Article Text

Abstract
BACKGROUND Guidelines state that oral and inhaled corticosteroids are the cornerstone of asthma treatment. The effect of both types of treatment can be assessed by measuring lung and systemic parameters. Treatment for two weeks with either oral prednisolone (30 mg/day), high dose fluticasone propionate (2000 μg/day, FP2000), or lower dose FP (500 μg/day, FP500), both given by a dry powder inhaler, were compared.
METHODS One hundred and twenty patients with asthma were treated for two weeks in a double blind parallel group design. Lung function, asthma symptoms, airway hyperresponsiveness (PC20 methacholine and adenosine-5′-monophosphate), sputum eosinophil and eosinophilic cationic protein (ECP) levels were measured as lung parameters. In addition, morning serum blood cortisol, blood eosinophil, and serum ECP levels were measured as systemic parameters.
RESULTS PC20methacholine and adenosine-5′-monophosphate showed significantly greater improvement with FP2000 (1.99 and 4.04 doubling concentrations (DC), respectively) than prednisolone (0.90 DC, p = 0.02; 2.15 DC, p = 0.05) and marginally more than with FP500 (1.69 and 3.54 DC). Changes in sputum eosinophil and ECP concentrations showed similar trends; the decrease in ECP was significantly greater with FP2000 than with FP500. In contrast, the systemic parameters of steroid activity (cortisol, peripheral blood eosinophils, and serum ECP) decreased to a similar extent with FP2000 and prednisolone but significantly less with FP500.
CONCLUSIONS Oral prednisolone (30 mg/day) was inferior to FP2000 in improving airway hyperresponsiveness to both methacholine and AMP, with similar trends in forced expiratory volume in one second (FEV1), sputum eosinophil and ECP concentrations. Systemic effects were similar with prednisolone and FP2000 and less with FP500.
- asthma
- fluticasone
- prednisolone
- corticosteroids
Statistics from Altmetric.com
It is now well established that inflammation of the airway wall plays a central role in the pathophysiology of asthma. Corticosteroids are the cornerstone of anti-inflammatory treatment in asthma.1-4 Oral corticosteroids are generally considered to be the standard for airway anti-inflammatory and clinical effects, with only occasional patients having marked systemic effects.5 Inhaled corticosteroids produce fewer systemic effects and exert their benefit locally within the airways, although an effect on bone marrow has been suggested.6 Studies measuring the effects of oral prednisolone and/or inhaled corticosteroids on clinical parameters in asthma generally show a significant improvement in lung function, airway hyperresponsiveness, rescue medication, and symptoms after treatment periods ranging from one to eight weeks.7-12 Few studies have made direct comparisons between oral and inhaled corticosteroids as initial treatment11 ,13 or during asthma exacerbations.14 The results have generally shown comparable effects on clinical parameters.
It may be more sensitive to measure inflammatory markers in addition to clinical parameters when evaluating the efficacy of corticosteroids in the management of asthma. Induced sputum reflects the degree of local inflammation in the lung and is a promising tool for monitoring eosinophilic inflammation. Several studies have reported a decrease in the numbers of eosinophils and proteins derived from eosinophils—for example, eosinophil cationic protein (ECP)—after corticosteroid therapy.15 ,16 So far no study has looked simultaneously at the effects of prednisolone and inhaled corticosteroids on lung and systemic parameters in asthmatic patients. We have followed the dosages advised in the most recently published asthma guidelines at the start of treatment in patients with mild to moderately severe persistent asthma and have compared the effects of 30 mg oral prednisolone, the highest licensed dose of inhaled fluticasone propionate (FP) (2000 μg/day), and a lower dose of FP (500 μg) on lung and systemic parameters as initial treatment for a two week period in patients with asthma.1 ,17
Methods
PATIENTS
Patients aged 18–56 years with a diagnosis of asthma were included in the study if they met the following criteria: concentration of methacholine causing a 20% fall in FEV1(PC20) of ⩽8 mg/ml, at least one positive skin test to 17 most common aeroallergens, reversibility to β2 agonist ⩾9% of the predicted FEV1, and ability to expectorate sputum after hypertonic saline inhalation.
STUDY DESIGN
Inhaled corticosteroids were tapered and when possible discontinued completely at least three weeks before the randomisation visit. If patients experienced a worsening of their asthma before complete discontinuation of inhaled corticosteroids for three weeks they were asked to return to the hospital earlier for randomisation in the study. Patients who experienced an exacerbation of their asthma which required a course of treatment with prednisolone were not included. Randomisation was performed by a computerised minimisation method18 with stratification according to age, previous dose of inhaled corticosteroids, FEV1 %predicted, reversibility after 200 μg salbutamol, smoking status, serum IgE, and PC20methacholine. The study was of a double blind, three arm parallel group, double dummy design and lasted for two weeks. Patients received either oral prednisolone (30 mg/day), fluticasone propionate 2000 μg (FP2000), or fluticasone propionate 500 μg (FP500), both given by Diskhaler dry powder inhalation. Rescue medication consisted of salbutamol 400 μg via Diskhaler. No other concomitant pulmonary medication was allowed. Measurements at the start and the end of the two week treatment period were performed on two consecutive days at the same time in the morning. On the first day lung function, reversibility after salbutamol, blood sampling, and sputum induction were measured and on the second day airway hyperresponsiveness was measured by methacholine challenge. One hour after the final dose of methacholine a second challenge with adenosine-5′-monophosphate (AMP) was performed, an indirect marker of airway inflammation.19 ,20 Peak flow (PEF) (Mini Wright, UK), symptom score (range 0–3), and use of rescue medication were recorded every day in a diary.
The local medical ethics committee approved the study protocol and all participants gave written informed consent.
LUNG FUNCTION
FEV1 was measured with a calibrated water-sealed spirometer according to standardised guidelines.21 At least three reproducible values were obtained, the highest value being used for analysis. Methacholine and AMP provocation tests were performed by a two minute tidal breathing method. FEV1 was measured before and 20 minutes after 800 μg salbutamol given by Diskhaler to test reversibility.
INDUCED SPUTUM
Fifteen minutes after salbutamol inhalation (200 μg) hypertonic saline (3%, 4%, and 5%) was nebulised (Ultraneb 2000, DeVillbiss, Somerset, Pennsylvania, USA) for each concentration over seven minutes. The output of the nebuliser was calibrated at 1.5 ml/min. Subjects inhaled the hypertonic saline and were encouraged to cough and expectorate sputum into a sputum container. The weight of the induced sputum was measured. An equal volume of dithiothreitol 0.1% (Sputalysin 10%, Boehring Diagnostics Inc, Sommervillle, New York, USA) was added to the weight of the sputum. The sample was vortexed and placed in a shaking water bath at 37°C for 15 minutes and was filtered through a nylon (48 μm) gauze. A haematocytometer was used to count the total cell number, viability, and squamous epithelial contamination of the cell suspension. The sputum sample was centrifuged (10 min, 450g, 4°C) and the supernatant was frozen at –80°C for later analysis. The cell pellet was resuspended in phosphate buffered saline (PBS) and cytospins were stained with the May-Grünwald-Giemsa stain. At least 200 non-squamous cells were separately counted by three investigators blinded to the treatment code, mean cell differentials being presented.
BIOCHEMICAL ASSAYS
The concentrations of ECP in serum and sputum supernatant were measured using a fluoroenzyme assay (ImmunoCAP ECP, Pharmacia, Uppsala, Sweden). Blood cell counts were performed by flow cytometry and serum cortisol concentrations were measured using a radioimmunoassay.
STATISTICAL ANALYSIS
All calculations of PC20 were performed with the base-2 logarithm (log2) since this reflects doubling concentrations and normalises the distribution. Patients already responding to saline were assigned a PC20 value half of the lowest concentration applied. Patients not responding to the highest concentration of methacholine or AMP were assigned a value twice the highest concentration applied. According to the study design, patients who showed an increase in symptoms while tapering off their inhaled corticosteroids or who used no inhaled corticosteroids were randomised directly into the study. Incomplete diary cards for these two reasons occurred in 30 of the 118 evaluable patients prior to randomisation. Data from the diary cards were therefore analysed cross-sectionally only at the post-treatment visit and not as change from the randomisation visit. One way analysis of variance followed by Tukey’s pairwise multiple comparison tests in the case of significant overall effects were applied for normally distributed variables. For variables not normally distributed the Kruskal-Wallis test was employed, followed by Mann-Whitney U tests in the case of significant overall effects. Data are expressed as means with SE or medians with interquartile ranges. Skewedness of distributions were assessed with Kolmogorov-Smirnov tests, histograms, and Q-Q plots. Log transformation was applied where useful for normalisation. All analyses were performed with the SPSS version 7.5 package (SPSS-PC, Chicago, USA).
Results
Between September 1995 and July 1997 120 patients were enrolled into the study. Two of the 120 patients were not able to visit the hospital two weeks after start of the treatment (one pregnancy and one loss of study medication). The baseline characteristics of the 120 patients are presented in table 1; there were no significant differences between the three treatment groups.
Baseline characteristics of the patients
FEV1 increased in all three treatment groups with the trend for a smaller improvement with prednisolone (table 2, fig 1). Mean PC20 methacholine improved with all three treatments, the change with FP2000 (1.99 doubling concentrations (DC)) being significantly larger than with prednisolone (0.90 DC, p = 0.02). PC20 AMP also improved in all three groups and the improvement with FP2000 (4.04 DC) was significantly greater than with prednisolone (2.15 DC, p = 0.05, fig 2). PEF, symptom score, and use of rescue medication improved in all three treatment groups. Use of rescue medication was significantly lower with FP2000 and FP500 than with prednisolone (table 3).
Change in parameters in the three groups following two weeks of treatment

Change in FEV1 (% predicted) following treatment with prednisolone, fluticasone propionate 2000 μg/day and fluticasone 500μg/day. Data are expressed as medians with interquartile ranges. Bold horizontal lines indicate median change.

Change in PC20 doubling concentrations for methacholine (Mch) and AMP following treatment with prednisolone, fluticasone propionate 2000 μg/day, and fluticasone 500 μg/day. Data are expressed as mean (SE).
Diary card data after two weeks of treatment
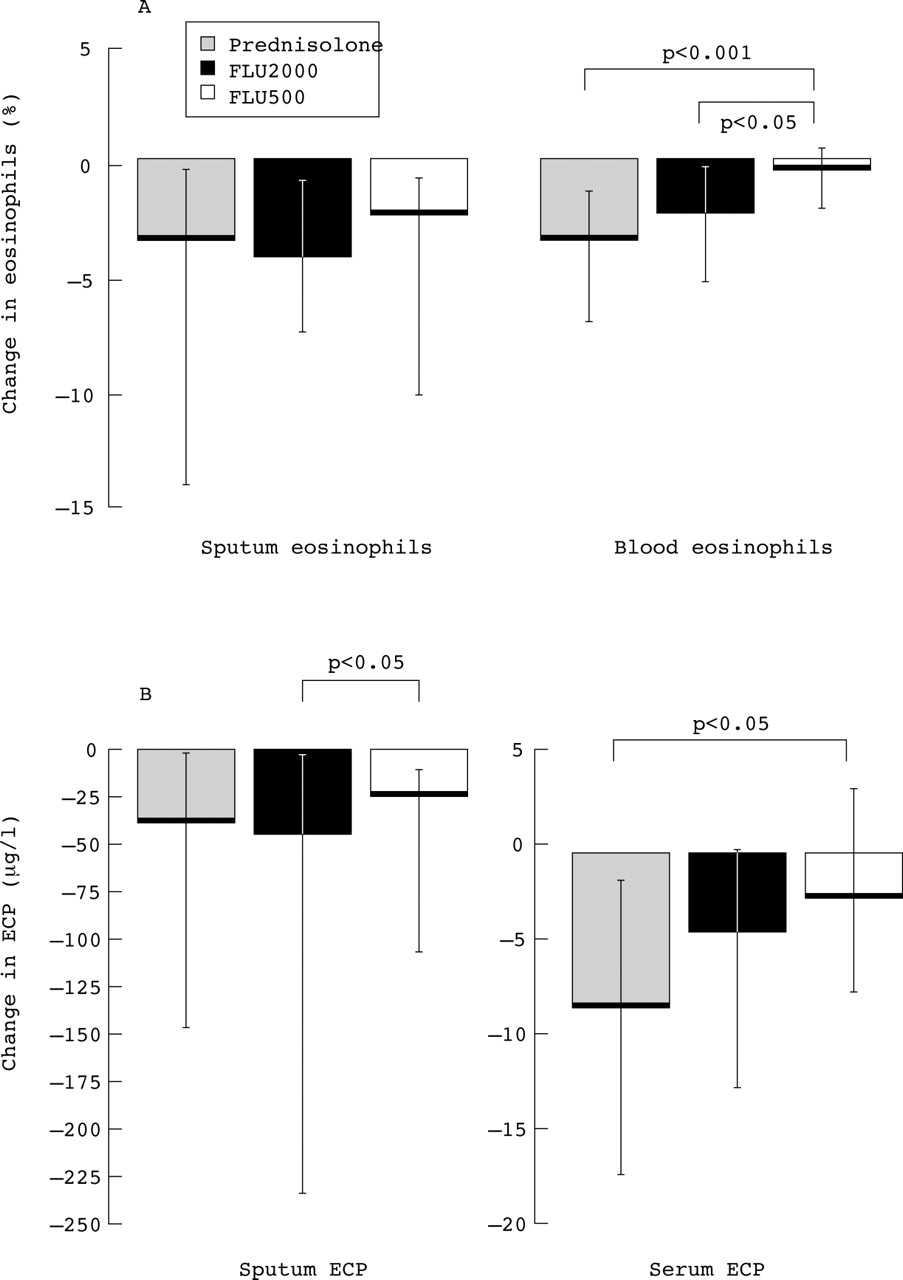
Eosinophils and ECP in induced sputum decreased significantly in all three groups (table 2). This decrease tended to be least with FP500 (fig 3). Blood levels of eosinophils and ECP did not change significantly with FP500 but prednisolone and FP2000 caused a significant decrease in both parameters. Blood eosinophils (p⩽0.001) and ECP (p = 0.02) decreased significantly more with prednisolone than with FP500, and more with FP2000 than with FP500 (p = 0.003; table 2, fig 3). Expressing ECP by the number of eosinophils showed the same differences between the treatment groups as described above. Morning serum cortisol levels were significantly more reduced with both prednisolone (28% reduction) and FP2000 (38% reduction) than with FP500 (0%) (fig 4). There was no significant difference between prednisolone and FP2000. In five patients in the prednisolone group and four in the FP2000 group the cortisol levels fell below the lower limit of normal values (100 nmol/l).

Change in sputum eosinophil and ECP levels and in blood eosinophils and serum ECP levels with prednisolone, fluticasone propionate 2000 μg and fluticasone 500 μg. Data are expressed as medians with interquartile ranges. Bold horizontal lines indicate median changes.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Change in serum cortisol levels with prednisolone, fluticasone 2000 μg and fluticasone 500 μg. Data are expressed as medians with interquartile ranges. Bold horizontal lines indicate median changes.
Discussion
This study in asthmatic patients showed that two weeks of treatment with high dose inhaled fluticasone (2000 μg) is more effective in improving PC20 methacholine and AMP than either 30 mg oral prednisolone or 500 μg fluticasone. In contrast, systemic parameters (blood eosinophils, serum ECP, and serum cortisol) decreased significantly more with oral prednisolone and fluticasone 2000 μg than with fluticasone 500 μg.
Several studies have reported improvements in airway hyperresponsiveness, FEV1, PEF, symptoms, and use of rescue medication after inhaled or oral corticosteroid treatment.7 ,8 ,11 ,13 ,15 ,22 ,23 The only available comparison of oral prednisolone and 2000 μg fluticasone during asthma exacerbations was made by Levy and coworkers14 who reported similar improvements in lung function, symptoms, and treatment success with both treatments. Airway hyperresponsiveness and inflammatory parameters in sputum and blood were not measured. We found a significantly greater reduction in airway hyperresponsiveness following two weeks treatment with fluticasone 2000 μg than with 30 mg prednisolone, which was true for both methacholine and AMP. However, the magnitude of change in doubling dilutions was more pronounced for AMP (4.04 and 2.15 DD for fluticasone 2000 μg and prednisolone, respectively) than for methacholine (1.99 and 0.90 DD, respectively, table 2). This difference between methacholine and AMP has been shown by other authors, suggesting that AMP responsiveness might be more sensitive to changes in airway inflammation than methacholine.20 ,24
In our study morning serum cortisol levels decreased significantly with both prednisolone (28%) and FP2000 (38%) but not with FP500. It is known that oral prednisolone has a cross reactivity with cortisol measurements (about 30% in our laboratory). When we corrected for this cross reactivity the cortisol suppression with prednisolone was 36% compared with 38% with FP2000, which does not alter the conclusion of similar suppression with prednisolone and FP2000 using the uncorrected data. In one study larger reductions in morning serum cortisol have been described after a single dose of FP2000 (58%) or a single dose of 50 mg prednisolone (87%).25 Other studies have reported smaller (48% and –134 nmol/l from baseline) but significant reductions in serum cortisol concentrations after treatment with 2000 μg/day fluticasone for periods of four days and three months, respectively.26 ,27 These reductions are comparable with our results. It has been suggested in one study that the suppressive effect of inhaled corticosteroids decreases somewhat after one year of treatment.28 It is known that fluticasone, when administered orally, is almost 99% metabolised in the liver29 without clinical or systemic effects. This suggests that the inhaled fluticasone that is absorbed from the lungs leads to a reduction in serum cortisol levels.7
We expected oral prednisolone and FP2000 to have the same clinical effect with oral prednisolone having a greater systemic effect. However, inhaled FP2000 was significantly more potent clinically than oral prednisolone while their systemic efficacy was equal. This could perhaps be explained by the differences in tissue penetration at the mucosal level, central and peripheral airways deposition, topical steroid potency, and half life. Our results are compatible with fluticasone having a better local effect than oral prednisolone in the epithelium and submucosa. The fact that the receptor affinity and half life of fluticasone are much higher than those of prednisolone and that tissue concentrations of fluticasone are markedly higher than serum concentrations support our hypothesis,30-32 but we are unaware of studies that have compared local tissue concentrations of prednisolone and fluticasone in the mucosa and submucosa. Finally, since it has recently been shown that asthmatic inflammation resides not only in the larger airways but also in the peripheral airways,33 differences between central and peripheral airway concentrations of prednisolone and fluticasone may also contribute to the more favourable clinical response to fluticasone. The high potency of fluticasone combined with high local concentrations in the peripheral airways, even when lower than in the central airways,30 would contribute to the possible difference.
Systemic inflammatory parameters (blood eosinophils and ECP) were not influenced by FP500 while FP2000 and prednisolone caused a significant decrease in both. This might suggest both a direct and indirect effect of FP2000 on blood parameters. The former consists of a reduction in airway inflammation resulting in lower levels of chemokines, cytokines, and a decreased attraction of blood eosinophils into the lung.34 Indirect effects of fluticasone—that is, after systemic absorption from the lung tissue—occur in peripheral blood and bone marrow with suppression of both progenitors of eosinophils in blood and of colony forming unit production in the bone marrow, both of which result in reduced numbers of blood eosinophils.6 ,35It is also known that inhalation of high doses of corticosteroids reduces the numbers of blood eosinophils by increased apoptosis.36
A dose of 2000 μg/day fluticasone is relatively high and has been equated to 4000 μg of conventional inhaled corticosteroids such as beclomethasone and budesonide.37 Further studies should therefore elucidate methods to determine the minimal effective doses of inhaled steroids after two weeks, preferably individualised to each patient. The present study in asthmatic patients shows that treatment with 2000 μg fluticasone is superior to oral prednisolone (30 mg/day). Two weeks inhalation of FP2000 provides a greater improvement in hyperresponsiveness than oral prednisolone in a dose of 30 mg/day) whereas their systemic effects tended to improve more with FP2000 (fig 3). It is still conceivable that higher doses of oral prednisolone (40–60 mg/day) would be comparable clinically to FP2000. However, this would also increase the systemic effects of prednisolone. We realise that FP2000 is much more expensive than oral prednisolone; nevertheless, a high dose of inhaled corticosteroids may be favoured over oral prednisolone because of its superior clinical efficacy in our study, and because of rare but severe side effects of oral prednisolone such as steroid induced diabetes.38 Our results are compatible with the advice of a 2–4 fold increase of inhaled corticosteroids in self-management of asthma exacerbations instead of treatment with oral prednisolone (30 mg/day). Such comparisons during exacerbations need to be further investigated.
Our findings are in contrast to statements in international guidelines1 ,3 in which oral prednisolone in a dose of 30 mg/day is regarded as “maximum therapy” for asthma control at the start of treatment. We found inhaled fluticasone in a dose of 2000 μg/day to be superior to oral prednisolone as initial treatment. A small dose response relation was seen on clinical parameters in favour of fluticasone in a dose of 2000 μg/day compared with 500 μg/day. However, the systemic effects of higher doses of inhaled fluticasone were also significantly greater.
Acknowledgments
The authors thank B Aalders, B Dijkhuizen, H Lange, D de Reus, M Swierenga-van der Veen, and J Zonderland for technical assistance. The study was funded by the University of Groningen, Glaxo Wellcome, Pharmacia-Upjohn, the Jan Cornelis de Cock Foundation, and the University Hospital Groningen.