Article Text

Statistics from Altmetric.com
The past decade has witnessed an explosion in the interest of biologists in the gas nitric oxide (NO). This highly reactive free radical, first considered only a noxious air pollutant, is produced in mammalian cells by specific enzymes and is believed to play a vital role in many biological events including regulation of blood flow, platelet function, immunity, and neurotransmission.1 ,2Direct measurement of NO in biological tissues is difficult to perform because this gas reacts rapidly with, for example, haemoglobin or other Fe2+-containing proteins. It is therefore often necessary to rely on indirect measurements in order to detect NO synthesis in vivo. Unlike the situation in most biological tissues where NO is rapidly destroyed, in the gas phase NO is fairly stable at low concentrations.3 NO produced in superficial structures of hollow organs will diffuse into the lumen and thus be detectable in gas collected from such organs.
The presence of NO in exhaled breath of humans was first demonstrated by Gustafsson et al in 1991.4Later studies clearly showed that, in healthy controls at rest, almost all NO found in exhaled air originates from the upper airways with only a minor contribution from the lower respiratory tract and the lungs.5-7
Origin of nasal NO
The exact origin of the NO found in nasal air and the relative contribution from different sources within the nasal airways are not known. There are, however, some indications that favour the paranasal sinuses rather than the mucosa of the nasal cavity as a major source of nasal NO in adult healthy humans.8 Firstly, NO release in the sinuses is markedly reduced by intrasinus instillation of an NO synthase inhibitor (l-NAME) whereas nasal NO concentrations are only slightly reduced following intranasal administration of this inhibitor.9 Secondly, immunohistochemical and in situ hybridisation studies showed dense staining for nitric oxide synthase (NOS) and its mRNA in sinus epithelium whereas only weak staining was found in the nasal epithelium.9 Thirdly, a transient decrease in nasal NO (measured from one nostril) was observed in a study when air was continuously removed from one maxillary sinus during nasal sampling and the opposite (transient elevation) occurred when air was injected into the same sinus.10 Fourthly, nasal NO levels are markedly reduced in patients who generally have mucus filled paranasal sinuses and obstructed sinus ostia (Kartagener’s syndrome,6 cystic fibrosis,11 acute sinusitis12). Finally, nasal NO levels are high in humans and other primates13 but very low in baboons,14 the only mammal lacking paranasal sinuses.
Both immunohistochemical and in situ hybridisation studies indicate that the NOS found in healthy sinus epithelium9 is identical or very closely related to the inducible NOS (iNOS) that has been cloned from activated human hepatocytes.15 Moreover, NOS activity in sinus mucosa is predominantly calcium independent, a characteristic associated with iNOS.16 However, the regulation of the expression and the activity of sinus NOS seems to differ from that previously described for iNOS. Thus, sinus NOS is constantly expressed and seems to be resistant to steroids,9 ,16 properties normally associated with the low rate NO producing endothelial and neuronal NOS. Immunostaining for NOS in the nasal mucosa has shown only weak staining for iNOS.9 Moreover, Ramis et alfound only calcium dependent NOS activity in nasal mucosa from healthy subjects.17 Human nasal epithelium from patients with nasal polyp disease express increased iNOS mRNA compared with normal epithelium.18
Measurement of nasal NO
Almost all studies in the literature on the measurement of nasal NO have used the chemiluminescence method. This method uses an excess of ozone (O3) which reacts with NO to produce nitric dioxide (NO2) with an electron in an excited stage (NO2*). NO2* changes back to the ground state while emitting electromagnetic radiation in the wavelength range 600–3000 nm. A photomultiplicator tube that proportionally converts the intensity of luminescence into an electrical signal detects this chemiluminescence. The chemiluminescence technique is highly sensitive and NO can be detected in levels down to parts per trillion.3 ,19 It is rapid and easy to use which allows for on line measurements of exhaled NO. Other techniques that have been used to establish that NO is present in the exhaled breath of humans include mass spectroscopy and gas chromatography-mass spectroscopy.4 ,20
Several techniques have been used for collecting nasal air, the most commonly used method being to sample nasal air directly from one nostril.21 ,22 Using the intrinsic flow of the chemiluminescence analyser or an external pump, air is aspirated from one nostril. The contralateral nostril is left open and the subject either holds his/her breath or breathes through the mouth. Air is thereby forced from one side of the nose to the other via the nasopharynx. To avoid contamination with NO from the lower airway the subject can be asked to exhale orally against a resistance in order to close the soft palate.23 ,24
Another suggested method of measuring nasal NO is to exhale through the nose after a full inhalation to vital capacity. The exhalation should be made at a constant flow rate. Following this procedure the subject then exhales through the mouth from full vital capacity at the same flow rate and the NO value from oral exhalation is subtracted from that measured during nasal exhalation (unpublished observation).
The optimal measurement technique for nasal NO is yet to be determined. A reliable and standardised method will allow for better comparisons of results between different laboratories. Attempts to standardise nasal NO measurements are in progress and recommendations for suitable sampling techniques will be given in the near future.
Factors that influence nasal NO levels
MEASUREMENT TECHNIQUE
Since NO is continuously released into the nasal airways the concentration will be dependent on the flow rate by which the sample is aspirated.21 Thus, nasal NO concentrations are higher at lower flow rates. It may therefore be preferable to express nasal NO as the output per time unit (e.g. nl/min) which has been shown to be relatively independent of flow rate.25
PHYSIOLOGICAL FACTORS
In an early study nasal NO was measured in healthy subjects at different ages ranging from 0 to 70 years.9 Interestingly, nasal NO was already present at birth. In a later study Schedinet al found significant nasal NO levels in newborn infants including those delivered by caesarian section.26 In a study by Lundberg et al the same flow rate was used in all age groups and nasal NO was found to be much lower in newborn babies and in infants than in adults. However, if the nasal NO concentration from these data is calculated in relation to body weight, the concentration in children around 10 years of age is found to be approximately twice as high as that in newborn infants and adults. There is no evidence of sex differences in nasal NO, but variation in NO levels has not yet been studied in relation to the menstrual cycle. NO output in the nasal airways is acutely decreased by physical exercise.27-30In the study by Lundberg et al 27 direct measurement from one maxillary sinus showed an 83% reduction in sinus NO concentrations after five minutes of exercise. The decrease in nasal NO levels cannot be explained merely by dilution of nasal air due to changes in nasal cavity volume or increased ventilation. Instead, these changes in nasal NO have been attributed to a reduction in the blood flow in the mucosa of the nasal airways with a concomitant decrease in substrate supply to the high rate producing NOS in the paranasal sinuses.27
DISEASES
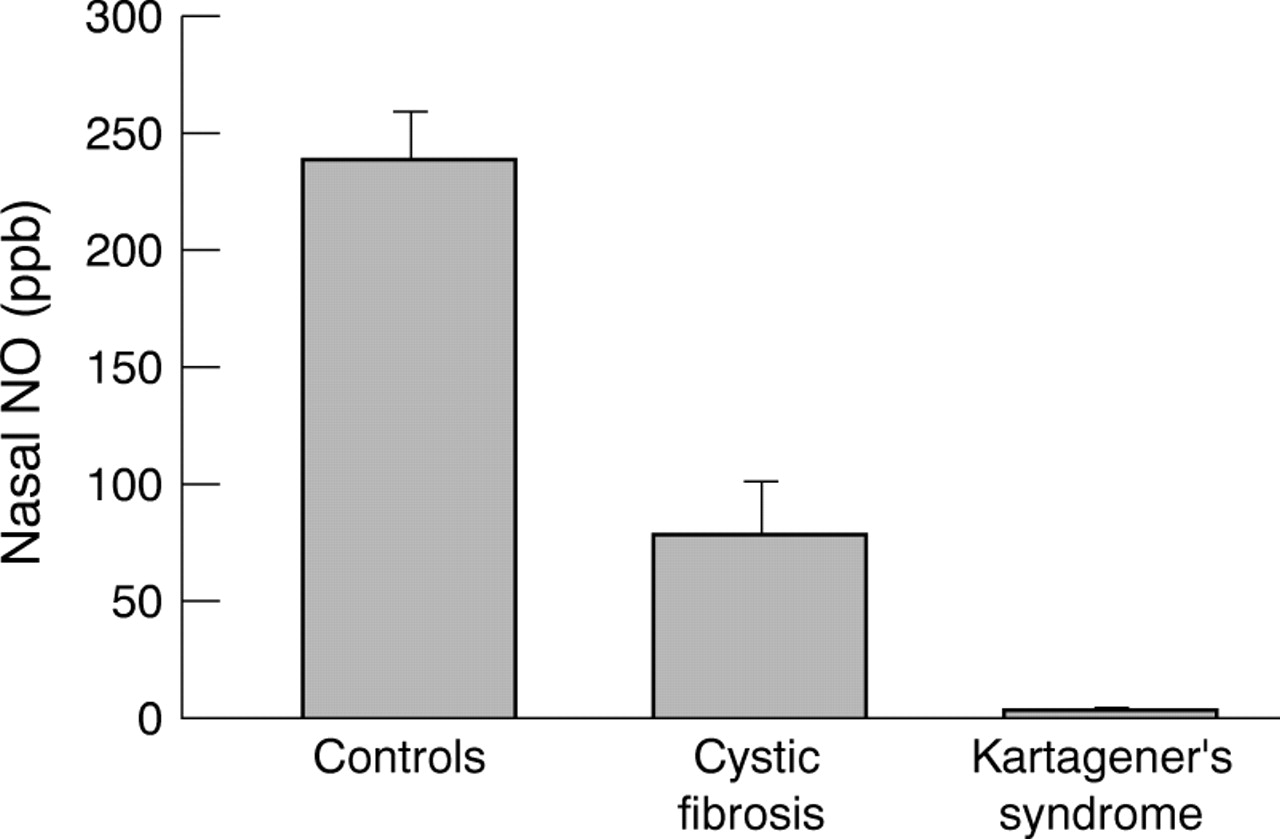
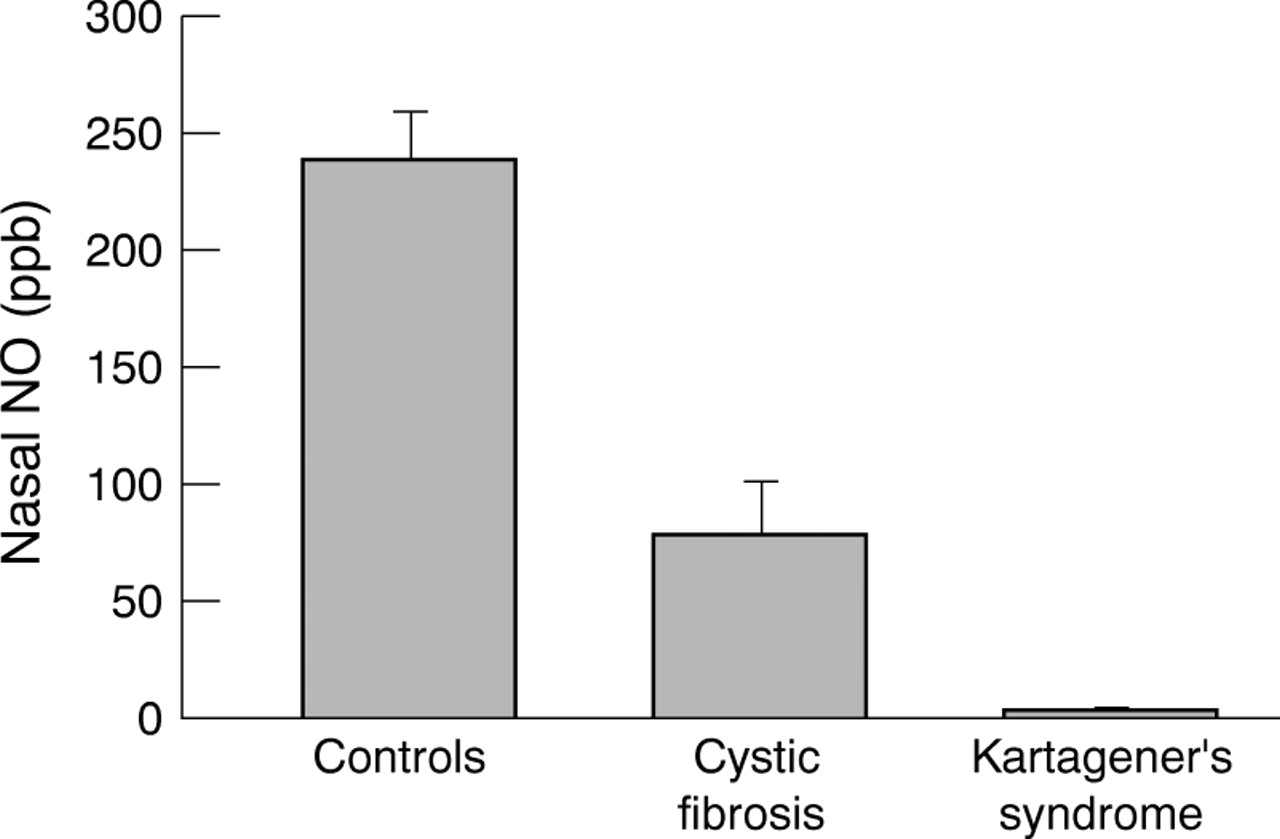
The effects of various diseases on nasal NO levels are summarised in table 1. In children with Kartagener’s syndrome—a triad consisting of sinusitis, bronchiectasis, and situs inversus—nasal NO levels are extremely low compared with healthy, age matched controls.6 Nasal NO levels are also very low in patients with cystic fibrosis (fig 1).11 ,31 ,32 Baraldiet al measured nasal NO in a group of children with acute sinusitis and found low nasal NO levels.12 In these patients nasal NO levels increased when the patients improved following treatment with antibiotics. Chronic sinusitis is associated with more than a 50% reduction in nasal NO levels.33 In general, the above studies indicate that nasal NO levels are lower in subjects with sinus disorders. It has not been established whether the low nasal NO levels in patients with sinus disorders are purely a result of altered passage of NO gas from the sinuses to the nasal cavity or whether the actual production of NO in the sinuses is decreased in these patients.
Nasal nitric oxide (NO): effects of disease
Whether or not nasal NO levels are altered in patients with rhinitis of different aetiology has not been fully established. Some groups have reported higher nasal NO levels in patients with allergic rhinitis.34-38 In one study nasal NO decreased following treatment with nasal topical steroids.35 Kirstenet al reported increased nasal NO levels after nasal challenge with endotoxin-containing swine confinement dust.39 In contrast, we found no alterations in nasal NO levels in a group of children with perennial rhinitis.11The reasons for the discrepancies between the studies are not clear. One might speculate that iNOS is upregulated in the nose during rhinitis,40as is the case in the lower airways in asthma.41 This would explain the higher levels of NO reported in some studies. On the other hand, the swelling of the nasal mucosa present during rhinitis might also lead to partial blockage of the sinus ostia which would result in reduced passage of sinus NO to the nasal cavity where it is measured.
Eccles et al measured nasal NO levels in patients with a common cold but failed to see any differences compared with healthy controls.42 In another study on experimental human influenza nasal NO levels decreased slightly during the symptomatic period.43
A general NO deficiency has been implicated in the pathogenesis of pre-eclampsia, a disease of pregnancy characterised by oedema, hypertension, and proteinuria. However, in a recent study we found similar nasal levels of NO in patients and healthy pregnant controls.44
DRUGS
The effects of various drugs on nasal NO are summarised in table2. Early reports on the effect of topical glucocorticoids showed no effect of these drugs on nasal NO levels.6 In fact, not even systemic steroids in high doses seemed to alter nasal NO levels.16 Gerlach et alsuggested that bacteria in the nasopharynx induced nasal NO release.7 However, we found no effects of systemic antibiotic treatment on nasal NO levels.6 Moreover, as already mentioned, newborn babies delivered by caesarian section had high nasal NO levels.26 Nasal NO release therefore seems to be independent of bacteria normally present in the nasopharynx.
Nasal nitric oxide (NO): effects of drugs, cigarette smoke and physical exercise
Topical nasal decongestants such as oxymetazoline have been shown to decrease nasal NO levels.37 ,42 ,45 The reason for this is not clear but it has been suggested that the decrease in nasal/sinus blood flow induced by these drugs leads to a reduction of substrate supply to the high producing iNOS in the sinuses.45Indeed, substrate supply seems to be of importance for nasal/sinus NO release since intravenous administration of l-arginine resulted in an increase in nasal NO levels.16
Rinder et al looked at the effects of histamine and capsaicin on nasal NO levels but found no effects of these drugs.45
The NO synthase inhibitor NG-nitro-l-arginine methyl ester (l-NAME) has only minor effects on nasal NO levels when administered locally in the nose.9 ,45 In contrast, Albert et al found a substantial decrease in nasal NO levels following intravenous administration of NG-monomethyl-l-arginine (l-NMMA), another NOS inhibitor.46 This fits well with the theory that the paranasal sinuses are the main source of NO in the nasal airways. Thus, NOS inhibitors probably penetrate poorly into the sinuses if administered locally in the nose whereas, if given intravenously, these drugs will reach the sinus mucosa.
Nasal NO levels have been reported to be lower in cigarette smokers7 ,47 but increase one week after smoking cessation.47
Animal models
Schedin et al have measured nasal NO in a large number of species and found high levels only in primates and in elephants.13 Lewandowski et alrecently measured nasal NO in baboons and found only low levels.14 Interestingly, baboons are the only mammal known to lack paranasal sinuses. Because of the large variation in nasal NO output between different species, caution should be taken when comparing data from animal models with results from studies in humans.
Role of nasal NO
Although the exact role of nasal NO is far from clear, it is reasonable to believe that this pluripotent gas is involved in a variety of physiological as well as pathophysiological events in the airways.
HOST DEFENCE
Among the various biological properties of NO are its effects on the growth of various pathogens including bacteria, fungi, and viruses.2 ,48 NO produced by white blood cells is thought to be important in the killing of certain micro-organisms by these cells. Furthermore, some bacteria are sensitive to authentic NO gas in concentrations as low as 100 parts per billion (ppb).49The fact that local NO concentrations in the nasal airways may be several hundred times higher than this supports the notion that NO is involved in local host defence in the upper airways. Local concentrations in the paranasal sinuses can reach 30 000 ppb.9 We have suggested that this NO may help to keep the sinuses sterile under normal conditions. One might speculate that very low nasal NO levels in patients with Kartagener’s syndrome or cystic fibrosis8 contribute to the increased susceptibility to airway infections in these patients. If this is correct, stimulation of endogenous NO production could increase the resistance to airway infections in patients with low nasal NO levels as suggested earlier.6 It is not clear whether NO itself acts directly on micro-organisms or whether it combines with other components to yield other reactive nitrogen intermediates that are toxic.50
Besides acting directly on micro-organisms, NO may also contribute to local host defence by stimulating ciliary motility.51 A study by Runer et al showed that application of an NO donor in the nasal mucosa of humans did, indeed, cause an increase in ciliary beat frequency.52 Furthermore, the same group has shown that low levels of nasal NO correlate with impaired mucociliary function in the human upper airways.53
INFLAMMATION
NO synthesis is clearly enhanced locally at sites of inflammation.54 This has been described not only in asthma5 but also in, for example, inflammatory bowel disease55 ,56 and cystitis.57 However, the role of NO in inflammation is far from certain. Some studies indicate a harmful role for NO during inflammation, whereas others indicate the opposite. Possible pro-inflammatory actions of NO include activation of enzymes such as cyclo-oxygenase or metalloproteases. Moreover, peroxynitrite, which is formed from the reaction of NO with superoxide, can exert toxic effects to tissues.36 ,58The possible harmful effects of NO have been attributed to the large amounts of this gas produced by iNOS during inflammation. However, the recent finding of a constantly expressed iNOS in the nasal airways complicates this picture since it clearly demonstrates that the sole expression of iNOS and the subsequent increased production of NO is not associated with tissue damage. On the contrary, iNOS in the upper airways may serve important protective functions as discussed above. Furthermore, in an animal model of colon inflammation McCaffertyet al have shown that mice lacking the iNOS gene develop a much more severe inflammation than wild type mice.59
NASAL NO AS AN AIRBORNE MESSENGER
The effect of inhaled exogenous NO is currently being investigated in large scale clinical trials in patients with pulmonary hypertension and/or adult respiratory distress syndrome and its clinical use in newborn children with persistent pulmonary hypertension has been reported.60 Several investigators have found clear effects on arterial oxygenation and pulmonary arterial pressure using concentrations of inhaled NO as low as 10–100 ppb.61 ,62Interestingly, during normal breathing endogenous NO is inhaled at concentrations (approximately 100 ppb) which are known to have vasodilating effects in the pulmonary circulation.6 ,7 We have shown that nasal breathing reduces pulmonary vascular resistance and improves arterial oxygenation compared with oral breathing in subjects without lung disease (fig 2).8 ,63 ,64 The addition of 100 ppb NO during oral breathing mimicked the effect of nasal breathing while moistened air during oral breathing had no effect.63 Intubated patients are deprived of the natural inhalation of endogenous upper airway NO. Supplementation of nasal air to intubated patients treated with a ventilator also improves arterial oxygenation and reduces pulmonary vascular resistance.65Moreover, Pinsky et al have shown that the hospital pressurised air may contain NO levels similar to those described above (6–500 ppb) which may consequently have effects on arterial oxygenation and pulmonary arterial pressure in mechanically ventilated patients.66 ,67 In a recent study nostril widening with a nasal tape improved arterial oxygenation in spontaneously breathing patients, probably by enhancing ventilation through the nasal airways thereby increasing the delivery of NO from the nasal airways to the lungs.68

Representative tracing showing transcutaneous oxygen tension in a healthy subject during periods of oral breathing (empty bars), nasal breathing (filled bar), or oral breathing of air containing exogenous NO at a concentration of 100 ppb (hatched bar). Reprinted from Lundberg et al63 with permission.
These results show that NO derived from the upper airways is capable of improving oxygen uptake and reducing pulmonary vascular resistance (fig3). It is tempting to speculate that the production of NO in the paranasal sinuses has the purpose of modulating lung function in humans. Since NO is produced above the bifurcation of the large airways this vasodilating gas will only affect pulmonary vessels in contact with ventilated alveoli, thereby improving ventilation/perfusion matching. This new physiological principle of NO as an airborne mediator may extend beyond vasodilation. Further studies will reveal whether inhalation of endogenous NO also has antimicrobial effects, upregulates ciliary motility, and inhibits platelet aggregation. If this is true the well known complications associated with long term intubation and ventilation, such as ciliary dysfunction and bacterial infections, may partly be explained by the lack of NO due to disruption of the natural low dose flushing of the lower airways by self-inhalation of endogenous NO from the upper airways.69

{kind=link}
{kind=link}
{kind=link}
Nitric oxide (NO) is released in the nasal airways in humans. During inspiration through the nose this NO will follow the airstream to the lower airways and the lungs. Nasally derived NO has been shown to increase arterial oxygen tension and reduce pulmonary vascular resistance, thereby acting as an airborne messenger.
Clinical value of nasal NO measurements
Measurements of nasal NO levels are attractive since they are completely non-invasive and can easily be performed even in small children. The finding of low nasal NO levels in patients with chronic sinus disorders such as Kartagener’s syndrome and cystic fibrosis are interesting.8 It is tempting to speculate that nasal NO measurements may be used to facilitate early diagnosis of these two respiratory disorders.
The possible usefulness of nasal NO measurements in the diagnosis and treatment monitoring of allergic rhinitis clearly needs to be further evaluated. If nasal NO is a reliable marker of local inflammation, this simple test may be used to monitor patients with rhinitis of different aetiology.
As mentioned above, intubated patients are deprived of inhaling the NO produced in the nasal airways. Considering the possible beneficial effects of nasal NO on pulmonary function, it is possible that replacement of nasal NO would be of benefit to patients being ventilated with an endotracheal tube.
It is reasonable to believe that drugs that affect endogenous NO synthesis will be used clinically in the future. These drugs may either facilitate or decrease NO production by, for example, interfering with different NOS. Measurement of nasal NO could be an interesting non-invasive means of monitoring the effects of such drugs and of optimising the dosage. The non-selective NOS inhibitorl-NMMA is currently being investigated for use in patients with sepsis. Interestingly, this inhibitor, when administered intravenously, leads to a dose dependent decrease in nasal NO levels.46 Conversely, systemic administration ofl-arginine increases nasal NO levels.16
Summary and future directions
Large amounts of NO are constantly being released in the nasal airways of humans and the paranasal sinuses seem to be the major source of this NO. Nasal NO may have important local as well as distal effects in, for example, host defence and regulation of pulmonary function.
The measurement of nasal NO levels may be helpful in further exploring the physiological and pathophysiological roles of this gas in the airways. Moreover, this simple test may be clinically useful in the diagnosis and treatment monitoring of certain respiratory disorders. To evaluate fully the potential of nasal NO measurements in the clinical setting it is important that we develop a standardised and reliable technique. We also need to know more about the different factors that affect nasal NO levels.