Article Text

Abstract
Background: Very few population based results have been presented for survival after resection for lung cancer. The purpose of this study was to present long term survival after resection and to quantify prognostic factors for survival.
Methods: All lung cancer patients diagnosed in Norway in 1993–2002 were reported to the Cancer Registry of Norway (n = 19 582). A total of 3211 patients underwent surgical resection and were included for analysis. Supplementary information from hospitals (including co-morbidity data) was collected for patients diagnosed in 1993–8. Five year observed and relative survival was analysed for patients diagnosed and operated in 1993–9. Factors believed to influence survival were analysed by a Cox proportional hazard regression model.
Results: Five year relative survival in the period 1993–9 was 46.4% (n = 2144): 58.4% for stage I disease (n = 1375), 28.4% for stage II (n = 532), 15.1% for IIIa (n = 133), 24.1% for IIIb (n = 63), and 21.1% for stage IV disease (n = 41). The high survival in stage IIIb and IV was due to the contribution of multiple tumours. Cox regression analysis identified male sex, higher age, procedures other than upper and middle lobectomy, histologies such as adenocarcinoma and large cell carcinoma, surgery on the right side, infiltration of resection margins, and larger tumour size as non-favourable prognostic factors.
Conclusions: Survival was favourable for resected patients in a population based group including subgroups such as elderly patients, those with advanced stage, small cell lung cancer, tumours with nodal invasion, and patients with multiple tumours. These results question the validity of the current TNM system for lung cancer with regard to tumour size and categorization of multiple tumours.
- lung cancer
- survival
Statistics from Altmetric.com
The increasing incidence and poor survival of patients with lung cancer, including women and young people, necessitates a reappraisal of the current strategy for diagnosis and treatment.1–,3 Patients are often in an advanced stage of disease and resection rates are therefore low. Improvements of surgical outcomes have been sparse, but evidence of lower postoperative mortality and slightly increased survival has been reported.4,5 Previous reports often originate from single institutions, and there are few population based reports on survival, especially relative survival.6,7,8,9,10
The population based cancer registries create a unique platform for studies of risk factors for survival. Traditionally, these registries have recorded the incidence of various cancers and research has been concentrated on aetiological factors and time trends in incidence. Now the registries are moving toward a trend where evaluation of treatment plays a more central role. This paper adds to a series of publications based on the evaluation of lung cancer treatment in Norway.11,12 The purpose of this study was to present relative and observed survival in different subgroups after resection and to quantify prognostic factors in a defined population.
METHODS
All newly diagnosed cases of cancer are required by Norwegian law to be reported without patient consent to the Cancer Registry of Norway. Since 1953, the Registry has collected information on all cancer patients in the population from clinical and pathology reports. The Registry also routinely receives death certificates from the Cause of Death Registry of Statistics Norway. For patients whose clinical or pathology reports were not satisfactory, supplementary reports from the hospital records were requested. Electronic summary discharge files from hospitals have been available from 1998 and were used for quality assurance. Administration of radiotherapy or chemotherapy was reported on clinical reports as “yes” or “no”. Supplemental information regarding preoperative and postoperative radiotherapy was obtained from verification systems of the linear accelerators located at the six different oncology units in Norway (including two satellite units). For all patients diagnosed from 1993 to 1998, supplementary information was requested, including details of co-morbidity.
Data on all lung cancer patients diagnosed during the period 1993–2002 were analysed retrospectively. Cases diagnosed at necropsy or notified with death certificate only were excluded (n = 704). Of the remaining 19 582 cases, surgical treatment was performed in 3211 patients and these were studied in detail. Twenty patients underwent surgery twice in the period for synchronous or metachronous tumours. Observation was terminated on 31 December 2004. Patients who had emigrated (n = 13) were followed up to the date of emigration or to the date of the last consultation after emigration, if known.
Information on treatment, including the date of operation and type of resection performed, was derived from clinical or pathology reports. Supplementary information including operative reports was retrieved from hospitals when the information was found to be incomplete. The survival time was calculated from the date of operation to the last follow up date.
All cases were restaged at the Cancer Registry according to pathology TNM (pTNM) by an experienced thoracic surgeon (HR).13 For synchronous tumours with different histopathology, the T stage of the most advanced lesion determined the T category according to the current TNM system. Only the first tumour was included in analyses in patients with metachronous tumours. The tumour size (largest diameter) as measured by the pathologist was described in 97% of the pathology reports.
Surgery
Surgical procedures were carried out at 27 hospitals by general or thoracic surgeons. The usual procedure was open thoracotomy, but in recent years a few surgeons performed thoracoscopic procedures, mainly for patients with small peripherally located tumours. When a limited resection of another lobe in addition to a lobectomy was performed, the procedure was classified as a lobectomy only. A limited resection is mainly performed in patients with severe co-morbidity as lobectomy is the standard of care. Tumours that could be diagnosed by a bronchoscope were regarded as centrally located, while others were classified as peripheral unless the pathology report indicated the opposite.
Analysis of data
Descriptive analyses of survival were only carried out for patients diagnosed and operated on before the year 2000, in order to have at least a 5 year follow up period. Cox regression analysis was used for all cases.
Univariate analyses were performed with independent sample t tests and Pearson χ2 statistics including χ2 test for trend. Included in the analyses were age, sex, side of resection, surgical procedure and technique, tumour stage and size, histopathology type, and treatment volume expressed by number of resections per year on average of the treating hospital.
Relative survival was estimated using the life table method14 and was calculated as observed survival in the patient group divided by expected survival of a comparable group from the entire general population (Norway), matched by current age, calendar time and sex. The life tables for each sex were obtained from the Statistics Norway by 1 year groups of age and period. The survival rates in each subgroup of patients were thus adjusted for the expected mortality that the group would have from all causes of death.
Prognostic factors were evaluated both by analysis of crude effects and adjusted for other factors using the Cox proportional hazard regression model.15 The statistical software SPSS Version 12.0 was used for descriptive, univariate and multivariate analyses.
RESULTS
Resections were performed in 2061 men and 1150 women during the period studied. The resection rate was 16.4% for the whole country. Postoperative mortality within 30 days of surgery was 4.8% (women 2.4%, men 6.1%). Median age was 66 years (mean 64.2, range 8–87). In patients aged less than 50 years, 54.1% of resected patients were men, increasing to 72.3% in those aged more than 80 years. Synchronous tumours were found in 112 patients, 101 of which were satellite tumours to the index pulmonary tumour.
Adjuvant chemotherapy or radiotherapy (or both) were given to 14.2% of resected patients in the period studied. Information on co-morbidity was known for 1837 patients diagnosed between 1993 and 1998; 14.9% had cardiac disease only, 12.6% had respiratory disease only, and 3.2% had both. Diabetes mellitus was present in 3.3%.
There was a higher proportion of squamous cell carcinoma in men than in women (44% v 23%), while the opposite was true for adenocarcinomas (33% v 47%). The proportion of pneumonectomies varied greatly between different centres (range 9.5–45.0%, mean 26.5%, p<0.001) and declined throughout the diagnostic period with a rate of 31% in 1993 and 23% in 2002 (p for trend = 0.011). The proportion of pneumonectomies was higher in men than in women (30% v 20%). Resection by minimal invasive technique was performed in 100 cases, mostly in the later years.
There were more procedures on the right side than on the left side (1752 v 1459). In 212 patients the margin was involved or possibly involved. The proportion of involved resection margins did not differ between patients operated on by the thoracoscopic or open technique. The overall stage distribution was representative for all histologies except bronchioloalveolar carcinomas and carcinoids, which both had a higher proportion of patients in stage I (79% and 91%, respectively). Of patients with small cell lung cancer 61% were operated with disease in pStage I.
The mean tumour size was 4.1 cm (range 0.3–16.5) for all cases; it was larger in the lower lobe than in the upper lobe (4.2 cm and 3.2 cm, respectively; p<0.001). Sufficient information was collected for 1835 patients to decide whether the location of the tumour was central or peripheral: 1120 tumours (61%) were localised peripherally. Adenocarcinomas and bronchioloalveolar carcinomas were peripherally located in 74% and 83% patients, respectively, while squamous cell carcinoma and carcinoids were located peripherally in 48%.
Survival
Observed survival at 1, 3, and 5 years was 74.4%, 50.9% and 40.9%, respectively (fig 1⇓). Subgroup analysis, with both relative and observed survival for patients diagnosed and operated on in the period 1993–9, is shown in table 1⇓. There was no trend towards a change in survival throughout the period; the 5 year survival for each diagnostic year varied between 37.9% and 41.2%.
Five year relative and observed survival in patients diagnosed and undergoing surgery in 1993–9 (n = 2144)

Kaplan-Meier survival plot for patients resected for lung cancer in Norway, diagnosed in 1993–2002 (n = 3211).
The pneumonectomy procedure was associated with the poorest prognosis, while lobectomies had the highest observed survival (fig 2⇓). Survival after upper lobectomy was significantly better than after lower lobectomy in multivariate analysis (p = 0.017).

Kaplan-Meier survival plot for patients resected for lung cancer in Norway according to procedure, diagnosed in 1993–2002 (n = 3211).
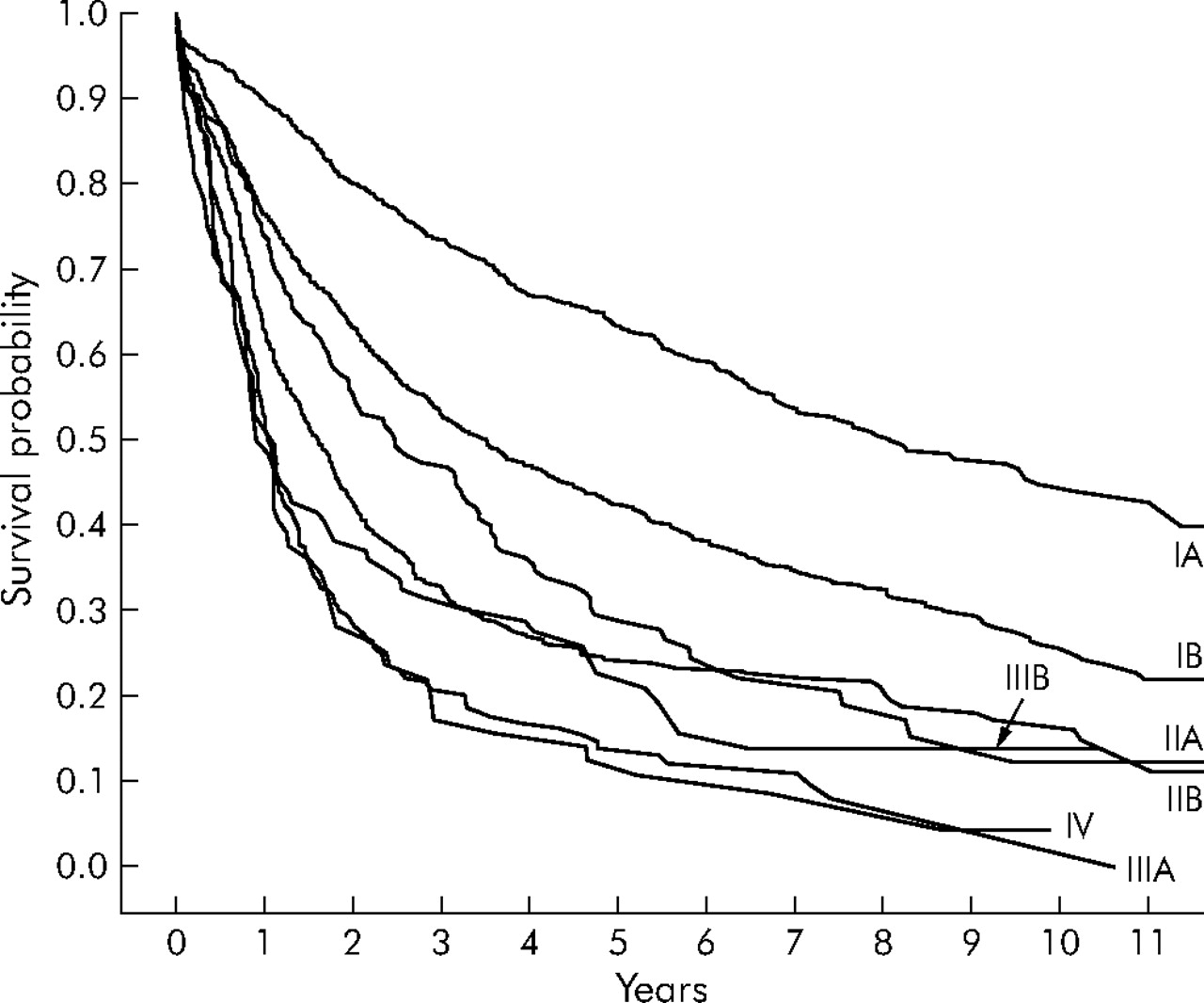
According to the principles of the TNM staging system, the survival rate should decrease with higher stages (fig 3⇓). Patients with stage IIIb and IV disease had a better prognosis than those with disease stage IIIa, but this was not significant. This difference was caused by cases with satellite tumours. Synchronous tumours of the same histology in the same lobe are classified as T4 (stage IIIb), while tumours in different lobes are designated M1 (stage IV). When patients with synchronous tumours in the same lobe were analysed separately (1993–9), the observed 5 year survival was 30.0% (95% CI 16.2 to 43.7; n = 43) compared with 8.0% (95% CI 0.0 to 18.5; n = 25) for patients with one T4 tumour due to other reasons. Likewise, for patients in stage IV, no patients with extrathoracic metastases to the liver, brain or adrenal gland (n = 9) lived more than 5 years (only two patients lived more than 1 year), while patients with synchronous tumours in different lobes (n = 35) had a 5 year observed survival rate of 22.9%. The 5 year observed survival was 49.3% for patients with nodal stage N0 (n = 2247), 24.0% for N1 (n = 750), and 13.1% for N2 (n = 212).

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival plot for patients resected for lung cancer in Norway according to stage, diagnosed in 1993–2002 (n = 3211).
As shown in table 1⇑, large tumour size was significantly associated with reduced long term survival. The corresponding 5 year relative survival rates for patients in stage I were 69.7% (95% CI 65.4 to 74.0), 55.3% (95% CI 49.8 to 60.8), and 36.9% (95% CI 30.4 to 40.3) for tumour size ⩽3.0, >3.0–5, and >5 cm, respectively.
Cox regression analysis for all patients identified male sex, higher age and stage, procedures other than upper and middle lobectomy, histologies such as adenocarcinoma and large cell carcinoma, surgery on the right side, infiltration of resection margins, and larger tumour size as prognostic factors for non-favourable survival (table 2⇓).
Univariate and multivariate analysis of risk factors affecting survival after surgery for lung cancer: patients diagnosed in 1993–2002 (n = 3211)
The effect of co-morbid disease (classified as presence of cardiac disease, lung disease, or diabetes) on survival was analysed with Cox proportional hazard regression in the subset of patients for whom this variable was available (patients diagnosed 1993–8). Co-morbid disease was significantly associated with inferior survival (hazard ratio 1.21, p = 0.001) but, when adjusting for this variable, the effect of the other independent risk factors was not changed. In particular, the effect of hospital volume was unchanged after adjustment for co-morbidity (data not shown).
DISCUSSION
This population based study of all lung cancer patients resected during a 10 year period in Norway shows favourable long term survival. Even elderly patients, those with advanced stage disease and subgroups with small cell lung cancer, nodal invasion (N1–N2), and patients with multiple tumours may be cured with surgery. A high proportion of patients had substantial co-morbidity and few received adjuvant treatment.
Norway is a small country of about 4.5 million inhabitants and hospital health services are free of charge. The use of multiple sources of information in the Cancer Registry makes reporting of the incidence of various cancers reliable and complete, and it is believed that all new cancers are reported to the Registry.16 We have no exact knowledge of the policy at each hospital in Norway regarding selection of patients for surgery. Similarly, we do not know how the relative contraindications are determined. A decision to offer surgery is generally based on the technical feasibility of resection and evaluation of the patient’s co-morbidity, provided that the patient consents to undergo a surgical procedure.
Relative survival in lung cancer is useful in making comparisons between different series of different origins possible.8 However, there are few population based reports on long term relative survival after lung cancer surgery in the literature, and detailed subgroup analyses have not been presented.9,17 Some of the hospitals in Norway have presented their survival results which partly or completely overlap this time period, and hence include the same patients. Their results correspond to ours when stratifying on these hospitals (data not shown).18,19
The survival rates in Norway are slightly inferior to those published in other comparable reports.10,20 Higher postoperative mortality could explain some of this, but the main reason is probably that the patients operated on are unselected in this population based study.21
The poor prognosis after sublobar resection compared with lobectomy, which was particularly evident in the multivariate analysis, was probably caused by local recurrence and co-morbidity.22 Survival after lower lobectomy was significantly reduced compared with upper lobectomy in univariate and multivariate analyses of all patients. To the authors’ knowledge, this finding has not been previously reported. Involved resection margins were an independent adverse risk factor, confirming findings in other reports.10
Adenocarcinomas, which are more frequent in women, were identified as a prognostic risk factor for reduced survival; in other studies this effect seems uncertain.23–,25 In a previous report we found that 5 year survival was about 45% in patients resected with small cell lung cancer, which was significantly better than other treatment modalities.12 This is a highly selected group since few patients present with limited stage disease. The favourable survival rates in patients with bronchioloalveolar carcinoma could be explained by the high proportion with limited stage disease. This might explain why bronchioloalveolar carcinoma was not an independent risk factor for survival in multivariate analysis. Carcinoids, not surprisingly, represent a tumour group with excellent prognosis.26
Patients with advanced disease should be carefully examined and evaluated with the aim of performing a resection if technically possible. In our unselected series there seems to be a role for surgery in patients with N2 disease; 13.4% survived for more than 5 years, although this survival rate was lower than other series which have reported 5 year survival rates of 20–26% in this group.27,28 Also, for multiple tumours with the same histology, the results indicate that surgery is a curative treatment and it is questionable if they should be categorised as stage IIIb and IV.29
Tumour size (⩽3 or >3 cm) seems to be insufficiently accounted for in the current TNM classification system, and a 5 cm limit has been suggested as a new category.30 Our data support the conclusion that patients with tumours >5 cm have a significantly poorer prognosis than those with smaller tumours.
Large hospital volume has been found to have a positive effect on long term survival.31 This was not supported in our multivariate model of hospitals performing an average of more or less than 20 procedures per year. Similarly, surgeon volume has been shown to have an important effect on outcome.32 At some small volume hospitals in Norway there are high volume surgeons who could interfere with the hospital volume effect. Another source of confusion is the difference in selection of patients at the different centres. Small units may perform resection only in patients without major risk factors for surgery, although analysis of the subset of patients with co-morbidity data did not change the absence of hospital volume effect.
In conclusion, we found favourable long term survival after lung cancer surgery in a population based study. Even subgroups with high age, advanced stage, small cell lung cancer, nodal involvement, and patients with multiple tumours at diagnosis should be operated upon when technically possible because the survival is better than with other treatment modalities. These results could therefore stimulate a more aggressive approach in the selection of patients for surgery.
Acknowledgments
The authors thank Professor Odd Geiran, Rikshospitalet-Radiumhospitalet, for valuable comments on the manuscript.
REFERENCES
Footnotes
Published Online First 5 April 2006
The first author has received a grant of 1000 Euro from the International Association for the Study of Lung Cancer (IASLC) as a Young Investigator Travel Award when the results were presented at the 11th World Conference on Lung Cancer.
None of the authors had competing interests in this study.
All patient information for this study was collected according to Norwegian law and statutory regulations, specifically stating that this information should be used for research purposes without patient consent. Ethics committee approval is thus not sought for this kind of study.