Article Text

Abstract
BACKGROUND Nitric oxide (NO) plays an important role as an inflammatory mediator in the airways. Since chronic obstructive pulmonary disease (COPD) is characterised by airway inflammation, a study was undertaken to determine NO levels in the exhaled air of patients with COPD.
METHODS Two groups of patients with clinically stable COPD were studied, 10 current smokers and 10 ex-smokers. Two control groups of healthy subjects consisting of 10 current smokers and 20 non-smokers were also studied. Exhaled NO levels were measured by the collection bag technique and NO chemiluminescence analyser.
RESULTS Mean (SE) levels of exhaled NO in ex-smokers and current smokers with COPD (25.7 (3.0) ppb and 10.2 (1.4) ppb, respectively) were significantly higher than in non-smoker and current smoker control subjects (9.4 (0.8) ppb and 4.6 (0.4) ppb, respectively). In current smokers with COPD exhaled levels of NO were significantly lower than in ex-smokers. In this latter group of patients there was a significant negative correlation between smoking history (pack years) and levels of exhaled NO (r = –0.8, p = 0.002). A positive correlation was seen between forced expiratory volume in one second (FEV1) and levels of exhaled NO (r = 0.65, p = 0.001) in patients with COPD.
CONCLUSIONS These data show that exhaled NO is increased in patients with stable COPD, both current and ex-smokers, compared with healthy control subjects.
- exhaled nitric oxide
- chronic obstructive pulmonary disease
- smoking
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) is a chronic, slowly progressive disorder characterised by airway obstruction that does not change markedly over several months.1 Airway inflammation plays an important role in the pathogenesis of mucus hypersecretion,2 lung destruction,3 and airway obstruction,4 which are all characteristic features of COPD.
In the past, nitric oxide (NO) was regarded exclusively as an atmospheric contaminant. Currently, however, it is thought to play an important endogenous signalling role in the physiological control of airway function and in the pathophysiology of airway diseases.5 NO is produced endogenously in the human respiratory tract where it can act as a dilator of bronchial and vascular smooth muscle, a neurotransmitter, and an immune response mediator.6 Measurement of NO in exhaled air is a simple method of investigating endogenous NO production7 and is under investigation by many research groups.8 Increased levels of exhaled NO have been reported in patients with inflammatory lung disorders such as bronchial asthma9 and bronchiectasis.10 The purpose of this study was to investigate levels of exhaled NO in a group of patients with clinically stable COPD.
Methods
SUBJECTS
The study population consisted of 20 patients with stable COPD recruited from Servizio di Fisiopatologia Respiratoria, Azienda Ospedaliera di Parma (PR), Italy and 30 healthy control subjects. The subjects were divided into four groups based on their smoking habit (table 1). The groups were matched according to smoking history (22 of 30 subjects had a smoking history >30 pack years). Although normal individuals were not age matched, no relationship between age and exhaled NO has been reported, at least in adults.
Mean (SE) clinical and functional characteristics of subject groups
Inclusion criteria for COPD were chosen according to the British Thoracic Society guidelines1: (a) evidence of airways obstruction (FEV1 <80% of predicted and FEV1/VC ratio <70%); (b) no improvement in FEV1 of more than 15% after inhalation of 200 μg salbutamol; (c) history of chronic progressive symptoms such as wet cough, wheeze and breathlessness. Exclusion criteria were: (a) history of atopy or evidence of atopy on skin prick testing for common inhaled allergens, (b) history of asthma or other pulmonary disease, (c) treatment with oral or inhaled glucocorticoids or antibiotics during the month before entering the study. Patients were not excluded if they were receiving short acting or long acting β2 agonists, or both, since these drugs are reported not to modify exhaled NO levels.11
The patients with COPD were clinically stable and had had no exacerbation of their disease, defined as increased dyspnoea associated with change in quality and quantity of sputum within the preceding month. Their smoking history was carefully controlled and a smoking history of at least 15 pack years was required. Before entry to the study patients were screened by clinical history, physical examination, electrocardiography, urinalysis, and haematological and blood chemistry tests. Chest radiography was performed to exclude other lung diseases.
All the subjects who smoked cigarettes at the time of the study, whether COPD patients or healthy controls, were considered to be current smokers; all the others were considered to be non-smokers or ex-smokers (smoking cessation >1 year). Current smokers in both groups were asked to refrain from smoking for at least 12 hours before the measurement of exhaled NO levels.
All the subjects gave their written informed consent to participate, and the study protocol was approved by the local ethical committee.
BREATHING MANOEUVRE
Subjects were seated and were asked to inspire room air via the mouth to total lung capacity and to exhale through a mouthpiece. Mixed exhaled air was collected using a three way stopcock into two sequential bags. In the first bag the first eight seconds (640 ml) of exhaled air was collected, representing the anatomical and mechanical dead space, and into the second bag the remaining exhaled air was collected. Subjects performed three exhalations and the mean value was calculated. In accordance with the European guidelines,12only the second portion of exhaled air was used for exhaled NO measurements.
The bags used were made of polyvinylfluoride film with a volume of 10 litres (Tedlar Samples Bags, SKC Inc, Philadelphia, USA); the concentration of NO in the bags did not change for at least six hours, as tested in separate experiments (data not shown).
During the expiration each subject maintained a constant expiratory flow (4.8 l/min) verified by a flow meter positioned between the mouth and the bags. Samples were discharged if the subject did not keep a constant flow. In a preliminary study we verified that an expiratory flow rate of 4.8 l/min with a constant resistance permitted a mouth pressure of 20 cm H2O to be reached, as shown by a manometer (Dwyer Instrument Inc, Michigan City, Indiana, USA) with a side arm inserted between the mouth and the flow meter. With this mouth pressure the soft palate rises and closes the access to the nasal space above, preventing leakage of nasal NO into the mouth during expiration.12 To prevent condensation of vapour on the walls of the bags a Teflon column, 20 × 60 mm packed with 6 g of silica gel (particle size 1.7–4 mm; E Merck, Darmstadt, Germany) was inserted between the mouthpiece and the bags.
Samples of exhaled air packed in bags, covered with black cloths, were transported to the laboratory and analysed within 60 minutes. To measure ambient NO, samples of air from the room in which the subjects performed the test were collected into bags by a pump immediately before exhaled NO evaluations.
MEASUREMENT OF NO
The levels of exhaled and ambient NO were measured using a chemiluminescence NO analyser (Model 42S; Thermo Environmental Instruments Inc, Franklin, Massachusetts, USA). The analyser measures photons resulting from oxidisation of NO by ozone using a photomultiplier at a sampling flow rate of 0.7 l/min with a response time of 10 s (it takes three measurements to reach the highest stable exhaled NO value). The instrument was calibrated daily over the range of 0–100 parts per billion (ppb) with dilutions of a known NO source (SAPIO, Milan, Italy) by using a multigas precision flow calibrator (Dynamic Gas Calibration System, Model 146, Environmental Instruments Division, USA). Before all NO measurements were made, NO-free air was passed through the analyser for NO zeroing.
DATA ANALYSIS
Group data were expressed as mean (SE) or median and range where appropriate. Coefficient of variation was used to test the repeatability of exhaled NO measurements. Comparisons between data from COPD and control subjects were tested using the Mann-Whitney U test; correlations between exhaled NO levels and smoking history and lung function tests were tested with Spearman’s rank test. A p value of <0.05 was regarded as significant.
Results
All the subjects performed the tests correctly without discomfort.
The mean coefficient of variation of the three exhaled NO measurements in COPD patients and in control subjects was 3.7 (0.7)% (range 0–11.9%) and 2.2 (3)% (range 0–6.7%), respectively. Ambient NO was always <20 ppb and no correlation was found between ambient and exhaled levels of NO (data not shown).
NO levels in exhaled air in patients with COPD who were ex-smokers (25.7 (3.0) ppb) and current smokers (10.2 (1.4) ppb) were significantly higher than in non-smoker (9.4 (0.8) ppb; p = 0.0001) and current smoker (4.6 (0.4) ppb; p = 0.0007) healthy control subjects (fig 1).

Exhaled NO levels in ex-smoker COPD patients (○), non-smoker healthy control subjects (□), current smoker COPD patients (•), and current smoker healthy control subjects (•). Horizontal bars represent median values.
Levels of exhaled NO in current smokers were significantly lower in both COPD patients and healthy control subjects than in COPD patients who were ex-smokers (p = 0.0005) and in non-smoker healthy control subjects (p = 0.0001; fig 1).
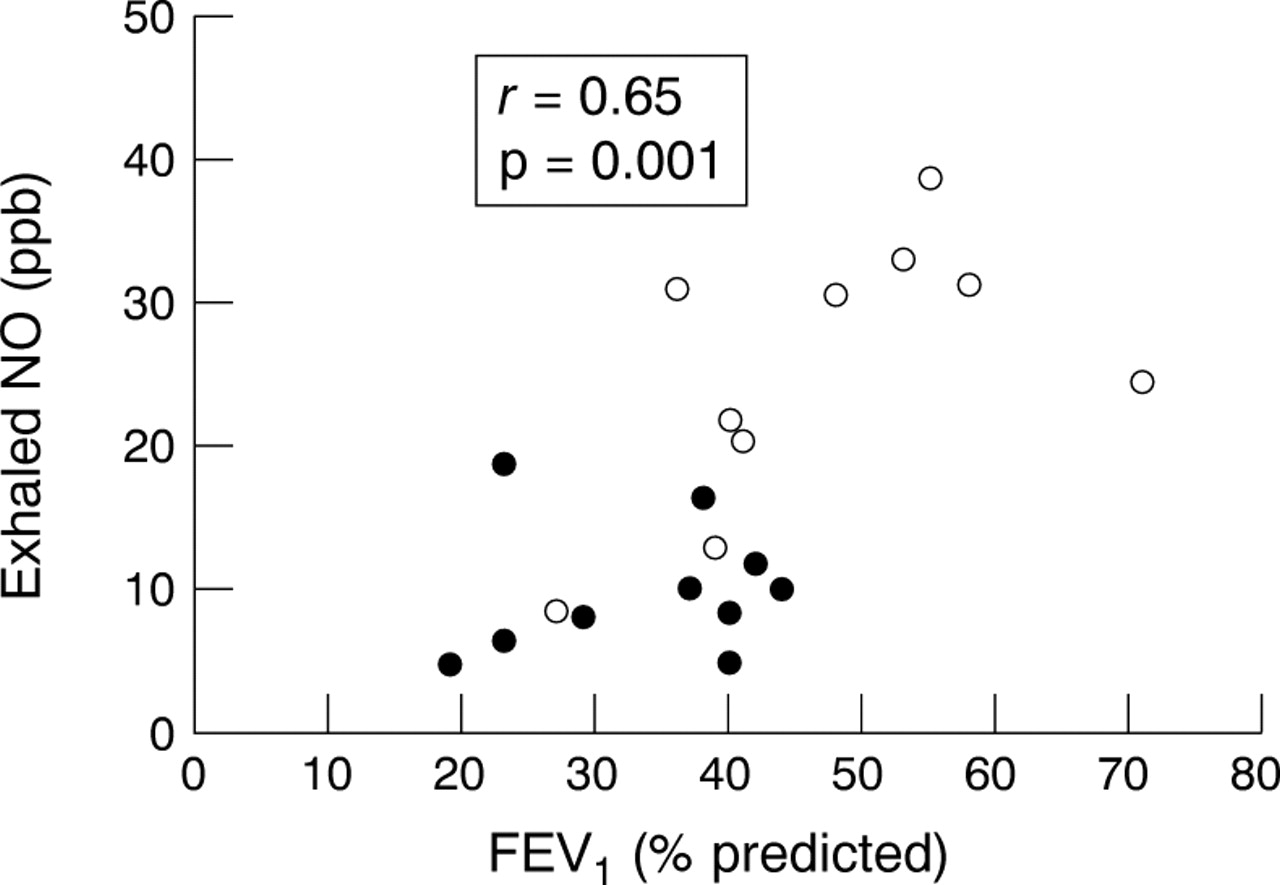
In COPD patients who were ex-smokers there was a significant negative correlation between smoking history (pack years) and levels of exhaled NO (r = –0.8, p = 0.002, fig 2). A positive correlation was found between FEV1 (% predicted) and exhaled NO levels (r = 0.65, p = 0.001, fig3) in patients with COPD.

Relationship between smoking history (pack years) and exhaled NO levels in ex-smoker patients with COPD.

{kind=link}
{kind=link}
{kind=link}
Relationship between FEV1 (% predicted) and exhaled NO levels in patients with COPD. Open symbols represent ex-smokers; closed symbols represent current smokers.
Discussion
Our results show a significant increase in the concentration of exhaled NO in patients with stable COPD, both current and ex-smokers, compared with smoking and non-smoking healthy subjects. The levels of exhaled NO were significantly positively correlated with lung function as assessed by FEV1. Cigarette smoke had a negative influence on levels of exhaled NO in both healthy subjects and in patients with COPD.
Our data in COPD patients confirm and extend previous observations of Maziak et al.13 We observed increased levels of exhaled NO in both current and ex-smokers with stable COPD compared with both smokers and non-smokers in a group of healthy subjects. Maziak et al 13 did not measure exhaled NO levels in non-smoking healthy subjects in their study. However, on the basis of their previous reports, they affirmed that levels of exhaled NO in patients with COPD were not high when compared with normal non-smoker subjects. This discrepancy may be explained by the fact that in both studies only a small number of patients were analysed. Also, it is well known that the term COPD covers a very heterogeneous group of patients.1 Moreover, confounding factors such as inhaled steroid treatment (it is known that inhaled steroids modify exhaled NO14), different smoking histories, and different methodologies for measurement of exhaled NO levels (on line technique compared with collection bag technique) could have influenced exhaled NO levels. This might also explain why higher levels of exhaled NO were observed in all our subjects compared with those measured by Maziaket al.13 In this respect, levels of exhaled NO in our smoking and non-smoking healthy subjects were similar to those previously reported in studies where the collection bag technique was used.15 ,16
In a recent study Robbins et al 15 did not observe increased levels of exhaled NO in a group of COPD patients when compared with healthy subjects. However, this result cannot be compared with ours as Robbinset al did not subdivide their patients according to smoking habit.
The significant positive correlation between FEV1 and exhaled levels of NO in patients with COPD suggests that the reduced levels of exhaled NO could contribute to airway obstruction. In this regard, endogenous NO has an inhibitory effect on bronchial obstruction.17 However, we cannot exclude the fact that statistical bias could have influenced our correlation. We think that it is important to be cautious about interpreting a correlation analysis involving two independent groups with quite different mean values from one or both of the correlating variables since this can lead to false correlation. Additional studies are therefore warranted to ascertain the pathophysiological role of NO in the airways of patients with COPD.
Moreover, though our findings confirm those of Kanazawaet al 18 who studied levels of exhaled NO in smokers with mild obstruction, they contradict Maziak and co-workers13 who found an inverse correlation between FEV1 and exhaled NO levels in patients with COPD. This discrepancy could be explained by the fact that Maziaket al 13 correlated levels of exhaled NO and FEV1 in both stable and unstable COPD patients. In unstable COPD patients activated inflammatory cells in the airways may account for an increase in NO production19 ,20in association with a decline in FEV1.21
The concentration of exhaled NO was significantly reduced in current smokers compared with non-smokers, both patients with COPD and healthy subjects. This confirms previous results.13 ,22 In addition, we observed a negative correlation between exhaled levels of NO and smoking history expressed as pack years in ex-smoker patients with COPD. This might suggest that cigarette smoke induces chronic damage on NO-producing cells in the airway.
We acknowledge that the relatively small number of patients is a potential weakness of our study. Moreover, measurements of urinary cotinine levels and exhaled carbon monoxide should have been done to confirm the smoking history of our patients.
Levels of exhaled NO have been reported to be increased in inflammatory chronic lung diseases such as asthma and bronchiectasis. We extend this observation to patients with clinically stable COPD. The usefulness of the measurement of exhaled NO levels in the clinical management of COPD should be evaluated in long term clinical trials in patients with COPD during exacerbations and after treatment.
Acknowledgments
We would like to thank Elisabeth de Young from the Linguistic Centre, University of Parma for her help with the final text of this manuscript. We also thank Cristiano Immovilli and Alessandro Pelizzoni from ARPA, Parma, for their excellent help in maintaining the analyser. The study was partially supported by a grant from Ministero dell’Università e Ricerca Scientifica e Tecnologica, Rome, Italy.