Article Text

Abstract
BACKGROUND Little is known about pulmonary Mycobacterium aviumcomplex (MAC) infection in human T lymphotrophic virus type I (HTLV-I) carriers. A study was undertaken to investigate and clarify the characteristics of pulmonary MAC infection in these subjects.
METHODS Twenty nine patients with pulmonary MAC infection without any underlying pulmonary disorder were investigated. The clinical features and radiographic appearance of HTLV-I carriers and non-carriers were compared and the bronchoalveolar lavage (BAL) fluid of these 29 patients and eight normal female control subjects was analysed.
RESULTS The prevalence of the HTLV-I carrier state in patients with pulmonary MAC infection was 34.5% (10/29) compared with 16.7% (529/3169) among all patients admitted to our department between 1994 and 1998 (odds ratio (OR) 2.63, 95% confidence interval (CI) 1.21 to 5.68). The HTLV-I carriers were all women and all had clinical symptoms, but they did not show systemic dissemination. Peripheral multifocal bronchiectasis with nodular shadowing was seen frequently on the chest computed tomographic (CT) scans of HTLV-I carriers. The area of the pulmonary lesions was more extensive than in non-carriers (p<0.05). White blood cell (WBC) counts and C reactive protein (CRP) levels on admission were significantly lower in HTLV-I carriers than in non-carriers (WBC: difference (D) = 1565/μl, 95% CI –68.9 to 3198.4/μl; CRP: D = 1.8 mg/dl, 95% CI –0.35 to 3.89 mg/dl). The concentrations of neutrophil elastase (NE) and interleukin (IL)-8 in BAL fluid were significantly higher in HTLV-I carriers than in non-carriers (NE: D = 1342 μg/l, 95% CI 704 to 1980.3 μg/l; IL-8: D = 304.5 pg/ml, 95% CI 89.7 to 519.4 pg/ml).
CONCLUSIONS Pulmonary MAC infection causes more diffuse and widespread lesions in HTLV-I carriers than in non-carriers.
- Mycobacterium aviumcomplex
- human T lymphotrophic virus type (HTLV)-I
- computed tomography
- cytokines
Statistics from Altmetric.com
Mycobacterium avium complex (MAC) is a common cause of disseminated infection in patients with acquired immunodeficiency syndrome (AIDS), and some studies have reported the clinical features of MAC infection in AIDS1 ,2 and other immunodeficient states such as cystic fibrosis.3 However, little is known about pulmonary MAC infection in patients infected with human T lymphotrophic virus type I (HTLV-I), a human retrovirus known to be the cause of adult T cell leukaemia (ATL)4 and HTLV-I associated myelopathy (HAM).5 It has been reported that T lymphocyte alveolitis frequently occurs in HAM.6Matsuzaki et al 7 reported a tendency for past respiratory illness in HTLV-I carriers. In this study we have investigated pulmonary MAC infection in HTLV-I carriers without any underlying pulmonary disorder, and have compared the features of this condition with those of pulmonary MAC infection in non-carriers.
Methods
SUBJECTS
Patients admitted to the Department of Respiratory Medicine of National Minami-kyushu Hospital between 1994 and 1998 were investigated by respiratory medicine specialists for inclusion in the study. Those with underlying factors of a systemic nature such as alcoholism, or of a local nature such as residual pulmonary damage from a previous infection, which predispose to pulmonary MAC infection, were excluded from the study, as were those who had unexplained pulmonary diseases and other possible pathogens. Patients who had reported cell mediated immune defects associated with MAC1-3 were also excluded.
All patients were examined for the presence of pulmonary MAC infection. The diagnosis of MAC infection was made initially by a DNA probe method (Gen-Probe Rapid Diagnostic System, Gen-Probe Inc, San Diego, USA)8 and confirmed by results of sputum or bronchial washing fluid culture on Ogawa egg medium on at least two separate occasions. We confirmed that all patients with pulmonary MAC infection had no underlying respiratory disorders before admission by screening the past histories and past chest radiographs.
DETERMINATION OF SERUM HTLV-I ANTIBODY
Serum samples were collected from all subjects and tested for anti-HTLV-I antibody as follows. Anti-HTLV-I antibody was measured with an Eitest-ATL kit (Eisai Inc, Tokyo, Japan) and serum samples with an enzyme-linked immunosorbent assay absorption rate of 0.5 or more were re-examined by the western blot method9 using MT-2 cell lysate antigens10 to confirm positivity.
CLINICAL STUDY
The clinical symptoms and laboratory findings (white blood cell (WBC) counts and C reactive protein (CRP) levels) of HTLV-I carriers and non-carriers were measured on admission.
CHEST COMPUTED TOMOGRAPHIC (CT) SCANS
The appearances on the chest CT scans were classified into five groups (nodules, mass, consolidation, bronchiectasis with nodules, and cavity) according to the classification of Primacket al.11 The affected pulmonary segments on the chest CT scans were examined to evaluate the distribution of pulmonary MAC infection. The ratio of affected area was judged subjectively by the visual scoring method.12 Each slice was evaluated individually and the right and left lungs were graded separately according to the percentage area having abnormal shadows on the CT scan (table 1). All slices above the level of the diaphragm were assessed in each patient. For each subject a visual score, which is the total of scores for each slice as a percentage of the total possible maximum score, was calculated. Each subject was evaluated independently on two separate occasions by two observers (a pulmonologist and a radiologist) without knowledge of the clinical data.
Scoring system
BRONCHOALVEOLAR LAVAGE (BAL) FLUID ANALYSIS
Subcutaneous injections of atropine (0.5 mg) and pentazocine (0.5 mg) were given. After anaesthetising the oral pharynx and upper airway with 4% lidocaine, a bronchofibrescope (Olympus BF type p20, Olympus Co, Tokyo, Japan) was wedged into the right B4segment. Four 40 ml aliquots of sterile physiological saline were instilled at 37°C, then removed by gentle suction. The recovered fluid was immediately filtered through sterilised gauze and the lavage fluid was spun in a cytometer (KN-70, Kubota Ltd, Tokyo, Japan) at 44g for five minutes and stained with May-Giemsa stain to identify cell populations. Five hundred cells (excluding epithelial cells) per slide were identified to establish differential cell counts expressed as percentages. The lymphocyte subtypes were analysed by flow cytometry using CD4 and CD8 monoclonal antibodies (Becton Dickinson Co, Mountain View, California, USA). The cytokines in the BAL fluid were measured using the following enzyme linked immunosorbent assay (ELISA) kits: tumour necrosis factor (TNF)-α, interleukin (IL)-1β, IL-6 (R&D Systems Co, Minneapolis, Minnesota, USA), IL-8 (Toray Fuji Bionics, Tokyo, Japan), and neutrophil elastase (NE) (Merck Co, Darmstadt, Germany). The albumin concentration in BAL fluid was determined with an automated specific immunoturbidimetric assay. Correlations between the cell populations and cytokines in the BAL fluid were analysed statistically.
Eight normal volunteers, all of whom were women (mean (SD) age 67.2 (7.8) years) and non-smokers, were recruited as controls for the BAL fluid study. All volunteers gave written consent to participate in the study. None had had any previous pulmonary disorders or disease which might cause immunological abnormality—for example, collagen disease or AIDS—and their chest radiographs, chest CT scans, and pulmonary function tests were all normal.
STATISTICAL ANALYSIS
The χ2 test, Mann-Whitney test, one way factorial ANOVA with Bonferroni/Dunn test and Pearson's correlation coefficient were used to measure differences between the groups. A p value of <0.05 was considered significant. Most values were expressed as mean (SD). All data were presented with appropriate 95% confidence intervals.
Results
SUBJECTS
Twenty nine patients were diagnosed as having pulmonary MAC infection. Confirmation that MAC was responsible for the lung pathology came from the fact that the patients had no other pathogens which cause pulmonary disorder and all showed improvement of abnormal lung shadows and disappearance of MAC from the sputum after treatment of MAC. The percentage of HTLV-I carriers among the patients with pulmonary MAC was 34.5% (10/29), but they had never had adult T cell leukaemia (ATL) or HTLV-I-associated myelopathy (HAM). There was no significant difference in age between the HTLV-I carriers (mean (SD) 69.5 (10.1) years) and non-carriers (70 (9.1) years). A total of 3169 patients were admitted to the Department of Respiratory Medicine between 1994 and 1998;their mean (SD) age was 61.3 (19.8) years. Of these 3169 patients, 529 (16.7%) were HTLV-I carriers compared with a prevalence of HTLV-I carrier state among patients with pulmonary MAC infection of 34.5% (p<0.05, odds ratio (OR) 2.63, 95% CI 1.21 to 5.68).
CLINICAL STUDY
The HTLV-I carriers were all women while, among the non-carriers, there were three men and 16 women. There were no disorders that might cause immunological abnormalities (including collagen disease) among the HTLV-I carriers. Two of the non-carriers had diabetes mellitus and one had liver cirrhosis due to hepatitis C virus. There was no history of smoking among the HTLV-I carriers while the three male non-carriers had smoking histories. There were no patients with sinusitis in either group. All HTLV-I carriers had clinical symptoms while only 11 of the 19 non-carriers had clinical symptoms. The asymptomatic non-carriers were investigated because of their chest radiographic abnormalities. No patient in either group had evidence of systemic dissemination. The WBC counts and CRP levels on admission were significantly lower in the HTLV-I carriers than in the non-carriers (WBC: difference (D) = 1565/μl, 95% CI –68.9 to 3198.4/μl, p<0.05; CRP: D = 1.8 mg/dl, 95% CI –0.35 to 3.89 mg/dl, p<0.05). All the patients were treated with three-drug (e.g. clarithromycin, rifampin and ethambutol) or four-drug (e.g. isoniazid, rifampin, ethambutol and streptomycin) regimens. Three HTLV-I non-carriers received surgical treatment in addition to chemotherapy. Non-carriers needed treatment for 11.8 (4.2) months and HTLV-I carriers needed treatment for 13.8 (5.1) months to achieve disappearance of MAC from the sputum.
RADIOGRAPHIC PATTERNS
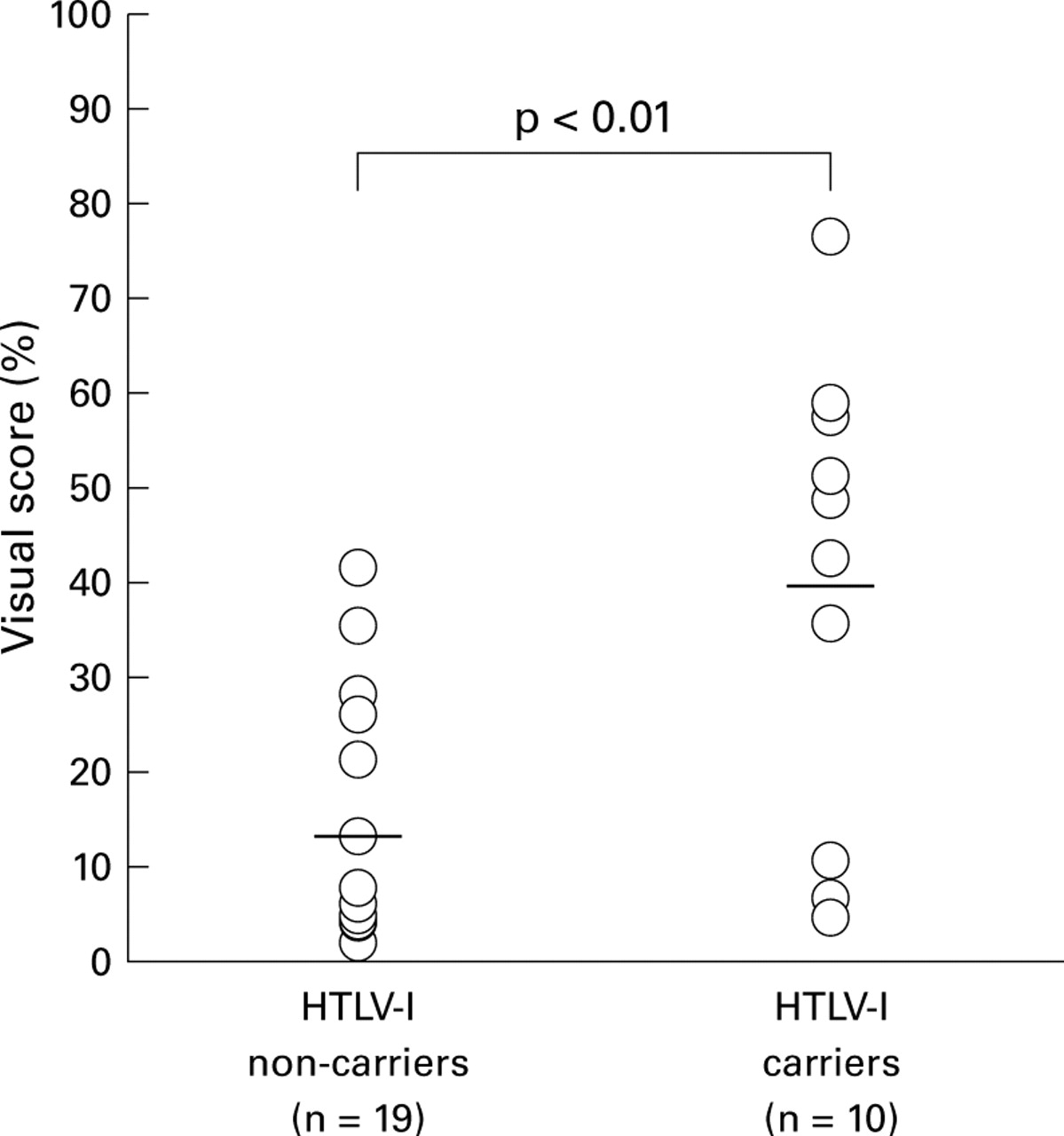
No patients had a mass shadow. Among the non-carriers, eight had nodular shadows, six had cavitary shadows, five had multifocal bronchiectasis with nodular shadows, and four had consolidation on the chest CT scan; one had both cavitary shadowing and consolidation, two had both cavitary and nodular shadowing, and one had both nodules and consolidation. Among the HTLV-I carriers, two had nodular shadows, two had cavitary shadows, seven had multifocal bronchiectasis with nodular shadows, and two had consolidation on the chest CT scan; one had both cavitary shadowing and consolidation, one had cavitary and nodular shadowing, and one had nodules and consolidation. The ratios of the affected areas on the chest CT scans were calculated using the visual score method12 and were significantly higher in the HTLV-I carriers (39.2 (24.6)) than in non-carriers (12.83 (11.9); D = 26.4, 95% CI 12.6 to 40.2, p<0.01, fig 1). The upper lobes and middle and lingular lobes were the predominant locations of bronchiectasis with nodular shadowing in the non-carriers but in the HTLV-I carriers there were no predominant sites for bronchiectasis with nodular shadowing. In both HTLV-I carriers and non-carriers both upper lobes were the predominant locations for cavitary shadows and the right lower lobe was the predominant location for nodular shadowing. Six asymptomatic HTLV-I non-carriers had nodular shadowing, one had cavitary shadowing, and another had bronchiectasis with nodular shadowing. The visual scores in asymptomatic HTLV-I non-carriers were low (5.21 (3.16)).

Comparison of the location of lesions between HTLV-I carriers and non-carriers using the visual score method. The visual score is the percentage of lesions as a proportion of the total pulmonary area shown on the chest CT scan. The visual score was significantly higher in HTLV-I carriers than in non-carriers. Horizontal bars show the mean value in each group.
BAL FLUID ANALYSIS
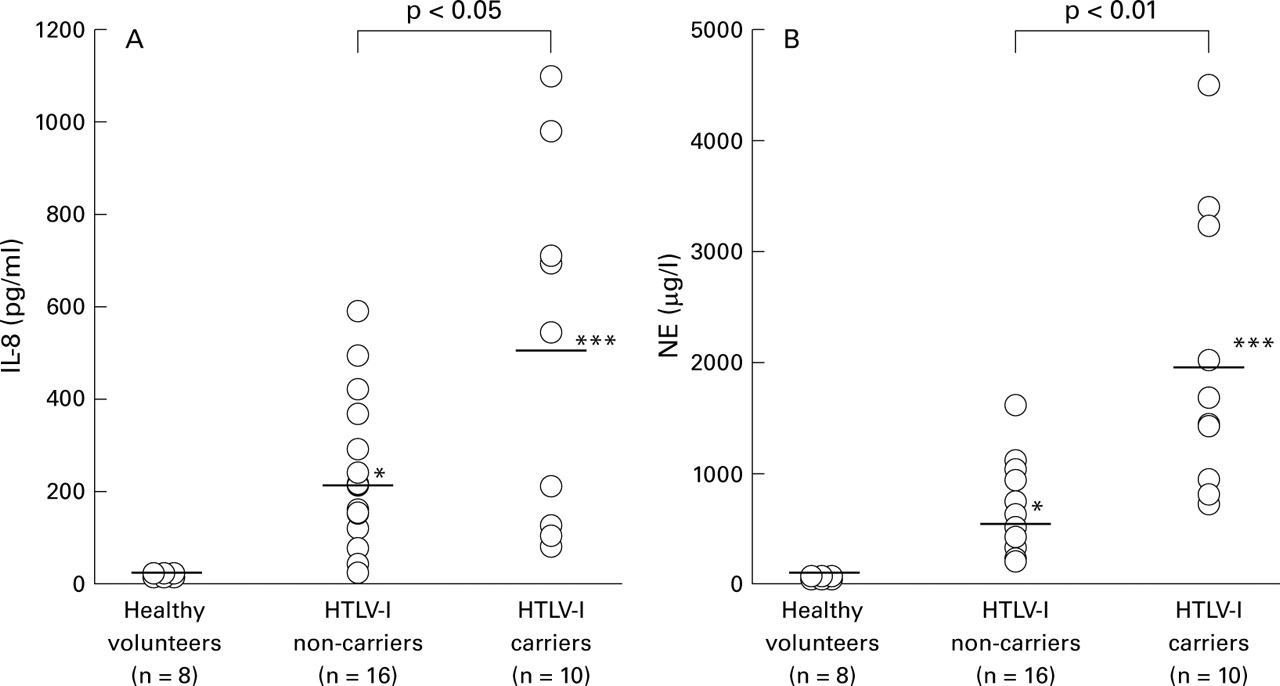
The results of BAL fluid analysis of all HTLV-I carriers and 16 non-carriers without a smoking history compared with those of healthy volunteers are shown in table 2. The total cell count, neutrophil percentage, lymphocyte percentage, and CD4/CD8 ratios were significantly higher in patients with pulmonary MAC infection than in healthy volunteers. However, there were no significant differences between HTLV-I carriers and non-carriers. The concentrations of TNF-α, IL-1β, IL-6, IL-8, and NE were increased compared with the healthy volunteers (table 3). NE and IL-8 were significantly higher in HTLV-I carriers than in non-carriers (NE: D = 1342 μg/l, 95% CI 704 to 1980.3 μg/l, p<0.01; IL-8: D = 304.5 pg/ml, 95% CI 89.7 to 519.4 pg/ml, p<0.05, fig 2). However, there were no differences in the concentrations of TNF-α, IL-1β, and IL-6 between HTLV-I carriers and non-carriers.
Comparison of BAL fluid findings in normal controls, HTLV-I carriers and non-carriers
Analysis of cytokines in BAL fluid
{kind=link}
{kind=link}
Concentrations of (A) interleukin-8 (IL-8) and (B) neutrophil elastase (NE) in HTLV-I carriers, non-carriers, and normal controls. Horizontal bars show the mean value in each group. *p<0.05, **p<0.01, ***p<0.001 compared with normal controls.
A significant correlation was established between the IL-8 concentration and the percentage of neutrophils (r = 0.464, p<0.05) and between the NE concentration and the percentage of neutrophils (r = 0.639, p<0.001). No other correlations were found between the concentrations of cytokines and the cell populations.
Discussion
Atypical mycobacterial infection commonly causes disease in patients with T cell abnormalities such as AIDS1 ,2 or idiopathic CD4+ T cell lymphocytopenia,13 or in patients with malignant tumours.14 In Japan the incidence of atypical mycobacterial infection, especially pulmonary MAC, has been increasing since 1970.15 In our study 34.5% of patients with pulmonary MAC were HTLV-I carriers and this prevalence was significantly higher than the prevalence in all patients admitted to our department between 1994 and 1998 (p<0.05, OR = 2.63, 95% CI 1.21 to 5.68). The prevalence of HTLV-I carriers among all patients was almost the same as that described in a previous report from Kagoshima Prefecture (16.6%) where the prevalence of HTLV-I is relatively high compared with that of the rest of Japan.16 A high prevalence of HTLV-I carriers in patients with respiratory disorders7 such as pulmonary cryptococcosis17has been suggested but, to our knowledge, there are no reports suggesting a high prevalence of HTLV-I carriers in patients with pulmonary MAC.
According to previous reports of patients with pulmonary MAC, the proportion of women was relatively high and productive cough was a common symptom.18 Fever was seen in only about 14% of patients, unlike patients with tuberculosis in whom fever was reported in 35–80% of cases.19 In our study only 21% of non-carriers and 20% of HTLV-I carriers had fever, and productive cough was the predominant symptom. Among the non-carriers, 42.1% did not have clinical symptoms, while other non-carriers showed clinical symptoms. These results were similar to those of Maesakiet al 15 but differed in that all HTLV-I carriers had clinical symptoms. Furthermore, the WBC counts and CRP levels on admission, which are the indices of a systemic defence reaction to infection, were lower in HTLV-I carriers than in non-carriers. This indicates that pulmonary MAC infection in HTLV-I carriers is likely to cause symptoms; however, the systemic inflammatory response to MAC infection is poor.
Radiographically, multifocal bronchiectasis with nodules was common in patients with pulmonary MAC and the predominant lesions on the chest CT scan were in the bilateral upper, middle and lingular lobes.20 In our investigation the incidence of multifocal bronchiectasis with nodular shadowing was high both in HTLV-I carriers and non-carriers. The upper, middle and lingular lobes were the predominant locations of lesions in non-carriers, but there was no predominance in HTLV-I carriers. Cavitary and nodular shadows were more frequent in non-carriers and the predominant locations of these lesions were almost the same as described in previous reports.21The ratio of affected areas on the chest CT scans of patients infected with MAC, calculated by the visual score method,12 was significantly higher in HTLV-I carriers than in non-carriers (fig 1). These results indicate that pulmonary MAC infection in HTLV-I carriers causes diffuse pulmonary lesions.
Few data have been reported on analysis of BAL fluid in patients with pulmonary MAC infection. Yamasaki et al 22 analysed BAL fluid of patients with pulmonary MAC infection without predisposing lung disease and reported significant increases in IL-1β, IL-6, and IL-8 concentrations and an increase in NE associated with the neutrophil count. Heurlinet al 23 also reported an increase in IL-1β and IL-8 concentrations in immunocompetent patients with pulmonary non-tuberculous mycobacteriosis. In our investigation IL-1β, IL-6, IL-8, and NE were all significantly increased compared with healthy volunteers. Furthermore, IL-8 and NE were increased significantly more in HTLV-I carriers than in non-carriers and these cytokines showed significant correlation with the percentage of neutrophils. IL-8 is known as a chemotactic factor for neutrophils, and alveolar macrophages release IL-8 in the early stage of pulmonaryMycobacterium tuberculosisinfection.24 NE is released from neutrophils and is known to damage the airway epithelial cells by overwhelming the normal host defence in airway infection.25 Indeed, the analysis of BAL fluid in this study showed significant positive correlations between these cytokines and the percentage of neutrophils. Our results suggest that there is a high level of neutrophil activity in pulmonary MAC infection in HTLV-I carriers.
In summary, this study of pulmonary MAC infection in HTLV-I carriers has shown three important features: (1) patients are likely to have symptoms without systemic dissemination while indices of systemic inflammation such as CRP levels remain low; (2) radiographically, bronchiectasis with nodular shadowing is common and the lesions are widespread; (3) the BAL fluid concentration of cytokines associated with neutrophil activity such as IL-8 and NE is high. It is unclear why pulmonary MAC infection in HTLV-I carriers causes widespread affected lesions. One possible explanation is that the MAC infection in the HTLV-I carriers in our investigation was more severe than that in non-carriers. We think it is possible that clinically significant MAC infection occurs with a high frequency in HTLV-I carriers because of the immunological effect of retrovirus infection.26 Our study population is too small to draw definitive conclusions and more cases are needed to clarify this point.