Article Text

Abstract
It is increasingly recognised that the airway circulation plays an important role in airway diseases, either through a change in blood flow or through microvascular leakage. Most of the information available regarding the anatomy and physiology of bronchial blood flow and its regulation has necessarily derived from animal studies. However, there have recently been important advances in understanding airway blood flow in airway disease in humans through the development of non-invasive methods and in the quantification of microvascular leakage using plasma markers. These studies have shown that bronchial blood flow is increased in patients with asthma but not in those with chronic obstructive pulmonary disease, confirming previous pathology investigations. Changes in bronchial blood flow may in part reflect the generation of new vascular vessels, a process known as “angiogenesis” which is caused by airway inflammation. Angiogenesis and the resulting plasma leak affect airway physiology, drug clearance and its bioavailability. This review discusses the anatomy, physiology and regulation of bronchial blood flow in the normal and diseased lung, In addition, it analyses the effect of current medical treatment and discusses the potential use of new anti-angiogenesis medications. The development of non-invasive assessment of bronchial blood flow and the study of angiogenesis have provided a tool to investigate airway physiology in vivo; these advances will contribute to a better understanding of inflammatory airway diseases as well as the implication of these findings to management.
Statistics from Altmetric.com
ANATOMY OF THE BRONCHIAL CIRCULATION
The pulmonary circulation is a high-capacitance low-resistance network of vessels which accommodates the entire venous return of the body, whereas the bronchial circulation is a high-resistance low-capacitance circulation which receives only 1–2% of the total cardiac output in normal subjects.1
Bronchial arteries
The bronchial circulation is part of the systemic circulation. Normally there are two main bronchial arteries, at least one of which originates from the aorta and the other from the intercostal arteries or, very rarely, from the internal mammary and the coronary arteries. The bronchial arteries join the main bronchi at the hila where they divide into two or three branches that wind around and supply the wall of the bronchus. These arteries divide into smaller vessels that anastomose and form a peribronchial arterial bronchial plexus (fig 1). They also give rise to small arterioles that penetrate the muscular layer to reach the bronchial mucosa where they form the submucosal plexus. The bronchial arteries also supply the visceral pleura.

Schematic representation of the bronchial circulation illustrating the adventitial and submucosal plexuses. Reproduced with permission from Deffebach et al.1
Bronchopulmonary circulation
About two-thirds of the bronchial capillary blood is thought to drain into anastomoses or communicating vessels that empty into the pulmonary veins forming the so-called “bronchopulmonary circulation”.
Bronchial veins
The bronchial submucosal and adventitial venules drain into the bronchial veins which drain into the azygos and hemiazygos veins.2 However, the intrapulmonary bronchial circulation mostly drains directly into the pulmonary circulation through bronchopulmonary anastomoses.
PHYSIOLOGY OF THE BRONCHIAL CIRCULATION
Most studies on the physiology of bronchial blood flow have been carried out on animals; this is a major limitation and unfortunately we can only assume that there are similarities with humans.
Oxygenation
Contrary to what has been shown for the pulmonary circulation, systemic hypoxaemia increases both anastomotic and total bronchial blood flow.1
Inhaled air temperature
The inhalation of cold air caused an immediate increase of the bronchial blood flow in an animal study.3 However, data in humans are scarce and unreliable.
Positive end expiratory pressure
The alveolar pressure and the lung volume significantly affect the bronchial blood flow with higher airway pressures decreasing blood flow.1 This may be due to mechanical compression of the blood vessels.
Pulmonary and systemic artery pressure
There is an inverse relationship between pulmonary artery pressure and the pressure in the left atrium and bronchial blood flow. On the contrary, elevated systemic blood pressure is associated with an increase in bronchial blood flow.1
Neurological regulation
The bronchial arteries have α- and β-adrenergic receptors and it is known that adrenaline, which has α-agonist effects, reduces total bronchial flow as it does in other systemic vascular beds.4
Even though the action of the parasympathetic system on the bronchial blood flow is controversial, there are indications that the stimulation of the vagus increases total bronchial flow.1
Animal studies show that several peptides released from airway nerves, such as vasoactive intestinal peptide from cholinergic nerves and substance P and calcitonin gene-related peptide, are potent bronchial vasodilators and may also increase microvascular leak.5
Effect of mediators
Histamine
Histamine causes vasoconstriction of the pulmonary circulation and vasodilation of the systemic vascular bed.6 In the bronchial circulation, histamine inhalation causes an increase in blood flow which is mediated via H2-receptors.7
Prostaglandins (PGs)
PGF2α has been shown to increase bronchial blood flow.8 Cyclo-oxygenase inhibitors reduce the increase in bronchial blood flow resulting from hypoxia.9
Nitric oxide
Sasaki et al showed that the administration of NG-nitro-L-arginine (L-NNA), a competitive inhibitor of NO synthase, decreased bronchial blood flow and inhibited acetylcholine-induced vasodilation.10 The administration of exogenous inhaled NO resulted in a dose- dependent increase in bronchial blood flow and a decrease in vascular resistance in sheep.11
FUNCTION OF THE BRONCHIAL CIRCULATION
Airway nutrition
The bronchial circulation provides nourishment to the airways. However, an acute obstruction of the main bronchial artery does not cause ischaemic changes; this may be due to a retrograde blood flow through the bronchopulmonary anastomoses.1
Airway lining fluid and local defences
The bronchial circulation is responsible for the formation of the epithelial lining fluid which plays a role in the local defences against inhaled irritations and substances. A functional bronchial circulation is required for the maintenance of normal mucociliary transport.1
Clearance of small particles
Interrupting bronchial artery perfusion in sheep resulted both in increased retention of a soluble tracer at the site of deposition and attenuation of the uptake of 99mTc-DTPA into the bronchial circulation.12 This indicates that bronchial blood flow is essential for the absorption and distribution of the particles and their clearance.
Airway temperature and air conditioning
The airway mucosa responds to the cooling of the airways following the inhalation of cold air by increasing bronchial blood flow and therefore improving heat and moisture transfer.1 This is a defence mechanism to protect the mucosa from “cold friction burns”. When the inhaled air temperature is elevated and dry, the respiratory system conserves the fluids by exhalation of practically dry air, losing only one-tenth of the water previously used to humidify the air inhaled.
MEASUREMENT OF BRONCHIAL BLOOD FLOW
Several techniques have been developed to measure bronchial blood flow invasively in animals. Bronchial blood flow has recently been measured non-invasively in humans and has been suggested as a marker of airway inflammation in asthma and chronic obstructive pulmonary disease (COPD).13 14
Invasive measurement of bronchial blood flow
The total bronchial blood flow can be measured by dissecting and isolating the bronchial vessels separately. Less invasive methods are dye video densitometry and the use of radioactive microspheres where blood flow is estimated from the radioactivity found in the excised lung.1
Non-invasive measurement of blood flow
Dimethylether method
The lung uptake of soluble inert gases is used to measure pulmonary blood flow as an index of cardiac output. The same principle was applied to measure the blood flow of the airways15 making use of dimethylether (DME), a soluble gas with a high affinity for haemoglobin. This method is based on the assumption that the uptake of an inert soluble gas in a tissue with capillaries and active flow of blood is determined by the volume of the tissue and by the blood flow.16 The same method was later modified and validated indirectly with microspheres in sheep.17
The DME method requires multiple breath holds followed by exhalations into a spirometer. The concentrations of DME, nitrogen and helium are measured at the airway opening with a mass spectrometer.18 This method has not been used in laboratories other than the one where it was first developed. This may in part be due to its complexity; eight breath hold manoeuvres are required for a single measurement. To address these limitations, the same group that developed the method originally has recently simplified the technique by reducing the number of breath holds to two.19
Acetylene method
Acetylene, like DME, has a very high affinity for haemoglobin but is less explosive.20 21 Subjects inhale a gas mixture which includes acetylene 5% and exhale into a mass spectrometer. The area under the curve (AUC) of the acetylene tracing is inversely proportional to bronchial blood flow, so multiple breath holds are not required.
The effect of vasoactive compounds such as the vasoconstriction induced by corticosteroids,14 adrenaline22 and L-NAME22 and the vasodilation following the inhalation of β2-agonists13 14 22 and nitric oxide (NO)22 support the hypothesis that the method effectively measures bronchial blood flow. The same method has been developed independently by two groups.
ANGIOGENESIS IN AIRWAY DISEASE
Inflammation is associated with the generation of new blood vessels (angiogenesis).
Role of VEGF and other angiogenic mediators
Angiogenesis has been extensively studied and the vascular endothelial growth factor (VEGF) has received increasing interest because of its role, not only in angiogenesis, but also in the regulation of vascular permeability and lung development. The VEGF family signals through three different receptors. Even though VEGF-A also binds to VEGFR-1, VEGFR-2 has been shown to account for most of its effects.23 Besides being a vascular endothelial mitogen for arteries, veins and lymphatics, VEGF promotes endothelial survival by inducing the expression of the anti-apoptotic proteins BCL-2 and A1.24 VEGF also regulates capillary permeability by inducing the fenestration in endothelial cells.25
Hypoxia26 and cytokines such as interleukin(IL)-1α and IL6 increase the expression of VEGF, but IL10 and IL13 downregulate its expression. Lung disorders characterised by inflammation and/or hypoxia such asthma and COPD therefore show pathological levels of VEGF.
Patients with asthma have increased concentrations of VEGF in induced sputum27 and BAL fluid28 which are negatively correlated with airway obstruction and positively correlated with eosinophilic inflammation and vascular permeability.29
The role of VEGF in COPD is unclear. The concentration of VEGF may be reduced in the induced sputum of patients with emphysema but raised in subjects with chronic bronchitis.30
VEGF works in concert with other growth factors including angiopoietins. Four members of the angiopoietin family are now known and angiopoietin-1 (Ang-1) has received a lot of interest and promotes circumferential growth.31
Even though VEGF is considered the main angiogenic factor, other molecules have been investigated including fibroblast growth factor (FGF),29 angiogenin,29 tumour necrosis factor-α (TNFα)32 and chemokines such as IL8 and eotaxin, all of which may have a role in lung angiogenesis.
Angiogenesis
The term “angiogenesis” defines the expansion of the primitive capillary vascular bed into a more complex network.33 Angiogenesis starts with vasodilation, which requires NO. Vascular permeability increases in response to VEGF, allowing extravasation of plasma proteins that lay down the provisional scaffolding for migrating endothelial cells. Contrary to the action of VEGF, Ang-1 inhibits vascular permeability without affecting vascular morphology. Endothelial cells need to loosen interendothelial cell contacts to emigrate from their resident sites. Ang-2, an inhibitor of endothelial-specific tyrosine kinase (Tie-2) signalling, may be involved in detaching smooth muscle cells and loosening the matrix. Once the intracellular contacts have been loosened, VEGF initiates endothelial network organisation and Ang-1 stabilises the newly formed vessels.
BRONCHIAL VESSELS IN AIRWAY DISEASE
Asthma
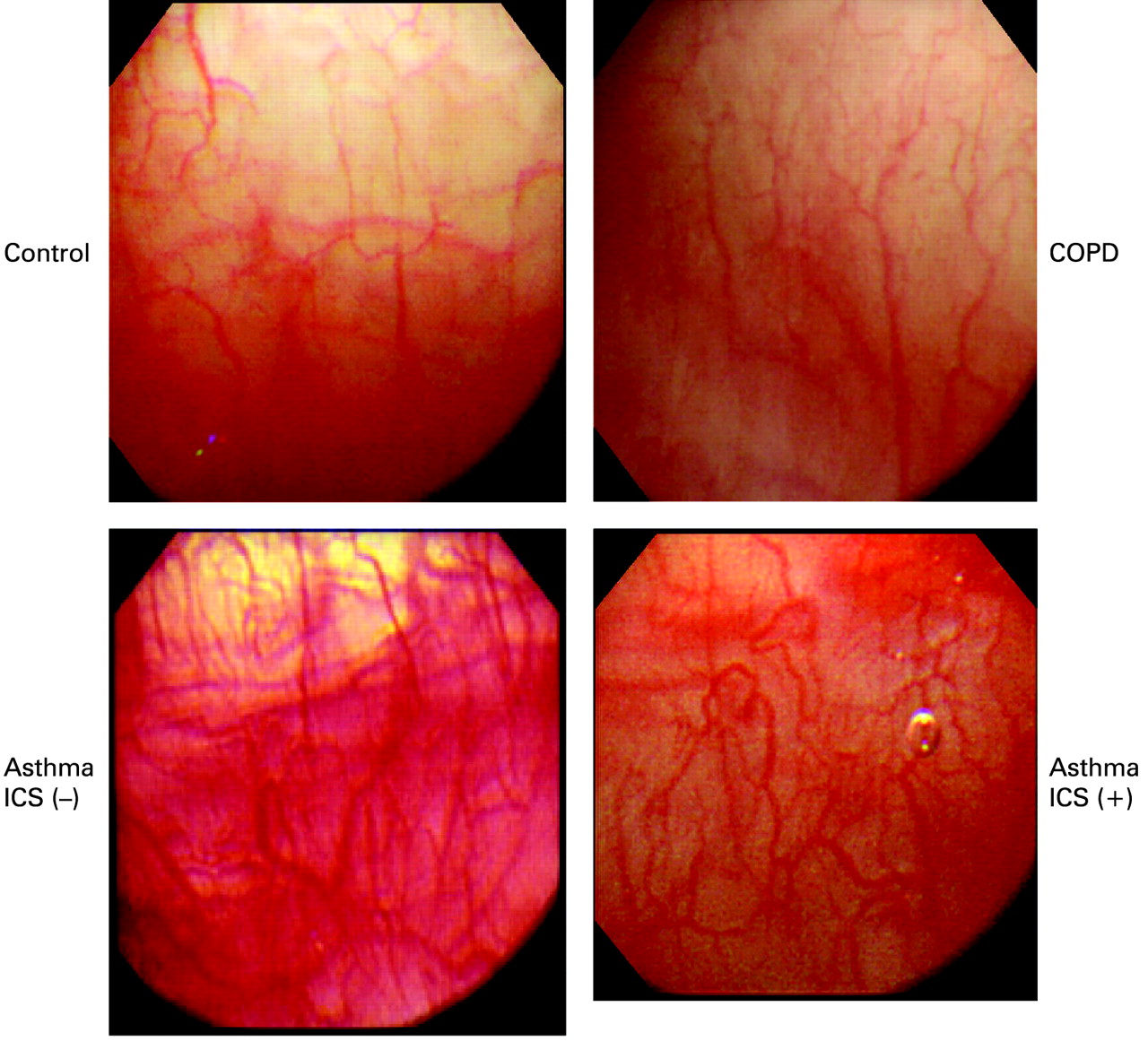
The bronchial submucosa of patients with asthma has an increased number of vessels, occupying a larger percentage of area than in normal subjects29 34—not only in the large but also in the medium and small airways.35 These changes are also present in patients with mild and moderate disease36 and in children (fig 2).37 The use of a high magnification bronchovideoscope has recently allowed direct visualisation of the bronchial vessels,38 confirming the presence of an increased number of vessels in subjects with asthma (fig 3).

Bronchial biopsy sections from (A) and (C) a child with asthma and (B) and (D) a control child showing increased number of subepithelial vessels (A, brown) and eosinophils (C, red) in the child with asthma. Arrows indicate epithelial loss (A and C) whereas arrowheads indicate reticular basement membrane thickening (A). Immunostaining with monoclonal antibody anti-CD31 (A and B) and anti-EG2 (C and D). Original magnification ×630. Reproduced with permission from Barbato et al.37

Bronchovideoscopic images of the lower trachea of a control subject, a patient with chronic obstructive pulmonary disease (COPD), a steroid-naive patient with newly diagnosed stable asthma (ICS (−)) and a patient who has had stable asthma for more than 5 years treated with inhaled corticosteroid (ICS (+)). Airway vascularity is increased in the patients with asthma compared with the control subject and the patient with COPD. Reproduced with permission from Tanaka et al.38
Airway vascular remodelling and inflammation may be responsible for increased bronchial blood flow39 and exhaled breath temperature gradients in patients with asthma.40 The measurement of bronchial blood flow may indirectly reflect airway inflammation and angiogenesis. Besides being increased in asthma as expected,14 39 bronchial blood flow is also correlated with the concentrations of exhaled NO,14 a potent vasodilator and a marker of inflammation. Subjects with asthma also show increased heat exchange and airway temperature gradients (Δe°T) which correlate with bronchial blood flow and exhaled NO. Increased levels of NO may lead to vasodilation and increased bronchial blood flow, as shown by the correlation between exhaled NO and Δe°T (fig 4).
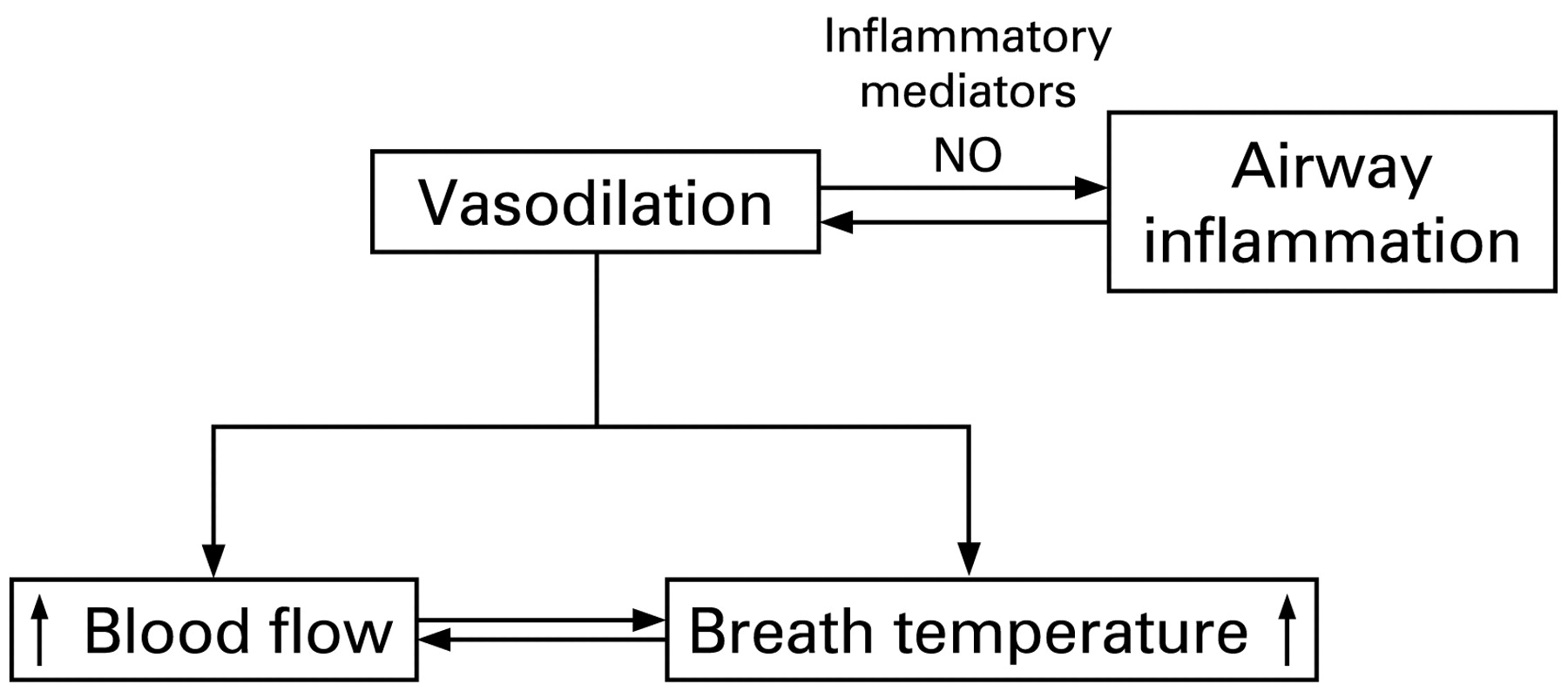
Schematic representation of the interaction between inflammation, bronchial blood flow and exhaled breath temperature.
COPD
Early histological studies showed decreased bronchial vascularity in patients with COPD.41 42 More recently, some authors have confirmed that the number of vessels in the airways of these patients is not significantly increased.35 A bronchovideoscopic study38 and the measurement of bronchial blood flow13 also support the hypothesis that vascular remodelling is not a feature of COPD airways (fig 3). However, at least two studies have shown increased bronchial vascularity.43 44 This discrepancy may be due to the recruitment of more severe and elderly patients in the last two studies.
In keeping with the studies showing increased vascularity of the airways, VEGF levels are increased in the induced sputum of patients with chronic bronchitis and the expression of VEGF in central and peripheral airways of ex-smokers with COPD is higher than in a normal control group.45 VEGF expression is correlated with airflow obstruction and inflammatory cytokines such IL8 and TNFα and has been suggested as a marker of inflammation.46
However, the role of VEGF in the pathogenesis of COPD is twofold; it may be detrimental in the bronchi where it correlates with obstruction and protective in the alveoli where lower levels of VEGF correlate with alveolar destruction.30 47 The decrease in VEGF in the lower respiratory tract48 may lead to the development of emphysema. This hypothesis is also supported by in vitro and in vivo studies showing that reduced VEGF levels or blockade of VEGF receptors could play a role in the pathogenesis of emphysema.49
Bronchiectasis
Liebow50 in 1949 showed enlargement of the bronchial arteries and increased anastomoses with the pulmonary circulation. A similar pattern was described in tuberculosis where the affected areas present increased bronchial blood flow and dilation and proliferation of the bronchial capillaries51 and bronchopulmonary anastomoses. These can form small pedunculated aneurysms found inside the tuberculous cavities, as described originally by Rasmussen, the rupture of which results in haemoptysis.
AIRWAY MICROVASCULAR LEAKAGE
Mechanisms
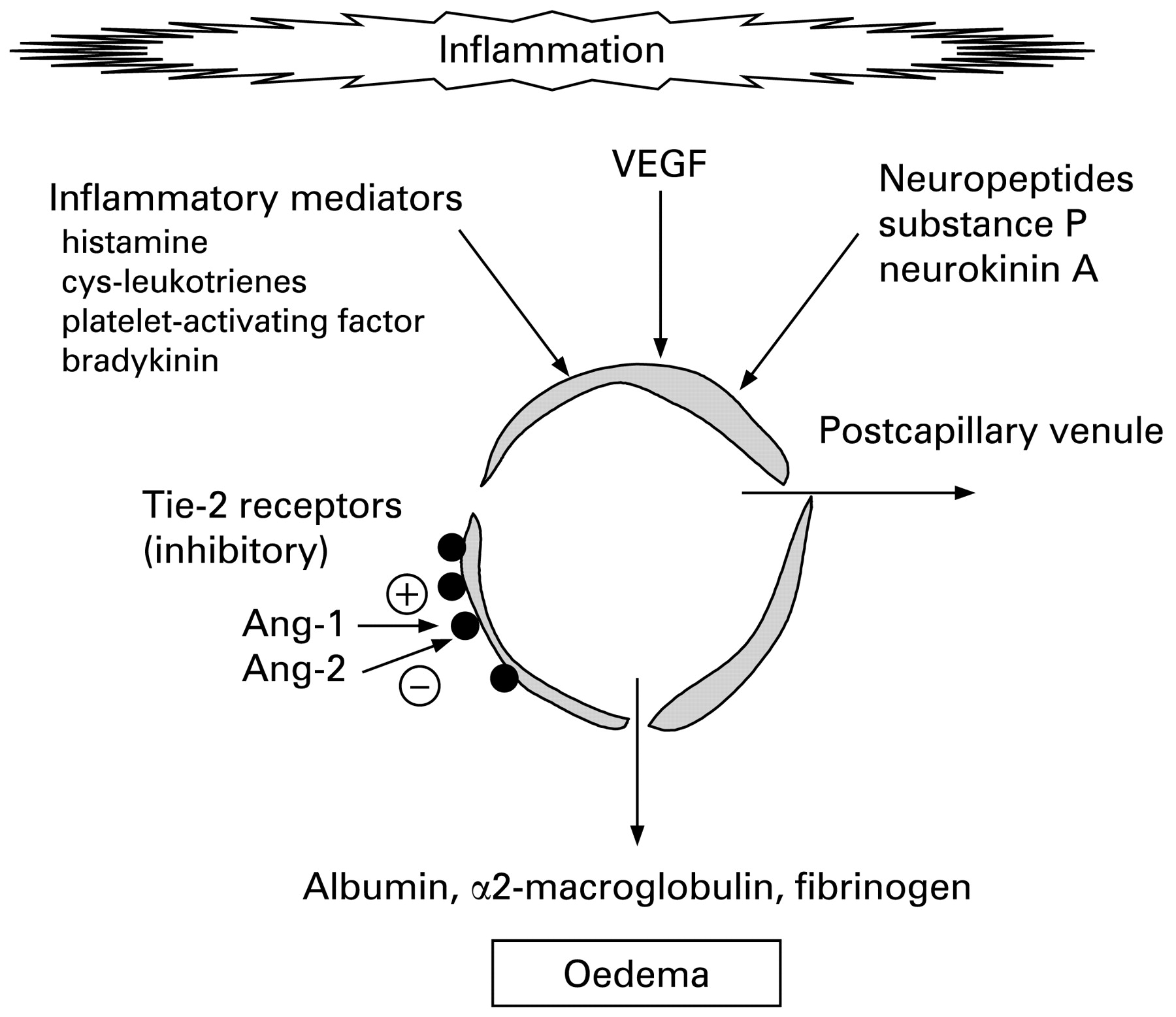
VEGF stimulates the formation of new vessels with increased permeability52 which cause mucosal oedema and reduce airway diameter (fig 5). Two endothelial-specific tyrosine kinase (Tie) receptors have been described, Tie-1 and Tie-2.53 Tie-2 is highly expressed in the lung. Both Ang-1 and Ang-2 bind to Tie-2 receptors with equal affinity, but they have opposite effects. Ang-1 reduces the permeability of the vessels31 whereas Ang-2, which is a competitive antagonist of Ang-1 on Tie-2 receptors, increases vascular permeability.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Schematic representation of airway microvascular leakage. Inflammatory cytokines, vascular endothelial growth factor (VEGF) and neuropetides cause vascular leakage. Angiopoietin-1 (Ang-1) and angiopoietin-2 (Ang-2) bind to endothelial-specific tyrosine kinase-2 (Tie-2) receptors with opposite effects. The measurement of albumin, α2-macroglobulin and fibrinogen in the bronchoalveolar lavage fluid provides an estimate of the leakage.
As well as redness due to increased blood flow (“rubor”), tissue swelling (“tumour”) is also a cardinal sign of inflammation. Microvascular leakage and plasma exudation are seen in both asthma and COPD as signs of airway inflammation, and many mediators may produce this effect by relaxing post-capillary venular endothelial cells, including mediators of inflammation such as histamine, cysteinyl-leukotrienes, bradykinin, platelet-activating factor and adenosine as well as neuropeptides such as substance P. Bronchial vasodilators increase plasma exudation by increasing the blood flow to leaky vessels and many mediators act as both vasodilators and induce leakage. Most of our knowledge of microvascular leakage is from studies in animals using Evans blue dye which binds to plasma proteins, but these methods are not applicable in humans.54 However, plasma exudation can be measured by assaying plasma proteins such as albumin. α2-Macroglobulin and fibrinogen in induced sputum or BAL fluid show an increased sputum/BAL concentration compared with plasma.
Measurement
The permeability of the blood-airway lumen barrier can be measured by analysing albumin and α2-macroglobulin in BAL fluid and paired serum samples.55 However, because the epithelial lining fluid (ELF) may present different degrees of dilution during lavage, urea is measured as a marker of dilution.56
The vascular permeability has also been assessed by measuring the ratio of albumin concentrations in induced sputum and serum.57 58
Asthma
In patients with stable asthma there is an increase in plasma exudation into the airways which correlates with bronchial hyperreactivity to histamine.59 VEGF, Ang-1 and Ang-2 levels in induced sputum from patients with asthma are higher than those from normal control subjects and there is an inverse correlation between Ang-1 and the airway vascular permeability index. In contrast, Ang-2 is positively correlated with airway vascular permeability.57
COPD
In patients with COPD there in an increase in the sputum Ang-2 level, particularly during infective exacerbations. The increased concentrations of VEGF in the airways of patients with a preponderant bronchitis60 may increase the permeability of the bronchial vasculature and facilitate oedema. This may explain the correlation between VEGF sputum levels and the degree of airflow obstruction.46
EFFECT OF DRUGS
β2-Adrenoceptor agonists
A placebo-controlled study showed a significant decrease in the number of vessels/mm2 in the lamina propria of patients with asthma following 3 months of treatment with salmeterol.61 This may have been caused by reduced levels of the angiogenic cytokine62 IL8 following salmeterol treatment.63
The long-term effect of β2 agonists on the bronchial vasculature of patients with COPD has not yet been investigated, but their acute effect on bronchial blood flow (QAW) is known. Like temperature gradients (Δe°T),14 QAW is also increased in steroid-naïve patients with COPD after inhalation of salbutamol, a known bronchial vasodilator.39 This differs from the findings in asthma where inhalation of salbutamol does not affect Δe°T or QAW,14 probably because in asthma the vessels are already maximally dilated by inflammatory mediators. The finding of a lower QAW increase after β2 agonists in patients with COPD than in normal subjects supports the hypothesis that steroid-naïve patients with COPD have blunted vasoreactivity.64
Besides having an effect on bronchial vascularity, β2 adrenergic agonists may attenuate vascular leakage induced by histamine,65 bradykinin66 and the platelet-activating factor.67
Corticosteroids
Inhaled corticosteroids (ICS) reduce airway wall vascularity in patients with asthma.68 69 In addition, there are indications that higher doses of ICS may reverse the increased airway vascularity by reducing the expression of VEGF and angiogenic sprouts.70 This effect of ICS may be mediated by a reduced production of VEGF in structural and inflammatory cells.71
In two cross-sectional studies, Δe°T and Qaw were similar in corticosteroid-treated and untreated patients with asthma14 and COPD,13, despite the efficacy of steroids in reducing bronchial blood flow.20 One hypothesis is that the vasoconstrictive action of ICS may have been balanced by β2 agonist-induced vasodilation.
In contrast to the effect of chronic treatment with ICS, the acute inhalation of budesonide in patients with asthma causes a significant temporary reduction in Qaw which returns to baseline 1 h after inhalation.14 39 ICS can potentiate the vasoconstrictor actions of norepinephrine and angiotensin II by upregulating their vascular receptors.72 Furthermore, corticosteroids may inhibit the synthesis of NO,73 thus causing vasoconstriction. In addition to these mechanisms of action, corticosteroids may also have a very rapid action (<5 min) by inhibiting norepinephrine uptake in bronchial blood vessels.74
In contrast to asthma, the acute inhalation of budesonide is ineffective in lowering Qaw in patients with COPD.13 The insensitivity of the bronchial circulation of patients with COPD to the inhalation of salbutamol and budesonide is confirmation that this group of patients has reduced vascular reactivity.
Angiogenesis inhibitors
Several inhibitors of angiogenesis have been studied in vitro and some have shown some promising clinical results in lung cancer, but these compounds have not yet been investigated in chronic lung disease. The therapeutic application of vascular growth factors may be promising. Ang-1 has been used to prevent or repair damaged and leaky vessels in diseases such as diabetic retinopathy, acute macular degeneration, ischaemia/reperfusion injury or in inflammation. The discovery of the molecular factors that regulate vessel formation may provide a number of new medications.
VEGF inhibitors
Different strategies have been devised to inhibit VEGF function. The injection of monoclonal VEGF antibodies into nude mice suppressed tumour growth and weight up to 96%,75 and a recombinant humanised monoclonal antibody to VEGF (bevacizumab) has been shown to inhibit the growth of a variety of human cancer cell lines.76 The VEGF system can also be targeted through the inhibition of the VEGF receptor (VEGFR) using monoclonal antibodies or specific tyrosine kinase inhibitors.76
Inhibitors of the Tie-angiopoietin system
No ligand has so far been found for the Tie-1 receptor, whereas the angiopoietin family are the natural ligand for Tie-2. The activation of Tie-2 by Ang-1 may be responsible for the assembly of the non-endothelial cells of the vessels, including perycites and smooth muscle cells.77 On the contrary, Ang-2 binds to the receptor Tie-2 without activating it and may therefore antagonise the action of Ang-1. The injection of the extravascular domain of the Tie-2 receptor has been shown to reduce tumour growth by more than 75% in mice.78
THERAPEUTIC IMPLICATIONS AND DIRECTIONS FOR FUTURE RESEARCH
Even though our knowledge of the bronchial vasculature—particularly in asthma—has been significantly improved in the last few years, the bronchial vessels in chronic inflammatory diseases such as COPD, interstitial lung disease and cystic fibrosis have not been sufficiently investigated. The lack of studies in these diseases is disappointing in view of the possible therapeutic implications that anti-angiogenic molecules may have. The role of the bronchial circulation in the absorption, distribution and action of medications is also unexplored, as is the action of anti-leukotrienes and theophylline.
The non-invasive measurement of bronchial blood flow has provided insights into the pathophysiology of the bronchial vasculature in airway disease, and has allowed a better understanding of the acute and chronic effect of medications. A clearer understanding of angiogenesis and of its role in diseases has led to the development of molecules with anti-angiogenic properties which may be of benefit in the treatment of cancer. The development of more selective medications with fewer side effects may also prove beneficial for patients with chronic lung disease.
REFERENCES
Footnotes
Competing interests: None.