Article Text

Abstract
Purpose Malignant pleural mesothelioma (MPM) has a high symptom burden and poor survival. Evidence from other cancer types suggests some benefit in health-related quality of life (HRQoL) with early specialist palliative care (SPC) integrated with oncological services, but the certainty of evidence is low.
Methods We performed a multicentre, randomised, parallel group controlled trial comparing early referral to SPC versus standard care across 19 hospital sites in the UK and one large site in Western Australia. Participants had newly diagnosed MPM; main carers were additionally recruited. Intervention: review by SPC within 3 weeks of allocation and every 4 weeks throughout the study. HRQoL was assessed at baseline and every 4 weeks with the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire Core 30. Primary outcome: change in EORTC C30 Global Health Status 12 weeks after randomisation.
Results Between April 2014 and October 2016, 174 participants were randomised. There was no significant between group difference in HRQoL score at 12 weeks (mean difference 1.8 (95% CI −4.9 to 8.5; p=0.59)). HRQoL did not differ at 24 weeks (mean difference −2.0 (95% CI −8.6 to 4.6; p=0.54)). There was no difference in depression/anxiety scores at 12 weeks or 24 weeks. In carers, there was no difference in HRQoL or mood at 12 weeks or 24 weeks, although there was a consistent preference for care, favouring the intervention arm.
Conclusion There is no role for routine referral to SPC soon after diagnosis of MPM for patients who are cared for in centres with good access to SPC when required.
Trial registration number ISRCTN18955704.
- mesothelioma
- palliative care
Statistics from Altmetric.com
Key messages
What is the key question?
Does regular early specialist palliative care (SPC) soon after the diagnosis of malignant pleural mesothelioma (MPM) lead an improved health related quality of life, when compared with standard care alone?
What is the bottom line?
Health-related quality of life did not differ in patients with MPM receiving regular early SPC compared with standard care, and there was no difference in anxiety/depression scores or survival.
Why read on?
This finding is in contrast to other studies of other cancer types and healthcare systems. Patients who are cared for in specialist centres with dedicated nurse specialists may be having their early holistic needs met.
Introduction
Mesothelioma is a malignancy of mesothelial cells caused by exposure to asbestos fibres. It occurs most frequently in the pleura but may affect the peritoneum.1 2 Patients with mesothelioma have a high burden of symptoms,3 4 and median survival is less than 1 year.5 The UK and Australia have some of the highest death rates in the world from mesothelioma.6 7 The global burden of mesothelioma largely reflects historic industrial utilisation of asbestos throughout the last century. While many estimates suggest that developed countries are probably approaching the peak of mesothelioma incidence now, the continuing presence of asbestos within the built environment is likely to lead to continuing cases of mesothelioma for decades to come.
The treatment of mesothelioma remains a significant challenge. Treatment includes combination chemotherapy with cisplatin (or carboplatin) and pemetrexed, which confers an improvement of 2–3 months in survival.8 There is increasing interest in immunotherapy9; however, to date, there is no clear role for this; surgery remains highly controversial with no quality trial data to inform clinical practice.10
Specialist palliative care (SPC) is the active, total care of patients with advanced, progressive malignant and non-malignant life-limiting illnesses11 and those who care for them. SPC involves the management of physical symptoms and is also concerned with the provision of psychological, social and spiritual support. The fundamental aim of SPC is to contribute to achievement of the best quality of life possible for patients and their families at any time between diagnosis and death. A recent Cochrane review examining early palliative care in the context of advanced cancer12 included seven randomised studies (five examining mixed cancer types, one pancreatic cancer and one non-small cell lung cancer).13–19 The review concluded that there is evidence of a small increase in HRQoL with early integrated SPC provision, but the level of certainty of current evidence is low to very low. A more recent single-centre randomised study of mixed advanced tumour types also reported a small to moderate improvement in HRQoL.20
The aim of this study was to examine the effect of regular early SPC in combination with current standard care on HRQoL in patients with malignant pleural mesothelioma (MPM) and their carers compared with standard care alone.
Methods
Trial design
We performed a multicentre, randomised, non-blinded, parallel group controlled trial comparing early referral to regular SPC versus standard care. The protocol has been published in detail previously.21
Setting
There were 19 recruiting secondary and tertiary hospital sites in the UK and one large tertiary site in Western Australia (WA).
Participants
The inclusion and exclusion criteria are listed in box 1. All potential participants were screened for eligibility at specialist thoracic cancer multidisciplinary team (MDT) meetings. Participants were encouraged to nominate a main carer for inclusion in the study, although those who did not were still eligible.
Inclusion and exclusion criteria for the RESPECT-Meso study
Inclusion criteria
Histological or cytological confirmation of malignant pleural mesothelioma (MPM).
European Cooperative Oncology Group Performance Score of 0–1 (0 indicating the patient is asymptomatic, 1 indicating some symptoms but ambulatory).
Diagnosis of MPM received within the last 6 weeks.
Participants were able to provide informed consent in English and comply with trial procedures.
Exclusion criteria
Another known malignancy within 5 years (excluding localised squamous cell carcinoma of the skin, cervical intraepithelial neoplasia, grade III and low-grade prostate cancer (Gleason score<5, with no metastases)).
Significant morbidity that might unduly confound or influence health-related quality of life (HRQoL).
A symptom burden sufficient to require referral to specialist palliative care at the time of diagnosis.
Concurrent or less than 3 months since participation in another clinical trial that may affect HRQoL.
Surgery for MPM including cytoreductive, tumour debulking, radical decortication or extrapleural pneumonectomy (video-assisted thoracoscopic surgery or ‘mini’ thoracotomy for pleurodesis and diagnosis attempts were permissible).
Chemotherapy for MPM initiated prior to consent.
A significant history of depression/anxiety/psychiatric illness requiring specialist hospital care within the last 12 months.
Randomisation and blinding
Following completion of the baseline assessments, eligible patients and their carers were randomised using minimisation with a random element in a 1:1 ratio between the intervention and control groups using an automated, centralised randomisation database, managed by the Oxford Respiratory Trials Unit, Oxford, UK. Minimisation was performed according to: centre, plan for chemotherapy (yes/no), European Cooperative Oncology Group (ECOG) Performance Score (PS) (0 or 1) and histological subtype (epithelioid vs non-epithelioid (biphasic, sarcomatoid, not defined)). Due to the nature of the intervention, it was not possible to blind participants or the immediate research team to the allocated intervention.
Intervention
Participants randomised to regular early SPC were reviewed by a palliative care physician within 3 weeks of allocation with carers encouraged to accompany the participants. SPC visits continued every 4 weeks (within ±7 days) for at least 24 weeks, until death or end of trial. To ensure a standard approach to SPC consultations across different centres, we used the Sheffield Profile for Assessment and Referral to Care tool22 and the revised Edmonton Symptom Assessment System23 at initial consultations for all participants. Therefore, each SPC consultation included an assessment of the participant’s physical, psychological, social and spiritual needs, with provision of additional treatments and referral to additional support services as required.
Control arm
Control group participants received all appropriate, routinely provided treatment for MPM currently available in the UK and Australia, with no treatment withheld. All patients were discussed at a specialist MDT (with SPC representation) with a consensus for a treatment plan. There is usually initial frequent contact with the patients and carers, about symptom management, advice on potential legal compensation and preparation for chemotherapy. All recruiting centres had a dedicated thoracic cancer or mesothelioma specialist nurse as part of the clinical team during the study. The referral of participants in the control group to SPC was at the discretion of the medical team(s) based on clinical need.
Outcomes
Primary aim
The primary aim was to determine if regular early SPC in newly diagnosed MPM patients resulted in improved HRQoL 12 weeks after randomisation, as compared with standard care. HRQoL was measured using the Global Health Status (GHS) subscale of the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire Core 30 (QLQ-C30), with a higher score indicating a better HRQoL. This questionnaire has been validated in patients with MPM24 and used in other recent MPM studies.25 26
Secondary aims
The secondary aims included: participant HRQoL at 24 weeks (using the EORTC QLQ-C30); participant symptoms using the EORTC QLQ LC-13 lung cancer module supplement; participant mood at 12 weeks and 24 weeks and overall survival; and primary caregiver’s HRQoL, mood and satisfaction with care at 12 and 24 weeks, and additionally at 24 weeks following patient death.
Caregiver HRQoL was assessed using the 1-week recall 36-Item Short Form Health Survey (SF-36v2). The FAMCARE-2 questionnaire has sound psychometric properties and measures family/carers satisfaction with end-of-life care.27 Mood was assessed using the 12-item General Health Questionnaire (GHQ-12), a widely used measure for screening for psychiatric morbidity in adults.28 The study visit schedule is presented in the online supplement.
Supplementary file 1
Sample size
With the assumption of a population mean of 55 and a common SD of 22 in GHS/HRQoL for mesothelioma patients,24 we estimated that a sample size of 78 patients in each arm was required to detect a 10-point difference in the mean scores between the two groups, with a power of 90% at a 5% two-sided significance level, assuming an association between baseline and follow-up GHS of R2=0.25. With an estimated 10% dropout before the primary endpoint at 12 weeks, the required sample size was estimated to be 174 participants.
Statistical methods
The primary analysis of the 12-week primary outcome was based on the intention-to-treat approach (ie, all patients analysed according to the group to which they were randomised) using a linear regression model adjusting for baseline (ie, analysis of covariance (ANCOVA)), resulting in an adjusted mean difference in global health status score between randomised groups. We also performed the same linear regression additionally adjusting for the minimisation variables (centre, plan for chemotherapy, ECOG performance status and histological subtype). We hypothesised that some data would be missing at 12 weeks due to early mortality, and quality of life (QoL) may be associated with survival, so analysing QoL on its own may have led to bias. Therefore, we additionally used a joint modelling approach combining linear mixed effects models for repeated measurements and Cox models for censored survival outcomes.29 The model incorporated all follow-up measurements of the outcome (ie, at 4, 8, 12, 16, 20 and 24 weeks) and survival time (with surviving patients censored at their 24-week visit or date of last known contact if they dropped out before the 24-week visit). Covariates of the mixed effects submodel were baseline measurement of the outcome, treatment group, measurement time point and a treatment group–measurement time point interaction.
For all patient-reported secondary outcomes, ANCOVA models were used, as per the analysis of the primary outcome, as described above. Median survival times were obtained from the Kaplan-Meier product-limit estimate of the survivor function. Patients who were alive at the end of the trial were censored at their last known date of contact. A Cox proportional hazards model was used to assess the effect of early SPC compared with standard care on survival with treatment group as the only covariate in the model.
Per-protocol analysis consisted of those randomised participants who had at least one postbaseline GHS score, additionally for those randomised to SPC: completed all scheduled monthly SPC visits within the specified ±7-day window prior to the primary time point. Prespecified subgroup analyses comparing the EORTC C30 GHS at 12 weeks and 24 weeks were performed on the following subgroups: neutrophil/lymphocyte ratio (NLR <5/≥5), International Association for Study of Lung Cancer Mesothelioma radiological stage (1–4),30 country of recruitment (UK/Australia), age at recruitment (<75/≥75 years), baseline ECOG PS (0/1) and nominated carer at recruitment (yes/no). For each subgroup, a linear regression was performed for the GHS score adjusting for the baseline GHS score, treatment group, subgroup and the subgroup–treatment group interaction for week 12 and week 24 separately. Statistical analyses were performed using Stata V.15.1 at the Centre for Statistics in Medicine, University of Oxford.
Results
From April 2014 to October 2016, we assessed 687 potential participants for eligibility, and 174 participants were randomised and included in the intention to treat population (figure 1). At 12 weeks, 157 (90.2%) participants were followed-up, and 135 (77.6%) at 24 weeks. There were 8 withdrawals and 31 deaths during the study period. Baseline characteristics were well balanced between the groups (table 1). The median follow-up (from randomisation to date of last known contact) was 41.1 (IQR 25.1–61.9) weeks.

CONSORT study diagram. CONSORT, Consolidated Standards of Reporting Trials; ECOG, European Cooperative Oncology Group; EORTC, European Organization for Research and Treatment of Cancer; PS, Performance Score; SPC, specialist palliative care.
Baseline characteristics of study participants
In addition, 145 main carers were recruited, 73 to the intervention group and 72 to the control group. At 12 weeks after randomisation, 130 (89.7%) remained in the study, 109 (75.2%) remained at 24 weeks (online supplement figure 1). The characteristics of those participants contributing to the primary outcome at 12 weeks are presented in online supplement table 5; participants without the primary outcome data available where older and had more sarcomatoid containing histology.
Supplementary file 2
Adherence to the intervention
In the intervention arm, 84 (96.6%) participants completed at least one SPC visit before 12 weeks with 68 (78.2%) completing all three visits. Twenty-nine (33.3%) of the intervention group had at least one SPC visit falling outside of the ±7-day window. At 12 weeks after randomisation, 15 (17.2%) participants in the control arm had been referred to and seen by SPC. By week 24, 30 (34.5%) participants in the control arm had been referred to SPC. At 24 weeks after randomisation, 31 (17.8%) participants had died and 93 (53.4%) had died at last point of contact (end of trial) with a median survival of 54.6 (95% CI 46.4 to 72.9) weeks.
Primary outcome
There was no statistically significant between group difference in the mean score of the EORTC QLQ-C30 GHS at 12 weeks after randomisation (table 2).
Participant-reported outcome measures at 12 weeks and 24 weeks
Secondary outcomes
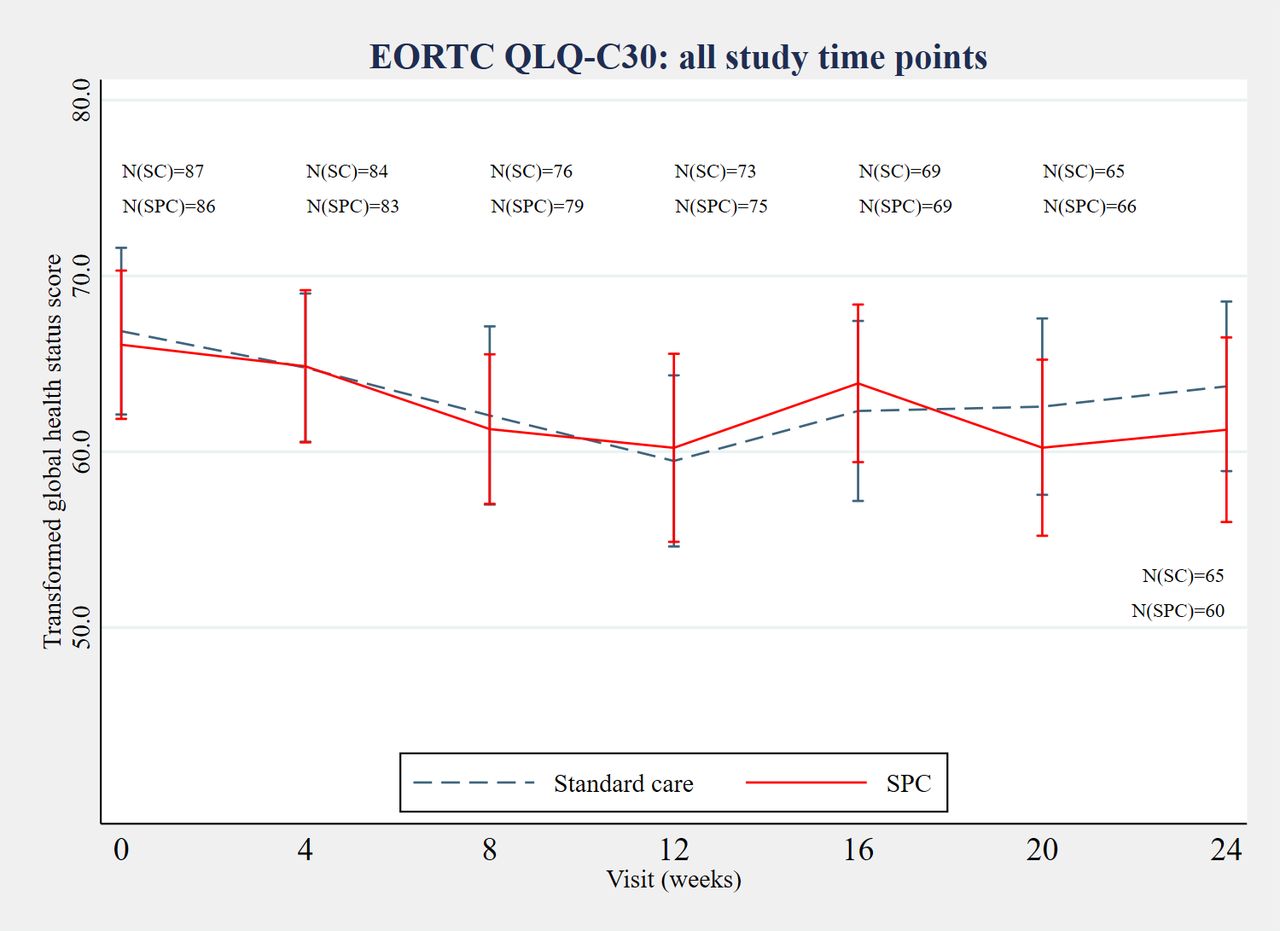
The data for secondary analyses for patients are provided in table 3 and presented in figure 2. The association parameter from the joint model applied to the GHS score and survival data was −0.11 (95% CI −0.16 to −0.06, p<0.01), which implied a negative association between the GHS score and death times (ie, the lower the score, the higher the chance of death). However, results remained consistent with the primary analysis, that is, the treatment effect estimated at each 4-week time point demonstrated no evidence of a significant difference between groups at any time. Symptom burden assessed using the EORTC QLQ LC-13 at 12 weeks after randomisation also had no significant between group differences (see online supplement).
Carer reported outcome measures at 12 weeks and 24 weeks after randomisation and 24 weeks postbereavement

{kind=link}
{kind=link}
Mean±95% CI of the mean global health status score (raw values) at all time points by treatment group. N(SC)=no. of available GHS scores in the standard care arm; N(SPC)=no. of available GHS scores in the specialist palliative care (SPC) arm. EORTC, European Organization for Research and Treatment of Cancer; QLQ-C30, Quality of Life Questionnaire Core 30.
Survival
Thirty (17.2%) participants died within 24 weeks of randomisation. There was no mortality difference between the groups with a Cox proportional hazards regression analysis demonstrating an HR of 1.1 (95% CI 0.6 to 2.3), p=0.74 and log rank test (χ2 (1)=0.11; p=0.74). Throughout the duration of the study, 93 (53.4%) participants died. Again, there was no mortality difference between the groups with a Cox proportional hazards regression HR of 1.2 (95% CI 0.8 to 1.7), p=0.50 and log rank test (χ2 (1)=0.46; p=0.50: table 2 and online supplement figure 2).
Supplementary file 3
Outcomes for carers
Data for the carer reported outcomes are presented in table 3. There was no evidence of a statistically significant difference in the physical or mental component measures of the SF-36 between treatment groups at any time point. The GHQ-12 score differed between the treatment groups at week 24, favouring a positive outcome on the intervention arm. FAMCARE-2 scores were significantly higher (better) in the intervention arm at week 12 and week 24; p values derived using non-parametric comparison were in agreement with this conclusion. At 24-week postbereavement, the mean difference adjusted for baseline still favoured the intervention arm, although numbers were small in each arm.
Protocol deviations and harms
One participant was randomised to the intervention arm in error as they were ineligible and were withdrawn. One participant in the intervention arm was unable to attend the SPC clinic appointments. Nine SAEs were reported during the study in five patients; all SAEs related to clinical decline and none were related to the intervention.
Prespecified subgroup analyses
There were no statistically significant between-group differences in the EORTC C30 GHS observed within any of the prespecified subgroups (see online online supplement).
Discussion
The RESPECT-Meso trial demonstrates that for patients with MPM with good performance status, routine referral to SPC soon after diagnosis does not confer any benefit in HRQoL and/or mood. This is the largest randomised controlled trial to examine this question in patients with mesothelioma. This study suggests strongly that current standard palliative management in the UK and Australia is adequately meeting the holistic needs of patients early in the disease trajectory of mesothelioma.
We have considered if the study design or conduct may have led to a type II error, missing a real effect of the intervention. Dropout (from lost to follow-up, withdrawal and death) before the primary outcome at 12 weeks after randomisation was as anticipated at 17 (9.8%), and data completeness for the primary outcome was good; thus, it is unlikely this study was underpowered. As anticipated in this pragmatic study, there was some dilution of effect from the intervention with 19 (21.8%) of the intervention group not completing all SPC visits and 15 (17.2%) of the standard care arm having received SPC review before the 12-week outcome. The primary outcome measure is a well-validated and accepted measure for mesothelioma HRQoL, and our baseline estimates of HRQoL were similar to two recent large randomised controlled trials in MPM25 26 suggesting validity of our findings. Finally, we have performed a post hoc analysis of those who died within 24 weeks of randomisation versus those alive at 24 weeks; this demonstrated a lower baseline score in those who died but no significantbetween group difference (mean GHS QLQ-C30 score (SD) early SPC vs standard care: 38.9 (30.6) vs 46.4 (21.4); p=0.25). Overall, we consider that the study result is a true negative.
The results of this study appear to be different to other similar reports examining early SPC in differing cancer types.13–20 Aside from differing study designs, the RESPECT-Meso study has examined a different disease in a different healthcare system compared with other studies. It is also possible that our study has recruited participants too early in the disease trajectory for the intervention to be useful (although the post hoc analysis above does not support this supposition). The inclusion criteria of the study included the requirement for an ECOG performance status of 0 or 1, which means the study recruited a relatively well population. The inclusion of participants with a performance score of 2 would have led to a much higher drop out (by death) before the primary outcome and the potential for the study being underpowered. Despite the requirement for a good performance status, at the time of randomisation, 77.0% of participants reported dyspnoea and 57.4% reported chest pain. At least one cycle of chemotherapy was completed in 59.2% of participants, suggesting that approximately one-third of the study population had contraindications and/or comorbidities precluding systemic cytotoxic therapy. The median survival of the whole study population was 54.6 weeks, suggesting that despite a good performance status at recruitment, many participants were symptomatic at baseline and deteriorated quickly.
The results for main carers are similar as for the participants. There is no demonstrable difference in QoL and an isolated signal of a lower anxiety/depression score at 24 weeks after randomisation, favouring the intervention arm. There is, however, a clear indicator of an increased overall satisfaction with care for the carers in the early regular SPC group. From the FAMCARE questionnaire, there was increased reported satisfaction with ‘SPC’s attention to patient’s symptoms’, ‘emotional support to family members’, ‘how effectively SPC manages the patient’s symptoms’, the ‘response to changes in symptoms’ and ‘emotional support provided to the patient by the SPC team’. SPC regards the patient as the centre of a family group, so that the assessment and management of carers’ needs is recognised as integral to patient care; this may in part explain the observed increased carer satisfaction.
Rather than regular early SPC having little effect on HRQoL or mood, it is possible that the current provision of clinical care in the control arm is providing a good level of holistic cancer care. All recruiting centres in this study had senior specialist thoracic cancer and chemotherapy nurses. It is plausible therefore that in the early months after diagnosis, the level of physical, emotional and spiritual care provided to most patients with mesothelioma in these treating centres is meeting patients’ needs; however, this study has not specifically tested this supposition. SPC should, however, continue to be involved when patients’ pain, symptoms, psychological/spiritual or advance care planning needs are no longer met by their respiratory or oncological teams and that 34.5% of patients in the control arm had been referred to SPC by week 24 appears to confirm this. Future studies might include specific pain and symptom outcome measures and/or examine which patients, what levels and when in their disease trajectory patients will most benefit from referral to SPC. Before understanding further the possible role(s) of early SPC integrated into oncological care, it may be useful to better understand and delineate the current aspects of general palliative care already being provided as standard care in many treating centres. In addition, the crucial aspect of direct and indirect healthcare-associated costs for providers and individuals must be analysed when assessing the utility of a new intervention. Given the results of the primary and secondary outcomes in this study, the prespecified formal healthcare economic evaluation was not performed as originally stated in the protocol.21
Potential limitations of this study include a high failure rate of screening (predominantly from refusal and not fitting eligibility criteria). Participants who had already started systemic chemotherapy or who were postsurgery where excluded as they were likely to have very different health needs and quality of life. The exclusion of ECOG PS 2 participants potentially reduces the generalisability of the study, although in the UK and WA, between 67% and 80% of MPM patients present with an ECOG PS of 0-1.5 31 Furthermore, the uniformity of the SPC intervention provided across multiple sites may have varied after the initial standardised baseline assessment, but the nature of palliative care is inherently bespoke to the patients’ (and families’) needs. Finally, while this was a multicentre study, 20.7% of recruitment was from a tertiary cancer centre for WA; however, prespecified subgroup analysis did not demonstrate any difference in HRQoL measurements between the Australian and UK sites, and the provision of both standard and SPC care is similar between the UK and Australia.
In conclusion, our data do not support the routine early referral of good performance status patients with newly diagnosed MAPM to SPC services, provided there is specialist follow-up and good access to SPC when required. The current practice of referral to SPC based on clinical judgement of the treating physician and MDT from symptom burden and perceived need should continue. The perceived increased carer satisfaction with SPC teams is noteworthy, but this finding alone is unlikely to influence widespread provision of healthcare services in this context.
References
Footnotes
Contributors FB: study conception, study design, data collection, analysis, interpretation and writing. SG: study design and data collection. IL: study design, data collection, analysis, interpretation and literature search. LM: study design, study conduct and data collection. CF: study design and conduct. CQ and SG: statistical analysis. LC, NH, SK, BY, DC, PC, EF, JW, CP, AB, CM, AT and LS: recruitment and data collection. NM: study design, data collection, analysis and interpretation. KF: study design, analysis and interpretation. AC: study design, data collection, analysis, interpretation and writing.
Funding British Lung Foundation and Australian Communities Grant.
Disclaimer The British Lung Foundation and the Australian Communities Foundation had no role in the study design, data collection, data analysis, data interpretation or writing of the report.
Competing interests None declared.
Patient consent Not required.
Ethics approval Ethical approval for this study was granted by the National Research Ethics Service Committee, London (Hampstead, UK), reference 12/LO/0078.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Collaborators RESPECT-Meso investigators: Andrew Bateman, Melissa Dobson, Richard Hopgood, Samuel King, Angela Morgan, Stephen Morris, Alice Mortlock, Neal Navani, Anna Nowak, Michael Peake, Mark Roberts, Lynne Squibb, Paul Taylor.