Article Text

Abstract
Background: Health related quality of life (HRQOL) after surgery is important, although very limited data are available on the QOL after lung cancer surgery.
Methods: The effect of surgery on HRQOL was assessed in a prospective study of 110 patients undergoing potentially curative lung cancer surgery at Papworth Hospital, 30% of whom had borderline lung function as judged by forced expiratory volume in 1 second. All patients completed the EORTC QLQ-C30 and LC13 lung cancer module before surgery and again at 1, 3 and 6 months postoperatively.
Results: On average, patients had high levels of functioning and low levels of symptoms. Global QOL had deteriorated significantly 1 month after surgery (p = 0.001) but had returned to preoperative levels by 3 months (p = 0.93). Symptoms had worsened significantly at 1 month after surgery but had returned to baseline levels by 6 months. Low values on the preoperative HRQOL scales were not significantly associated with poor surgical outcome. However, patients with low preoperative HRQOL functioning scales and high preoperative symptom scores were more likely to have poor postoperative (6 months) QOL. The only lung function measurement to show a marginally statistically significant association with quality of life at 6 months after surgery was percentage predicted carbon monoxide transfer factor (Tlco).
Conclusion: Although surgery had short term negative effects on quality of life, by 6 months HRQOL had returned to preoperative values. Patients with low HRQOL functioning scales, high preoperative symptom scores, and preoperative percentage predicted Tlco may be associated with worse postoperative HRQOL.
- lung cancer
- surgery
- quality of life
Statistics from Altmetric.com
There has recently been increased recognition of the need to complement cancer treatments with an assessment of health related quality of life (HRQOL) experienced as a result of the disease and its treatment. The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-C30 (EORTC QLQ-C30) together with the lung cancer module (LC13) is the most commonly used HRQOL assessment tool for cancer patients in European countries1–5 and was found to be the best developed instrument.1 Collection of postoperative HRQOL data has been advocated in follow up of patients with cancer6 and most published studies encourage the assessment of HRQOL in evaluating treatment outcomes.1–4,7,8
Patients with lung cancer frequently have some degree of lung function impairment.9 Although lung resection remains the most effective treatment for patients with operable non-small cell lung cancer (NSCLC),10,11 patients with borderline lung function are at increased risk of complications from surgery and of functional impairment postoperatively. For many patients the risk of an impaired HRQOL after surgery is an important consideration when deciding whether to proceed with surgery. Some patients may regard immediate postoperative complications as an acceptable risk, but are not prepared to accept significant postoperative functional debility.12 However, there is very little information available about the effect of surgery on HRQOL in this group of patients, and the way in which postoperative HRQOL relates to preoperative factors.
This study aimed to assess prospectively the effect of lung cancer surgery on HRQOL measured using the EORTC QLQ-C30. In addition, we examined the association between preoperative HRQOL and clinical characteristics, and poor surgical outcome defined by operative complications and HRQOL at 6 months.
METHODS
Patients
Between January 2001 and December 2003, 150 patients were assessed for curative surgery for lung cancer at Papworth Hospital. Of these, 32 were not referred for surgery and were excluded from the study (nine due to lack of fitness for surgery, three refused surgery, and 20 due to upstaging). A further eight patients were deemed not resectable at the time of exploration (open and closed thoracotomy) and were not studied further. The remaining 110 patients (30% of whom had borderline lung function as judged by forced expiratory volume in 1 second (FEV1); preoperative post-bronchodilator FEV1 <1.5 l for lobectomy, <2.0 l for pneumonectomy) made up the study sample. All patients gave written informed consent and the local ethics committee approved the study.
In addition to HRQOL results, demographic data, staging, operative details, and results of preoperative lung function and exercise tests were recorded. All had full pulmonary function tests according to the Association of Respiratory Technology and Physiology Practical handbook of respiratory function testing guidelines. The shuttle walk test was performed as described by Singh et al13 and the cardiopulmonary exercise test was performed using the Standardized Exponential Exercise Protocol (STEEP) protocol as described by Northridge et al.14
HRQOL assessment
The EORTC QLQ-C30 includes five functional scales (physical, role, emotional, social and cognitive functioning), three symptom scales (fatigue, pain and nausea/vomiting), a global health status/quality of life scale, and a number of single items assessing additional symptoms and perceived financial impact, as well as LC13 which assesses lung cancer specific symptoms such as cough, haemoptysis, severity of shortness of breath, chest/body pain, and chemotherapy/radiotherapy side effects symptoms such as sore mouth, dysphagia, peripheral neuropathy, and hair loss. The EORTC QLQ-C30 and lung cancer module LC13 were administered to all patients before surgery and at 1, 3 and 6 months postoperatively. Patients completed the questionnaires in the clinic where the study doctor/nurse was available to provide explanation if required. Patients were also seen by the researcher (a specialist registrar in respiratory medicine) at each visit and a lung cancer specialist nurse, and symptoms were actively treated as appropriate. Patients were seen by their surgeon at 6 weeks after surgery as normal.
All scales were re-weighted to a scale of 0–100 according to the EORTC manual for the core questionnaire and the lung cancer module. A high score (60–100) represents a high/healthy level of functioning for a functional scale and a high global quality of life. However, a high score (60–100) for a symptom scale represents a high level of symptomatology.
Statistical analysis
HRQOL scales were generally symmetrically distributed and were summarised using the mean and standard deviation (SD). Plots of mean HRQOL scales and their confidence intervals were used to explore changes over time. Repeated measures analysis of variance was used to assess the significance of changes over time for the main scales of interest (global health status, functioning scales, pain, fatigue, dyspnoea, coughing, and constipation). For these analyses a simple contrast was used with each postoperative measure compared with the preoperative value. For each of the HRQOL scales considered as a function of time, the global p value was <0.05 so post hoc comparisons between preoperative and postoperative intervals were presented.
Poor outcome after surgery was defined as death or a major complication (myocardial infarction, cardiac, renal or respiratory failure, pulmonary embolism, pneumonia or sepsis) within 40 days. The ability of preoperative quality of life scales to predict poor outcome was assessed using logistic regression. In addition, we explored the relationship between 6 month postoperative global health status and preoperative HRQOL scales and preoperative physiological data (FEV1, carbon monoxide transfer factor (Tlco), shuttle walk distance, peak oxygen consumption) using correlation coefficients and scatter plots.
RESULTS
110 patients underwent surgical resection of whom 44 (40%) were women and 66 were men. The mean (SD) age was 69 (8) years (range 42–85). 33% underwent pneumonectomy, 59% lobectomy, 4% bilateral lobectomy, and 4% wedge resection. Four patients (3%) died in hospital within 40 days of surgery and an additional 24 (22%) experienced a major complication (table 1).
Frequency of major complications
Quality of life data were available for all 110 patients at baseline, 94 (85%) at 1 month, and 83 (75%) at 3 and 6 months after surgery. No follow up data were available for nine patients who had died, four undergoing radiotherapy, two undergoing chemotherapy, seven lost to follow up, and five too unwell to complete questionnaires at the time of appointment. Baseline HRQOL was the same in patients with and without follow up data. Preoperative physiological data are shown in table 2.
Preoperative physiological data
Baseline HRQOL is shown in fig 1. On average, patients had high levels of functioning and low levels of symptoms in both the core questionnaire and the lung cancer module. The most frequent symptom at baseline was cough, although pain, dyspnoea and insomnia were also reported.

Baseline quality of life.
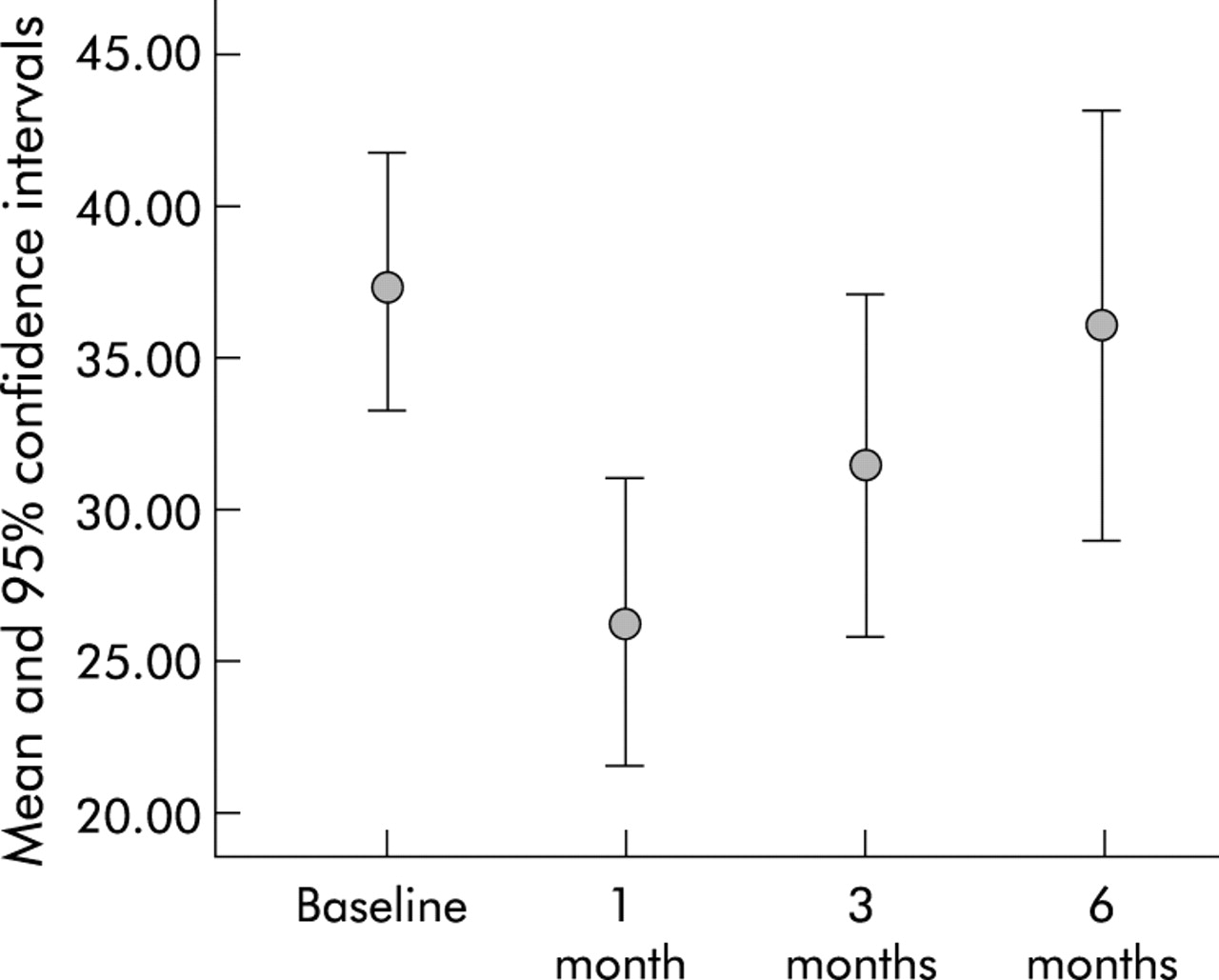
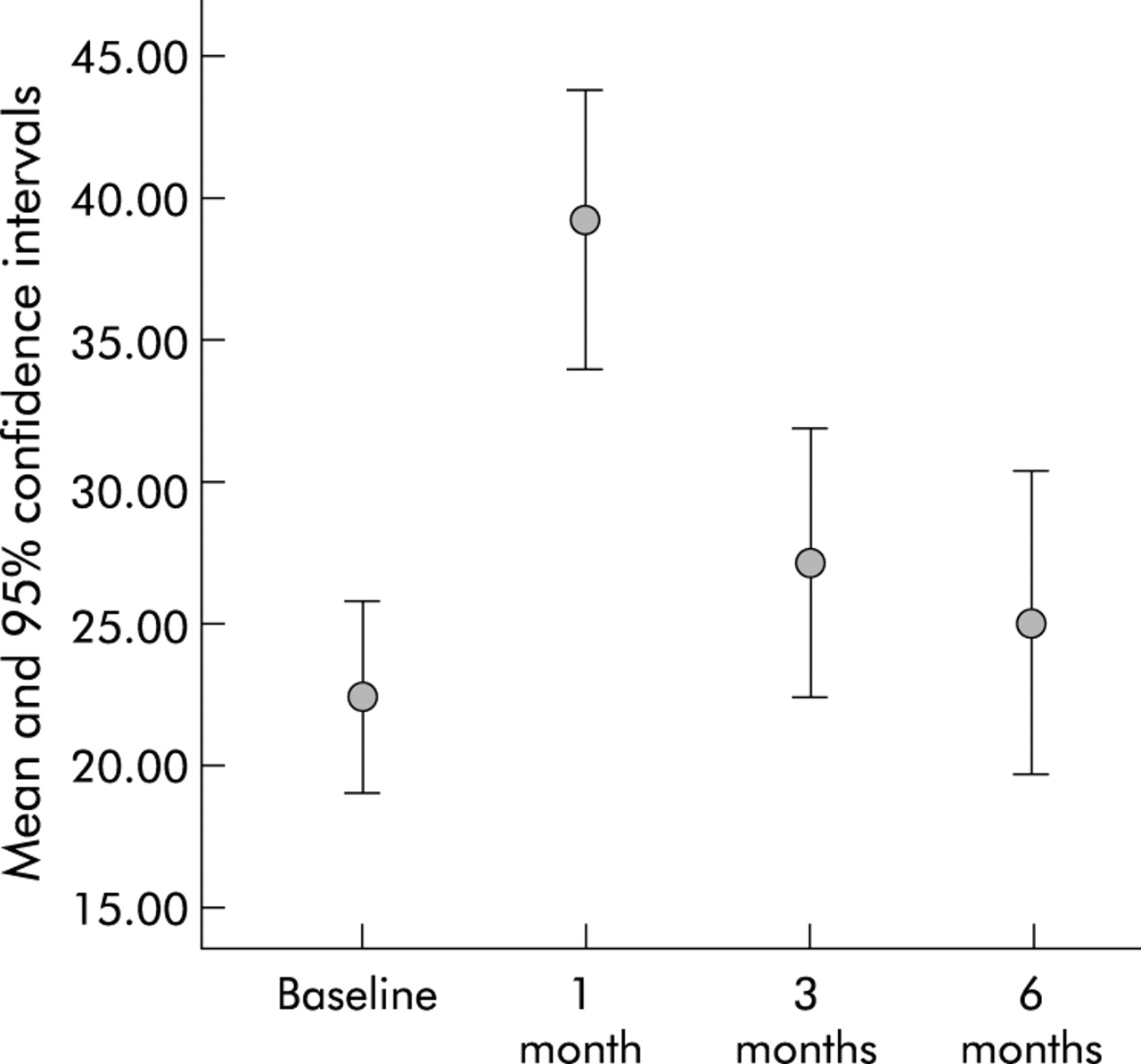
The effect of surgery on global health status is shown in fig 2 for the 83 patients who had HRQOL measurements at all four time intervals. Global quality of life had deteriorated significantly at 1 month after surgery (repeated measures ANOVA compared with baseline p = 0.001) but had returned to preoperative levels by 3 months (p = 0.93, fig 2). The other functioning scales (physical, role, emotional, cognitive and social) showed the same pattern. Symptoms such as fatigue, nausea, pain, and dyspnoea were significantly worse 1 month after surgery but had returned to baseline levels by 6 months (figs 3 and 4). Cough displayed a different pattern in that the symptom was suppressed around the time of surgery (p = 0.003) but had returned to baseline levels by 6 months (p = 0.116).

Effect of surgery on global health status.

Effect of surgery on cough.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect of surgery on dyspnoea.
In this cohort no preoperative HRQOL scales were significantly associated with poor outcome defined by surgical mortality and/or major complication. In exploratory analysis the correlation between baseline percentage predicted Tlco and 6 month global health status was marginally significant (r = 0.22, p = 0.05), although this may have been a chance finding due to the number of multiple analyses carried out, and no other measures of lung function or exercise capacity were significantly correlated with global HRQOL at 6 months (table 3). However, there was an association between preoperative HRQOL scales—specifically, physical and cognitive functioning, fatigue, pain, dyspnoea and dysphagia scales—and 6 month global health status (table 3).
Correlation between global health status at 6 months and baseline lung function, EORTC QLQ-C30 core questionnaire, and lung cancer module
DISCUSSION
The long term goals of lung cancer surgery include improved length and quality of life.15 The main focus for clinicians is predicted mortality and morbidity, but patients are concerned about potential long term disability.12 Follow up of patients with lung cancer to include both survival and postoperative QOL may offer a more comprehensive approach to evaluating the associated risks and benefits.6,16
Clinical QOL studies in unselected lung cancer patients reported pain in 86%, dyspnoea in 70%, and anorexia in 68%.17 There are few published reports of HRQOL in surgical patients.18,19 Using the generic SF36 questionnaire, Handy et al found that preoperative functional health status in lung cancer surgical patients was significantly impaired, and that pain and impaired functioning persisted for 6 months.8 Another study of 117 patients undergoing thoracotomy showed that patients with cancer reported dyspnoea four times as often as patients with benign disease, and that QOL returned to preoperative levels by 6–9 months.19 Zieren et al20 found that, although HRQOL deteriorated soon after surgery, it was restored within 3–6 months in disease-free patients. HRQOL in long term survivors of NSCLC showed a hopeful attitude and patients viewed lung cancer as having made a positive change in their lives.21 Another study of selected surgical lung cancer patients showed significant benefit in terms of long term QOL.22
Our study showed that potentially operable patients had acceptable preoperative HRQOL. Most patients did not experience pain, anorexia, constipation, diarrhoea, nausea or vomiting, although fatigue, dyspnoea and cough were reported with the majority suffering a mild to moderate degree. In common with other studies, most of our patients had recovered by 3 months follow up.20
Our study group also had a better operative outcome in terms of mortality (3% 40 day mortality, 7% 6 month mortality) than other studies (5.8% and 12.2%, respectively8), despite a significant number of patients with borderline lung function in terms of preoperative post-bronchodilator FEV1 <1.5 l for lobectomy, <2.0 l for pneumonectomy. Our patients also had a lower mortality than that acceptable according to the British Thoracic Society guidelines (4% for lobectomy and 8% for pneumonectomy).23 Although mortality was low in our patients, a significant number (22%) of them experienced postoperative major complications. Our patients had similar co-morbidity, incidence of preoperative chemotherapy, and staging (data not shown) to the group described by Handy et al,8 but our patients were also older with a higher frequency of pneumonectomy. In our group mean preoperative FEV1 was similar to that reported by Handy, but mean preoperative Tlco was slightly greater.
It is unclear why postoperative mortality and QOL were more favourable in our study patients than previous studies.8,24 All our patients underwent full staging including head CT and PET scanning before surgery, so we may have excluded patients with unrecognised metastatic disease. However, the fact that more patients underwent pneumonectomy suggests that we did not have a particularly favourable group in terms of local disease progression. In our study patients were reviewed regularly throughout the 6 month follow up period by a respiratory physician and, if necessary, by a respiratory specialist nurse. It is possible that this may have led to improved management of complications and/or symptoms leading to improved QOL at 6 months.
Cough was reduced immediately after operation, most probably due to postoperative pain interfering with the cough reflex. Haemoptysis had resolved in all patients after surgery. Although only a few patients suffered from this, it was the most frightening for them and its resolution was a positive change in their life. According to our findings, financial difficulty was reported in only 6%, mostly those who were self-employed and unable to work around the time of surgery.
Handy et al suggested that restorative surgery probably has a different impact on functional health status than in patients undergoing cancer excision.8 A study of 454 patients which compared QOL in patients undergoing total hip arthroplasty, lung cancer surgery, or abdominal aortic aneurysm repair showed that QOL had improved at 6 months and was sustained for up to 12 months in patients undergoing arthroplasty or abdominal aortic aneurysm but declined and remained reduced at 12 months in lung cancer patients.24 Another study in patients undergoing cardiac surgery showed a significant improvement in QOL within 3–6 months after surgery.25 It is not clear why our results were more favourable than previous studies.8,24 This could be due to better patient selection and staging, a thorough assessment of surgical fitness, extensive consultations before and after surgery regarding possible complications, and/or prompt and appropriate intervention for symptoms at the postoperative follow up clinics.
We found no significant association between preoperative HRQOL scales and poor outcome, as defined by surgical mortality or major complications. This is compatible with previous studies.19 However, one previous study found that QOL was the strongest prognostic factor for survival in lung cancer patients.26 Our study did, however, show a weak correlation between the preoperative percentage predicted Tlco and postoperative HRQOL, which supports the findings of a previous study.8 This could possibly be due to chance as a result of the multiple analyses carried out or, if it is a real association, could be explained by the fact that Tlco may be the most representative measure of the extent of underlying lung disease, being affected by the severity of underlying emphysema, associated underlying interstitial fibrosis, and/or pulmonary hypertension.
As might be expected, preoperative global health status, physical function, and cognitive function were significantly correlated with 6 month postoperative global health status. Dyspnoea and dysphagia on the lung cancer module questionnaire and fatigue, pain, and diarrhoea on the QLQ-C30 questionnaire were significantly inversely correlated with the 6 month postoperative global health status, most probably because these symptoms closely represent late stage of disease.
In summary, potentially operable lung cancer patients had a reasonable QOL compared with a general lung cancer population. Lung cancer surgery had short term negative effects on QOL, but these effects had disappeared by 6 months after surgery. Low preoperative HRQOL results did not predict poor surgical outcome defined by either death or major complication, although they were associated with a worse postoperative QOL (at 6 months). Preoperative percentage predicted Tlco was also suggestive of a worse postoperative QOL at 6 months.
REFERENCES
Footnotes
-
Dr Win received a Department of Health, Eastern Region Research and Development grant.