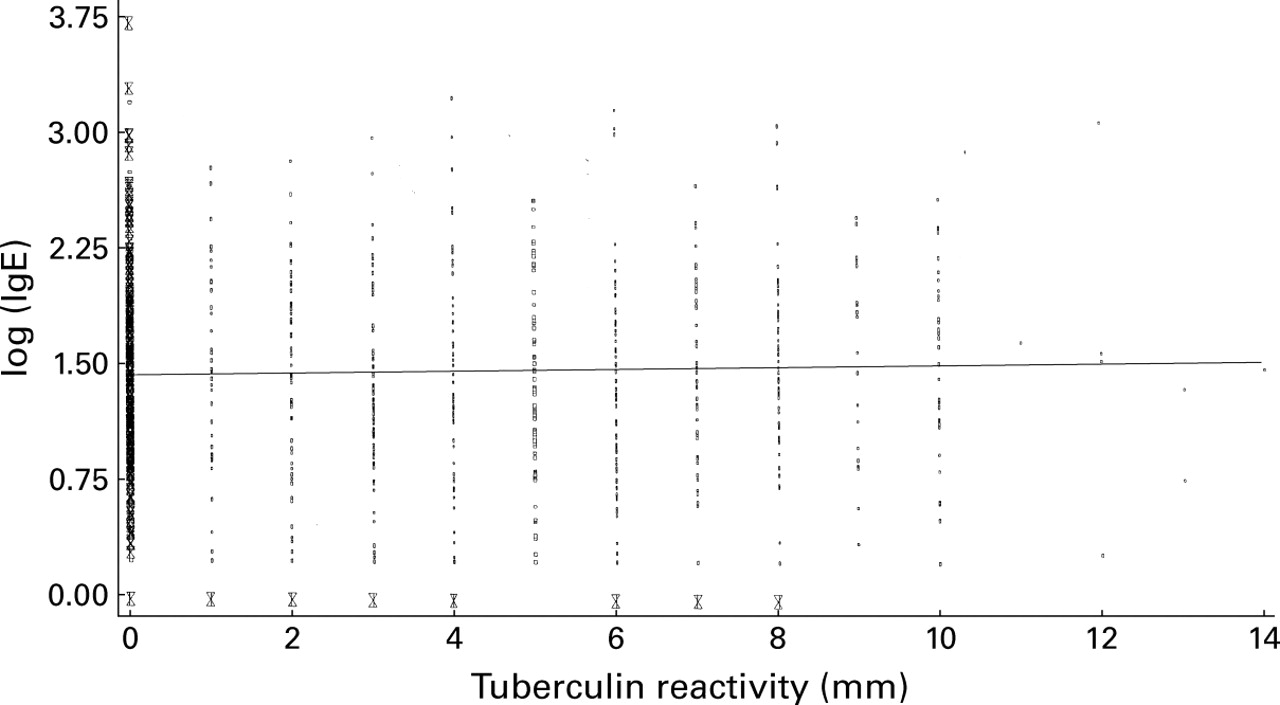
Tuberculin reactivity by total serum IgE in young Norwegian adults (n = 574).
DISTRIBUTION OF IGE
The geometric mean total serum IgE concentration was 30.2 kU/l with higher levels in smokers than in non-smokers (35.7 versus 27.1 kU/l, p<0.01) but no significant variation with age or sex. One or more of the five specific IgE antibodies was observed in 27% of those examined (house dust mite 14%, cat 8%, timothy grass 16%, birch 10%, and moulds 2%). The probability of having a positive response to any of the five allergens or having each of the specific IgE antibodies separately did not vary significantly (p<0.05) with sex or smoking category. The prevalence of one or more of the specific IgE antibodies decreased significantly with increasing age (p<0.01), ranging from 31% in those aged 20–24 years to 18% in those aged 40–44 years.
UNIVARIATE RELATIONSHIP BETWEEN TUBERCULIN REACTIVITY AND IGE
Tuberculin reactivity and log IgE values were uncorrelated in this young population (r = 0.043, p = 0.30; fig1). The mean tuberculin reactivity in the lower, middle, and upper tertile of IgE distribution (<14 kU/l, 14–61 kU/l, >61 kU/l) was 4.6 mm, 4.9 mm, and 5.0 mm, respectively. Although not significantly different (p = 0.19 in test for equality of slopes), increasing tuberculin reactivity in non-smokers tended to be associated with slightly decreasing log IgE levels while in smokers and ex-smokers the association was reversed.
The prevalence of a positive IgE response to any of the five specific IgE allergens did not differ between subjects with a positive and a negative tuberculin test (table 2). Furthermore, no significant differences with age, sex, or smoking habit were observed in having any of the five specific IgE antibodies (p<0.05). The pattern appeared to be similar for the individual specific allergens.
Distribution of specific IgE antibodies (>0.35 kU/l) by tuberculin reactivity status assessed with the adrenaline-Pirquet method in young Norwegian adults
MULTIVARIATE RELATIONSHIP BETWEEN TUBERCULIN REACTIVITY AND IGE
In the multiple logistic regression analyses none of the interactions was statistically significant. The odds ratio for positive tuberculin reactivity was not related to the level of total serum IgE antibodies nor to the presence of any of the five specific IgE antibodies measured (table 3). However, the odds ratio for being tuberculin reactive was significantly higher in men than in women, in older than in younger subjects, and in smokers than in non-smokers (table 3). An analysis of the variables shown in table 3 stratified by smoking status showed an effect of the same magnitude across smoking categories.
Adjusted odds ratios (OR) and 95% confidence intervals (CI) for having a positive adrenaline-Pirquet tuberculin test (⩾4 mm) in young Norwegian adults based on multiple logistic regression analysis
Discussion
We found that a positive tuberculin test was significantly related to age and smoking habits but not to markers of atopy (total and specific IgE antibodies) in this young adult population from Bergen, Norway, most of whom had received BCG vaccination at the age of 14 years. These results were consistent in both the univariate and multivariate analyses.
The study population, drawn randomly from the general population, consisted of young men and women living in Bergen, Norway. The participation rate in the study was 75%. However, less than 50% of those invited returned to have their tuberculin reactivity test read after 2–3 days. As with other population studies performed in the same area,19 those who returned were somewhat older and included a lower proportion of men. The main purpose of this study was the assessment of respiratory health in general,10 and the selection was not on the basis of BCG vaccination, tuberculin status, or disease. We therefore believe that the exclusion of attenders who were allergy and tuberculin tested but not read should not have biased our results to a substantial degree. The difference in the mean age of those who did and did not return to have their tests read was only one year and the percentage of tuberculin converters prior to BCG vaccination was at the same level.
BCG immunisation status was assessed using the adrenaline-Pirquet test with synthetic medium tuberculin. This test has recently been shown to be comparable with the Mantoux test in terms of reproducibility14 and the proportion of tuberculin reactors in a population.20
Until 1995 BCG vaccination was mandatory in Norway at the age of 14 years, except for those who had a positive synthetic medium tuberculin test or in whom the test was contraindicated. The study population was born between 1947 and 1971 when the BCG coverage in this population was approximately 95%. The incidence of tuberculous disease in the community in this age group has been less than one per 100 000.21 Consistent with this, we did not observe any subjects in the study population with tuberculous disease.
Our markers of atopy (serum total and specific IgE levels) are widely used and well recognised markers and have been applied in large epidemiological studies. The total serum IgE levels, as well as specific IgE levels, were lower than those observed in the UK, North America, Australia and New Zealand.17 A significant relationship between total IgE and specific IgE as markers of atopy has been observed in a previous population study from Norway,19 indicating that these IgE measurements are highly related to atopy in this northern environment. In other areas of the world IgE reactivity may be driven by other environmental exposures, as indicated by the ECRHS survey where no relationship between total and specific IgE was observed.17 We therefore believe that total and specific serum IgE measurements are useful markers of atopy in the present study.
Shirakawa et al 5 observed an inverse association in Japanese children between tuberculin responses and atopic disorders, indicating that immunisation, subclinical exposure to M tuberculosis, or host characteristics from birth to the age of 12 years may influence the Th lymphocyte balance with decreased atopy in children as a result. In the same study subjects converting to a positive tuberculin test at the age of 12 appeared to have less atopy and symptomatic asthma than those converting at the age of six. This might suggest that immunisation may have a role in modulation of the immune system in older children as well. Furthermore, in a retrospective analysis, immunisation with whole cell pertussis vaccine was found to be a predictor of allergic asthma, hay fever, and eczema.22 However, other investigators have not observed a significant relationship between BCG vaccination and development of atopy in children,6 ,7 One might therefore speculate whether BCG vaccination, primary tuberculosis infection early in childhood, or sensitisation to environmental mycobacteria was responsible for tuberculin responsiveness in the Japanese study. Approximately 1–2% of Norwegian school children have a positive tuberculin reaction before the scheduled BCG vaccination at the age of 14, mostly as a result of infection with environmental mycobacteria.21 Later in life a positive tuberculin reaction may be observed as a result of exposure and infection by environmental mycobacteria. However, it is unlikely that these numbers would be so high in young healthy Norwegian adults that it would affect our observations. In general, differences in host characteristics, indoor and outdoor environmental exposures, family size, and immunisation programmes/assessment may be of importance when explaining differences between Scandinavian and other studies.
Since BCG vaccination of the population is performed in only a few countries, this Norwegian population with its high coverage of BCG vaccination could be used to assess the relationship between tuberculin reactivity and atopy using well recognised markers of atopy. We did not observe significant relationships between a positive tuberculin test and markers of atopy in young men and women when immunisation was performed at the age of 14. This might suggest that host characteristics such as the Th1/Th2 balance do not explain the relationship between tuberculin reactivity and atopy observed in the younger Japanese population.5 If a true relationship exists between tuberculin reactivity and atopy, our study suggests that this relationship may be limited to populations immunised in early childhood when a substantial modulation of the immune system can occur.
Acknowledgments
The authors acknowledge public health nurse Mrs Berit Drageset who performed the tuberculin testing and reading and nurse Mrs Bjørg Meidell who did the interviews and data registration. The authors are grateful for their accuracy and persistence. We also thank Geir Egil Eide for statistical advice. The study was supported by the Norwegian Research Fund for Asthma and Allergy and the Norwegian Research Council.