Article Text

Abstract
AUTHOR:e-mail address please Background: Airway clearance techniques are an important part of the routine care of patients with bronchiectasis. The use of the Flutter, a hand held pipe-like device causing oscillating positive expiratory pressure within the airways, has been proposed as an alternative to more conventional airway clearance techniques.
Methods: A randomised crossover study was performed in 17 stable patients with non-cystic fibrosis bronchiectasis at home, in which 4 weeks of daily active cycle of breathing technique (ACBT) were compared with 4 weeks of daily physiotherapy with the Flutter device.
Results: No significant differences between the two techniques were found. Median weekly sputum weights were similar with a median treatment difference of 7.64 g (p=0.77) and there was no evidence of treatment order or order interaction effects (p=0.70). Health status (Chronic Respiratory Disease Questionnaire) and ventilatory function did not change significantly during either treatment period. There was no significant change in peak expiratory flow rate or in breathlessness (Borg score) after individual physiotherapy sessions with either technique. A questionnaire indicated subjectively that patients preferred the Flutter (11/17) to ACBT for routine use.
Conclusions: Daily use of the Flutter device in the home is as effective as ACBT in patients with non-cystic fibrosis bronchiectasis and has a high level of patient acceptability.
- Flutter
- airway clearance techniques
- bronchiectasis
Statistics from Altmetric.com
Airway clearance techniques such as chest physiotherapy remain an important part of treatment in bronchiectasis, together with prompt antibiotic treatment for infective exacerbations. Interest has been generated in the Flutter device (Varioraw SARL, Scandipharm Inc, Birmingham, Alabama, USA), an alternative to more conventional techniques, which has been tried in a number of respiratory diseases with chronic sputum production including cystic fibrosis (CF),1–6 chronic obstructive pulmonary disease (COPD),7–9 asthma,10,11 and diffuse panbronchiolitis.12
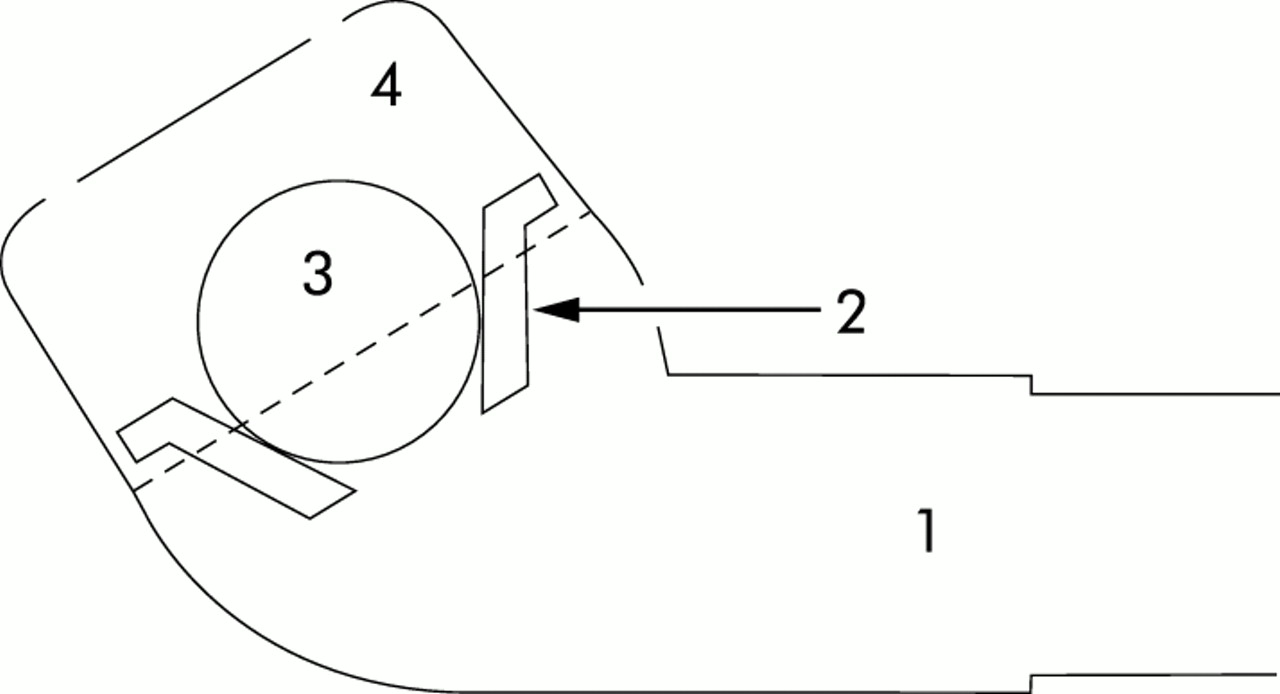
The Flutter is a simple hand held pipe-like device (fig 1) which produces an oscillating pressure wave through the repeated displacement of a steel ball within a cone. The oscillating positive expiratory pressure is reported to prevent premature closure of the bronchi, to loosen secretions, and allows mobilisation of sputum which may be cleared by the forced expiratory technique (FET).10 It is not available on prescription in the UK and costs approximately £45.00.
{kind=link}
Diagram of the Flutter device and its constituent parts: 1 = mouthpiece, 2 = circular cone, 3 = high density stainless steel ball, 4 = perforated protective cover.
The current literature on the efficacy of the Flutter is limited and studies of its use in bronchiectasis have been in patients with CF. A randomised crossover study of patients with stable CF compared 4 weeks of treatment with the Flutter with autogenic drainage. No differences were found in sputum weight or lung function after a single session with either method at the end of the treatment period, but sputum viscoelasticity was significantly reduced with the Flutter.13 Konstan et al reported that up to three times more sputum was produced with the Flutter than with postural drainage in similar subjects.3 In contrast, again in patients with stable CF, Pryor et al found that significantly more sputum was produced with the active cycle of breathing technique (ACBT) than with the Flutter in individual supervised sessions, but similar sputum weights were produced with both methods over 24 hours.1 Two studies compared the Flutter with percussion, vibration, and postural drainage by a physiotherapist in children with CF admitted to hospital with an acute exacerbation and found no significant differences in lung function or exercise tolerance.2,4
Most studies are short with physiotherapist supervision in hospitalised patients.1,2,4 Comparisons have been made between sputum produced from individual physiotherapy sessions rather than total daily production over several days.13 One study of more than a year in children with CF compared the Flutter with the positive expiratory pressure mask and found a greater decline in forced vital capacity (FVC), increased hospital admissions, and increased antibiotic use with the Flutter.6
Different airway clearance techniques used for comparison with the Flutter, inconsistencies in its application, and various outcome measures all contribute to the difficulties in interpreting the literature. The physiological properties of sputum differ in CF and non-CF bronchiectasis,14 so different airway clearance techniques may vary in their efficacy.
To our knowledge there are no comparative studies with the Flutter device in patients with non-CF bronchiectasis. We have performed a study in such patients at home, comparing the efficacy of the Flutter with ACBT.
METHODS
Study design
ACBT and the Flutter were each used unassisted at home for 4 weeks in a randomised crossover design. Patients with productive bronchiectasis attending a specialist respiratory outpatient clinic were recruited. Baseline medication was not altered. Exclusion criteria were an inability to perform pulmonary function tests, current pneumothorax, untreated cor pulmonale, and haemoptysis. Patients who had had an exacerbation in the 4 weeks prior to or during the study were withdrawn.
All patients had previously been trained in the ACBT (breathing control, thoracic expansion exercises, and FET) and postural drainage. Before the ACBT arm each patient had a refresher session with the physiotherapist (SH) who optimised their technique. Before the Flutter arm they were instructed to tilt the device until maximum vibrations were felt within the chest to loosen the sputum which was cleared with FET. They were asked to perform the airway clearance techniques twice daily until there was no further sputum to expectorate. Written instructions were provided. Postural drainage was used as necessary throughout.
Patients recorded the daily weight of sputum produced (Ohaus LS200 electronic scales), the duration of physiotherapy, peak expiratory flow rate (PEFR), and breathlessness (Borg scale) before and after each physiotherapy session. Post bronchodilator spirometric tests, PEFR, and health related quality of life (Chronic Respiratory Disease Questionnaire (CRQ)) were measured at baseline and after each arm. A questionnaire on completion of the study asked which technique was preferred for routine use.
Statistical analysis
The study was powered to detect a standardised effect size of 0.8. Fifteen patients provide 80% power to detect this using a paired t test with a two sided 5% significance level. One patient failed to complete their sputum diary for week 4 under both treatments so the mean value for 3 weeks was used. For the Borg scores and PEFR, the mean difference between the values recorded immediately before and after treatment, averaged over each 4 week arm, were used. Normally distributed data are expressed as mean (SD) values and treatment differences with 95% confidence intervals (CI) were analysed using the t test. Non-normal data are expressed as median values with interquartile range (IRQ) and differences were analysed using the Wilcoxon rank sum test. A change of ±0.5 in the CRQ score is associated with a minimum clinically important difference in health status. In addition, for each outcome, tests were performed for a treatment effect, an order effect, and for order interaction. Bonferroni corrections were applied as appropriate. A p value of <0.05 was considered statistically significant.
RESULTS
Five of the 22 patients recruited to the study were withdrawn. All five used the Flutter first; three dropped out because of an infective exacerbation (two during the Flutter arm and one during the ACBT arm) and two recorded insufficient data for analysis. Baseline characteristics for all who entered the study are shown in table 1.
Baseline characteristics and treatment differences between 4 weeks of treatment with the Flutter and 4 weeks of ACBT
The diagnosis of bronchiectasis had been confirmed by prior CT scanning (14/17) or bronchography (3/17). None had CF; the underlying aetiology of the bronchiectasis was unknown in six cases, post-pneumonic in four, post-whooping cough in six, and one was associated with inflammatory bowel disease.
There was no significant difference between the ACBT and Flutter for any outcome (table 1), nor was there evidence to suggest any treatment order or interaction effect (p>0.1). Median (IQR) daily sputum weights were 26.6 g (15.0–45.2) for ACBT and 23.4 g (16.8–36.2) for the Flutter (p>0.05). There was a statistically significant improvement in FEV1 with the Flutter, but this did not achieve a clinically meaningful change. The mean (SE) total time spent each day performing the airway clearance techniques was similar (29.5 (17.0) minutes and 25.9 (11.7) minutes for the ACBT and Flutter, respectively; p>0.05). Eleven of the 17 patients preferred the Flutter for routine daily use, three preferred ACBT, and three had no preference. One patient reported nausea using the Flutter; no other adverse events occurred.
DISCUSSION
This study shows that the Flutter is as effective in aiding sputum clearance in patients with non-CF bronchiectasis as the ACBT. Previous studies have frequently been performed in hospital with supervision from a physiotherapist and over a shorter time varying from a single physiotherapy session13 to a few days.1,4 Our study confirms the efficacy of the device when used unsupervised by the patient in the home over a period of 1 month. Many earlier studies2–5,13 did not include comparison with the now widely accepted ACBT, nor did they include FET with the Flutter,15 and this may explain why we have found the technique to be effective where others have not.1
Ventilatory function, sputum production, and health related quality of life are not the only important outcome measures; exercise capacity, use of medication, the number and duration of infective exacerbations, and cost effectiveness are other parameters not addressed by our study which could be incorporated into a future study over a longer period.
The Flutter was well tolerated; there were no adverse events with either technique, although one patient reported nausea after using the Flutter and a pneumothorax has been reported in the literature in a patient with panbronchiolitis.12 Like others,3,10,11 we have found the Flutter to have a high level of patient acceptability; 11 of the 17 patients preferred the Flutter for routine use and its ease of use was commented upon.
A recent review of airway clearance techniques in adults15 has suggested that, if the objective differences are small between the different techniques, then individual preferences are likely to play an important part in compliance with treatment. We have found the Flutter to be as effective as the ACBT in the home in a group of patients with non-CF bronchiectasis and therefore suggest that individuals with bronchiectasis should be offered a trial of the Flutter and, if preferred by them, it should be recommended for regular daily use.
Acknowledgments
The authors acknowledge the Medical Illustration Department, K Parry and Dr C Rogers, Research and Development Unit, North Bristol NHS Trust.
REFERENCES
Footnotes
-
Funded by Frenchay Respiratory Research Fund.
-
Conflict of interest: none.