Article Text

Statistics from Altmetric.com
Obstructive sleep apnoea (OSA) and central sleep apnoea have been identified and described in adults, children, and infants.1-3 It is not certain, however, if the adult sleep apnoea syndromes, particularly OSA, originate from childhood or whether paediatric and adult sleep apnoea are separate syndromes. Some investigators have suggested that the pathophysiology, criteria for diagnosis, and the management of paediatric patients with OSA are different from that for adults.4-7 Other investigators have found that risk factors, clinical symptoms, and the consequences of OSA share common features between adults, children and infants.8-11 We propose that the adult sleep apnoea syndrome is related to sleep apnoea in children, and that adult patients with sleep apnoea have been predisposed to developing apnoea since early infancy. The differences in OSA in patient populations of different age groups may represent different stages in the development of the adult form of OSA. This review will discuss the similarities and differences between adult, childhood and infant sleep apnoea, particularly OSA. The risk factors, potential mechanisms, and familial factors of OSA will be presented to ascertain the possible genesis of adult sleep apnoea during childhood.
The sleep apnoea syndromes
The OSA syndrome in adults was identified more than 30 years ago,12 has been described extensively in adults, and is believed to be caused by collapse of the oropharyngeal airway.1 It is not certain whether adult patients had OSA as infants or children; however, the diagnosis of OSA in adults often occurs several years after the onset of symptoms, sometimes starting during adolescence. Obstructive apnoea is associated with repetitive episodes of hypoxaemia, sleep fragmentation, and cardiovascular and neurobehavioural sequelae (fig 1).13-15 Several risk factors have been identified that predispose an individual to developing OSA including obesity, age, sex, upper airway structural abnormalities, and a family history of OSA.11 ,16-19

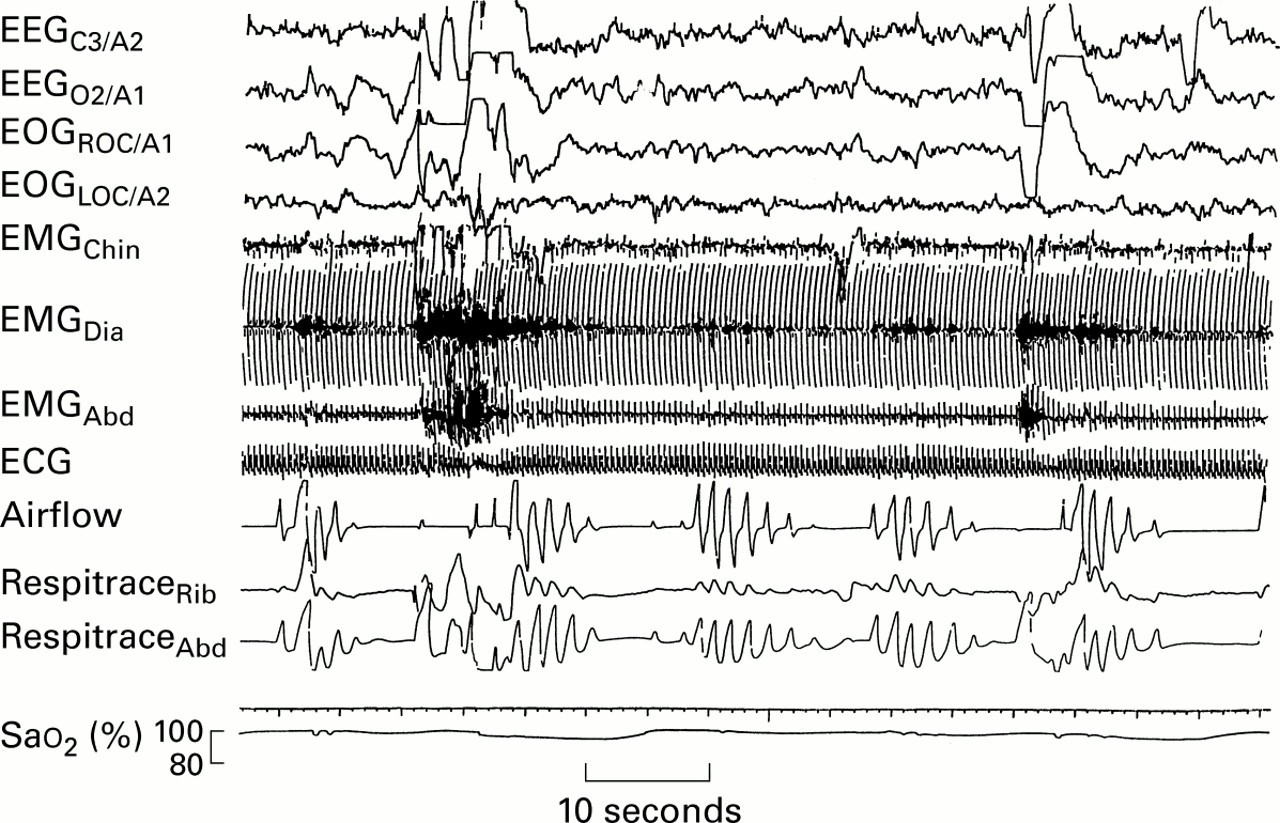
Polygraphic example of repetitive obstructive apnoea. EEGC3/A2 and EEGO2/A1 = central and occipital electroencephalogram, respectively; EOGROC/A1 and EOGLOC/A2 = right and left oculogram, respectively; EMGChin = submental electromyogram; EMGDia = diaphragm electromyogram; EMGAbd = abdominal electromyogram; ECG = electrocardiogram; Airflow = airway pressure measured from nasal prongs; RespitraceRib and RespitraceAbd = thoracic and abdominal movements, respectively; SaO2 = arterial oxyhaemoglobin saturation (%). Inspiration is an upward deflection on the airflow and Respitrace signals. Note that there is a cessation of airflow accompanied by continued deflections from the Respitrace channels. The apnoeas are associated with decreases in Sao 2 to approximately 75% and are terminated by brief arousals.
SLEEP APNOEA IN INFANTS
During the first year of life, marked changes and development of the cardiorespiratory system occur in infants due to growth and maturation of the central nervous system.20 Sleep apnoea is commonly recorded in infants; it is usually central in nature and is considered to be a normal manifestation of the immature central nervous system. Periodic breathing—that is, episodes of repetitive central apnoea—is also a common pattern of apnoea recorded in infants. Central sleep apnoea and periodic breathing during non-REM and REM sleep occur most frequently during the neonatal period and decrease in frequency during the first 6–12 months of life.21-25
OSA has been thought to be rare in infants and few data exist on the occurrence of OSA in normal infants. Upper airway obstruction has been hypothesised to occur in association with craniofacial abnormalities—for example, Pierre Robin sequence,26apnoea of prematurity,27 and apparent life threatening events (ALTE).28 OSA has also been implicated in the mechanisms of the sudden infant death syndrome (SIDS).29-31 The mechanisms of airway obstruction in infants are not certain. In preterm infants it has been suggested that airway closure is caused by decreased upper airway muscle tone.32 Endoscopic examination of the upper airway during obstructive apnoea in infants with ALTE has shown that obstruction occurs at the level of the larynx,28 similar to that observed in adults.1
The occurrence of obstructive and central sleep apnoea in some infants has been shown to change during the first year of life (fig 2). In a group of infants with OSA who had either experienced an ALTE or had a family history of SIDS it was found that OSA peaked in severity at approximately two months of age and subsequently improved and resolved with age.33 Their apnoea was dominated by periodic breathing involving predominantly mixed apnoea, a pattern not unlike the repetitive obstructive apnoeas recorded in adults. This supports the speculation that OSA in paediatric patients is a precursor for adult OSA. Although the apnoea resolved with development, it is possible that infants with this pattern of apnoea during the first year of life may be predisposed to upper airway obstruction and may therefore be likely to develop OSA later in life.

Polygraphic example of central and obstructive apnoeas in an infant aged two months. Abbreviations as for fig 1. Note that there are repeated short apnoeas (<10 seconds in length) that are mixed or central in nature. Also note that the first mixed apnoea is terminated with a brief EEG arousal while the other apnoeas are terminated without any changes in the EEG.
SIDS, ALTE AND ITS ASSOCIATION WITH OSA
It has been suggested that SIDS, ALTE, and OSA in infants have similar pathophysiological mechanisms and recently these have been linked to the adult OSA syndrome.34-37 Obstructive and central apnoea has been recorded during sleep in infants who have experienced an ALTE.28 ,34 ,35 In addition, several studies have reported obstructive events during sleep in infants who subsequently became victims of SIDS.29-31 Guilleminaultet al 30 were the first to document obstructive apnoea in an infant with laryngomalacia who subsequently died of SIDS. Kahn et al 29 and later Schlüter et al 31 found that infants who subsequently died of SIDS had obstructive events more commonly recorded on a previous polysomnographic study than matched controls or infants who died from other known causes. These findings have suggested that upper airway obstruction is probably involved in the mechanisms of SIDS and ALTE.
More recently Rees et al 38 have presented further evidence that infantile OSA, SIDS, and the adult OSA syndrome are related. These investigators found differences in the facial structure of infants who died of SIDS compared with control infants. The anatomical features found in the SIDS cases—namely, a retrognathic facial structure—would predispose these infants to narrowing and occlusion of their upper airways. This anatomical feature is similar to that found in many patients with the adult OSA syndrome. Facial structure is believed to be, at least in part, genetically inherited and it is likely that a predisposition to develop OSA either in childhood or adulthood has been determined prenatally.
OSA IN CHILDREN
Upper airway obstruction has been recorded in children and, although no population studies have been performed, it is now considered to be a common problem.39 Polygraphic studies performed in children with symptoms of OSA have shown that many children with clinically significant upper airway obstruction have a pattern of continuous partial obstruction (fig 3) rather than the repetitive complete obstructive apnoea seen in adults with OSA.4 ,40 It has been speculated that partial upper airway obstruction in children is a precursor to the adult form of OSA. A potential explanation for the difference in the pattern of obstruction between children and adults could be the recruitment of accessory respiratory muscles that occurs more often in children. Airway maintaining and expiratory muscles are frequently recruited during loaded breathing and partial obstruction in children41 ,42and it is possible that this reflex muscle recruitment diminishes with age and disease progression.
{kind=link}
{kind=link}
{kind=link}
Polygraphic example of repetitive episodes of partial obstruction in a four year old boy. Abbreviations as for fig 1. Note that there are repetitive hypopnoeas and an obstructive apnoea that are associated with paradoxical thoracic and abdominal respiratory movements and the inspiratory phase of the airflow shows a typical pattern of airway limitation.
The association between childhood and infantile OSA is not certain; however, Guilleminault and colleagues43 ,44 have reported the development of OSA from infancy to childhood. In a group of children who were first diagnosed with apnoea following an ALTE during the first four months of life, more florid symptoms of obstruction developed and they were diagnosed with OSA by five years of age. These reports suggest that the onset of obstructive sleep apnoea may occur very early in life.
Symptoms and consequences of OSA
The clinical symptoms and consequences of OSA vary between infants, children, and adults. In adults, regardless of when the diagnosis of OSA was confirmed, the onset of symptoms can often be traced back to adolescence or childhood. In adults the most common symptom includes daytime hypersomnolence which is believed to be caused by the sleep fragmentation associated with the repeated obstruction.13 ,45 In contrast, excessive daytime sleepiness is not frequent in children who have OSA.5Behavioural problems such as hyperactivity and aggressiveness have been reported, and learning problems in school aged children can occur.2 ,46 ,47 In infants the effect of OSA on daytime behaviour is difficult to measure; however, in infants whose OSA was treated with nasal continuous positive airway pressure (CPAP) parents reported a change in the infants' alertness during wakefulness following treatment.48
OSA in adults is associated with repetitive arousals from sleep, terminating the obstructive event and resulting in sleep fragmentation.1 ,13 However, the majority of apnoeas recorded in infants and children are resolved without any change in the EEG pattern.49 The association of apnoea with arousal is age related; a higher percentage of apnoeas are terminated with an arousal as age increases, suggesting a relationship between change with development of OSA and arousal between infants, children, and adults. It has been suggested that subcortical arousals may be important in infants and children.50 ,51 Recently, however, it was found that termination of obstructive apnoea in adults, as in children, did not always occur with an EEG arousal and was sometimes accompanied by subcortical responses in the absence of an EEG arousal.52
The sleep disturbances in patients with OSA have significant effects on sleep architecture. In infants OSA is associated with shortened episodes of REM sleep and an overall decrease in the amount of REM sleep.33 In contrast, in children OSA is associated with a decrease in slow wave sleep47 and in adults a deficit of REM sleep and slow wave sleep have been associated with OSA.53 When sleep apnoea is prevented by CPAP treatment or resolved with development, the sleep disturbances are at least partly reversed.48 ,53 ,54
Snoring during sleep is another predominant symptom in adults with OSA.13 ,45 ,55 Snoring is also a common feature in children with OSA2 ,7 ,47 but has rarely been reported to be associated with OSA in infants. However, Kahn et al 10 recorded snoring and noisy breathing in infants with obstructive apnoeas during sleep. The snoring in their study is possibly equivalent to the intermittent noisy or laborious breathing that has been described by other investigators.30 ,37 ,43 In addition to snoring, other symptoms that were apparent in infants with abnormal breathing during sleep included breath holding spells, fatigue during feeding, and profuse sweating during sleep.10 OSA symptoms in children reported by parents include sweating, restlessness during sleep, frequent awakenings and, in some cases, nocturnal enuresis.2 ,47 ,56
More recently the focus of OSA has been on the cardiovascular consequences, in particular the effect of obstructive apnoea on blood pressure responses. OSA in adults is associated with an increased frequency of systemic hypertension.57 ,58 Pulmonary hypertension has been recorded in children with OSA but systemic hypertension secondary to OSA is thought to be uncommon in children.7 This could indicate that the haemodynamic effects of OSA are the result of a prolonged disease or that they were not recognised in children. Recently, however, OSA in children was found to be associated with an increased diastolic blood pressure and the increase in blood pressure could be predicted by the apnoea index and body mass index.9
Risk factors for OSA
Obesity is reported in a high proportion of adult patients with OSA13 ,59 but is not always found in paediatric patients with OSA, with varying prevalences of OSA being reported in obese children.60 ,61 A high prevalence of OSA has been recorded in overweight infants in the absence of clinical symptoms.62 In infants and young children, however, failure to thrive is commonly associated with OSA63 and relief of the OSA by surgery or CPAP treatment often results in “catch up” growth.2 ,54 ,64
In adults the incidence of OSA increases with age and is more common in men. Approximately 9% and 4% of middle aged men and women, respectively, are reported to have OSA.14 In children the prevalence of OSA has been studied in children up to six years of age using overnight video recording and oximetry and questionnaires. Approximately 1% of children of pre-school age are believed to have OSA7 and there is conflicting evidence about its sex distribution. Carroll and Loughlin5 reported that there was no sex difference in children with OSA; however, Marcuset al 9 found that OSA was more common in boys. There are no reliable data on the prevalence of OSA or any sex differences during infancy. In SIDS victims, however, there is a male predominance with approximately 60% of cases being boys.65
Other less common risk factors may vary among the different patient groups. Structural malformation of the brainstem that occurs in myelomeningocele, for example, is associated with obstructive and central apnoea.66 Respiratory infections and allergic rhinitis can exacerbate and induce obstructive apnoeas in children and adult patients.61 ,67 In infants a viral respiratory infection such as respiratory syncytial virus can cause life threatening obstructive apnoea.68 These findings suggest that increased nasal resistance and airway inflammation may be involved in the pathogenesis of OSA in all patients.
Structural abnormalities and OSA
Potential causes of OSA include anatomical abnormalities of the face and upper airway. The anatomical features may involve the bone or the mucosa and soft tissue development and structure. Some investigators have suggested that the existence of any anatomical features leading to a narrow upper airway may favour the development of sleep disordered breathing from early infancy to adulthood.44
OSA is common in infants and children who have anatomical abnormalities involving the face, mandible, and the size of the upper airway. These abnormalities include laryngomalacia; mid face hypoplasia that occurs, for example, with Down's syndrome; or the micrognathia, cleft palate, and macroglossia that occurs in the Pierre Robin sequence.69 ,70 The obstruction in these infants and children is often relieved by surgery to correct the site of obstruction; however, follow up of these patients to ensure that OSA does not return with age has been limited.
Adenotonsillar hypertrophy is frequently assumed to be the predominant cause of childhood OSA, and removal of the tonsils and adenoids usually results in relief of obstructive symptoms.2 ,46 ,47 ,71Some children, however, continue to have residual OSA following adenotonsillectomy.72 In addition, the severity of the OSA before surgery is not always proportional to the size of the tonsils and adenoids.73 ,74 These findings suggest that other factors such as abnormal ventilatory drive, mechanical abnormalities, and other anatomical abnormalities of the upper airway may be involved in the mechanisms of OSA. In reality the size of the tonsils and adenoids is rarely the primary problem. The severity of OSA has been reported to be inversely related to the size of the posterior airway74; other investigators have shown that children with OSA have a more collapsible upper airway than age matched controls75 and similar findings have been reported in adults.76
A prospective cohort investigation of prepubertal children with OSA found that the symptoms resolved 2–4 months after tonsillectomy but that apnoeas during sleep recurred years later at puberty.77 Cephalometric radiography indicated a reduced posterior airway space in these children. The upper airway and craniofacial anatomy are influenced by genetic factors and the development of OSA may be predetermined from childhood. Evaluation of upper airway and craniofacial morphology in children with OSA may identify patients at risk of persisting or recurring symptoms later in life. It is possible that OSA originates from prenatal factors that will lead to a development of OSA at various stages throughout life.
Familial OSA syndrome
There is significant evidence that familial factors influence the risk of developing upper airway obstruction in both paediatric and adult patients. OSA in adults has been shown to aggregate significantly within some families.19 ,78-82 The familial occurrence of OSA was first described by Strohl et al 78 who reported OSA in several members of one family. In addition, an infant of this family had died of SIDS and it was speculated that SIDS may have been related to the familial OSA. Family studies have shown that relatives of patients with OSA have a 2–4 fold increased risk of developing OSA compared with controls.19 It has been suggested that members of such families are predisposed to developing upper airway obstruction due to genetic risk factors including obesity, craniofacial morphology, and an abnormality of ventilatory and respiratory muscle control.78 ,79 ,83 In some families subtle craniofacial anatomical abnormalities have been detected and differences in the ventilatory responses to hypoxia and hypercapnia have been found when compared with controls.
More recently a co-aggregation of familial OSA with SIDS and ALTE in infants was identified within families.84 ,85 Tishler and colleagues84 found that 10 of 91 families with OSA studied had at least one case of sudden unexpected infant death or ALTE, whereas there were no such cases in control families with no OSA. Similarly, Mathur and Douglas85 reported, from a mailed questionnaire, that SIDS occurred more commonly in families that had members with OSA than in control families. It has previously been shown that ALTE and SIDS aggregates within some families, and abnormalities in the sleep and breathing patterns of these infants have been recorded.86 Guilleminault et al 87 presented five families with at least two cases of SIDS and/or ALTE and adult OSA among their family members. It was found that infants in these families had OSA which persisted into childhood. A small airway was a common feature in the members of these families. Recently we have examined the incidence of OSA in infants who have multiple cases of SIDS, ALTE, and/or adult OSA among family members.88 We found that the majority of infants who had a family history of multiple cases of SIDS, ALTE and/or adult OSA had OSA recorded during infancy, whereas only about one third of infants with a single case of SIDS or ALTE within their family and no OSA in adult family members had OSA. We hypothesised that these infants were possibly genetically predisposed to develop OSA. It is therefore possible that these infants will be predisposed to developing OSA later in life.
An abnormal central ventilatory control as well as craniofacial morphology have been proposed as risk factors for familial OSA, and these features are believed to be at least partly genetically determined.89 Pillar et al 90 showed that healthy offspring of patients with OSA were more likely to collapse their airway with loaded breathing than normal controls. Redline et al 91 showed that ventilatory responsiveness to hypoxia and hypercapnia was depressed in family members of OSA patients. In addition, a depressed response to hypoxia has been recorded in the siblings of infants with SIDS92 and also in the parents of SIDS victims.93
There is significant evidence that familial factors probably influence the risk of developing OSA in adulthood. Adult physicians and paediatricians should consider looking for the presence of OSA symptoms in relatives of their patients. Information from these patients will provide a better understanding of the development of OSA, may identify patients with familial features who are at risk of developing the OSA syndrome, and could prevent OSA and its consequences in some cases.79 ,94
Conclusions and future research
Infantile and childhood OSA is probably related to the adult OSA syndrome and the possibility of developing OSA during adulthood might be predicted during childhood. The anatomical abnormalities that predispose an individual to OSA are similar across the age groups. The findings of the familial OSA syndrome and its association with SIDS, ALTE and infantile OSA suggest further that adult OSA may be predetermined during infancy or childhood. There is little evidence, however, that adults with OSA had sleep disordered breathing during infancy and/or childhood. Continued contact with the infants that we have studied during the next several years may document the development of OSA in children and adults. In addition, population studies in infants and children are necessary to determine the prevalence and extent of the disease in the paediatric population. Although some investigators believe the OSA syndromes in infants, children and adults could be viewed as three separate syndromes, we believe that they represent different developmental stages in the progression of OSA from infancy to adulthood.