Article Text

Abstract
Hospitalisations for acute exacerbations of COPD (AECOPD) carry significant morbidity and mortality. Respiratory viral infections (RVIs) are the most common cause of AECOPD and are associated with worse clinical outcomes. During the COVID-19 pandemic, public health measures, such as social distancing and universal masking, were originally implemented to reduce transmission of SARS-CoV-2; these public health measures were subsequently also observed to reduce transmission of other common circulating RVIs. In this study, we report a significant and sustained decrease in hospital admissions for all AECOPD as well as RVI-associated AECOPD, which coincided with the introduction of public health measures during the COVID-19 pandemic.
- COPD exacerbations
- viral infection
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
COPD is the third leading cause of global mortality.1 Preventive measures, including smoking cessation, pulmonary rehabilitation and vaccinations, are key strategies to reduce exacerbations and hospitalisations. Common respiratory viral infections (RVIs) are common triggers of acute exacerbations of COPD (AECOPD) and contribute significantly to hospitalisations.2 Thus reducing viral exacerbations can lead to improved outcomes in patients with COPD. In Singapore, various public health measures including hygiene reinforcement, social distancing and compulsory mask-wearing were implemented during the COVID-19 pandemic to reduce SARS-CoV-2 transmission. These measures were effective in mitigating community transmission of SARS-CoV-2 and in addition, other common circulating RVIs.3 We thus sought to assess if these measures would also potentially be associated with a reduction in hospitalisations for AECOPD, in particular exacerbations associated with common RVIs.
Methods
Anonymised epidemiological data on AECOPD admissions was obtained from our institution’s electronic database using discharge diagnosis codes. The total number of AECOPD admissions and the proportion of those admissions who tested positive for a concomitant RVI over a 6-month period during the COVID-19 pandemic (February 2020 to July 2020) were compared against a 2-year prepandemic period (January 2018 to January 2020). In clinical practice, patients presenting with clinical syndromes compatible with a viral exacerbation of COPD (eg, normal serum procalcitonin) were tested for common RVIs using a 16-target respiratory virus multiplex PCR assay (RV-16) on respiratory specimens, at the primary physician’s discretion. Trends in AECOPD admissions and the proportion of AECOPD admissions who were tested and had a PCR-positive RVI were compared in the prepandemic and pandemic periods, using t-test and χ2 test, respectively. The incidence of PCR-positive RVI among AECOPD admissions during the prepandemic and pandemic periods was compared using the incidence rate ratio method.
Results
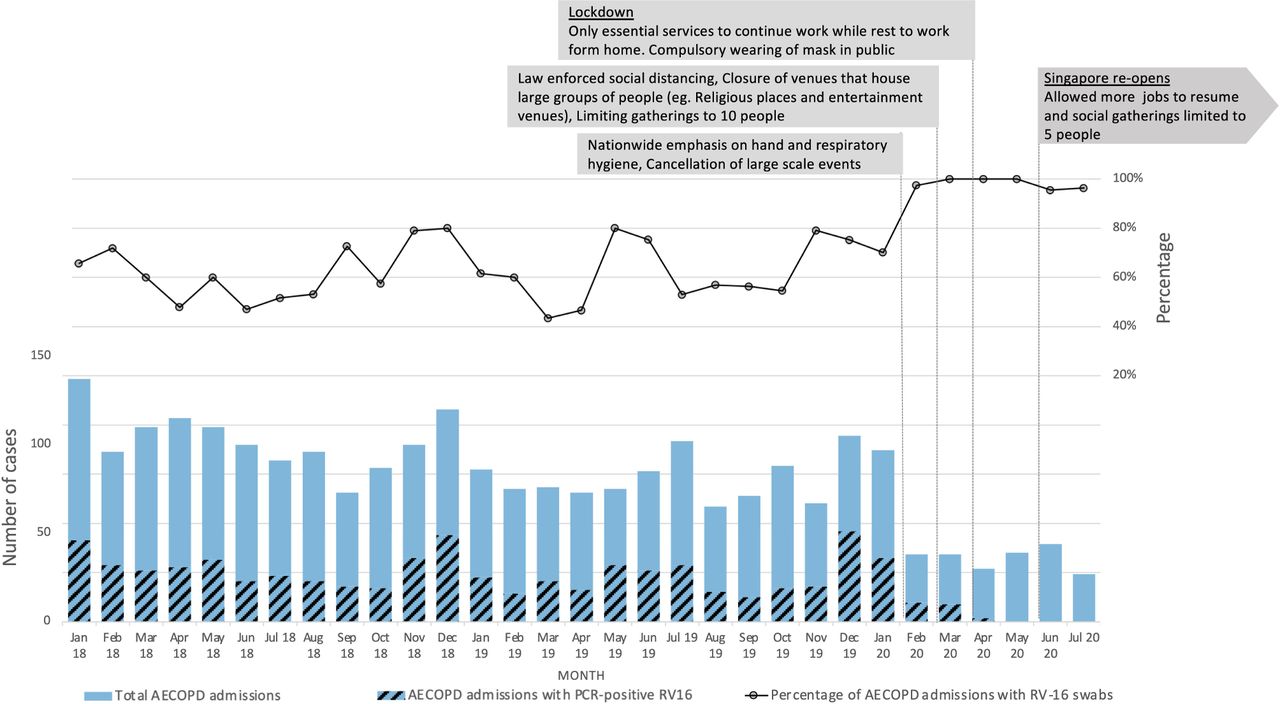
The introduction of public health measures during the COVID-19 pandemic coincided with a significant decrease in admissions for AECOPD over a sustained 6-month period, as well as a decrease in concomitant PCR-positive RVI-associated AECOPD admissions (figure 1). Prepandemic, our hospital saw an average of 92 (SD 18) AECOPD admissions per month; this decreased by more than 50% to 36 (SD 6) admissions per month during the pandemic period (February–July 2020) (p<0.001). During the pandemic, the proportion of AECOPD admissions tested for common RVIs increased substantially (prepandemic: 60% vs pandemic: 98%). Elevated vigilance for respiratory symptoms during the ongoing pandemic likely drove the increase in testing. Despite the substantial increase in testing, the incidence of PCR-positive RVI among AECOPD admissions dropped significantly during the pandemic period. The incidence rate of PCR-positive RVI was 106 cases per 1000 AECOPD admissions (23 cases, 216 admissions) during the pandemic, compared with 304 cases per 1000 AECOPD admissions prepandemic (701 cases, 2300 admissions); the decline was statistically significant (incidence rate ratio=0.35, 95% CI 0.22 to 0.53, p<0.001).
{kind=link}
Trend of AECOPD admissions and proportion with PCR-positive RV-16. Line graph depicts the percentage of AECOPD admissions tested for respiratory viruses.The standard respiratory virus multiplex panel (RV-16) at our institution included: respiratory syncytial virus A/B, influenza A/B, parainfluenza viruses 1–4, metapneumovirus, rhinovirus A/B/C, human coronovirus OC43/229E/NL63, adenovirus, human enterovirus, human bocavirus 1–4.
Prepandemic, close to half of AECOPD admissions tested had a PCR-positive RVI (48.8%, 701/1437). During the pandemic period, only 10.8% (23/212) of AECOPD admissions had a PCR-positive RVI; the decline was statistically significant (OR=7.8, 95% CI 5.0 to 12.8, p<0.001).
Discussion
According to the 2020 GOLD (Global Initiative for Chronic Obstructive Lung Disease) guidelines, COPD exacerbations associated with hospitalisations place patients in a more severe group. Frequent exacerbations lead to increased mortality, accelerated lung function decline and poor quality of life.4 Detection of a respiratory virus in respiratory specimens in both stable COPD and in AECOPD has been shown to be associated with worse clinical outcomes.5 6 As not all common RVIs are preventable with vaccines, simple public health measures to reduce community transmission of RVIs especially among vulnerable individuals may be important. The impetus for widespread adoption of public health measures, including social distancing and universal masking, during a pandemic provided a unique opportunity to observe the potential impact of such measures on AECOPD admissions. A significant decline in AECOPD admissions and incidence of PCR-positive RVI was observed over a 6-month period during the COVID-19 pandemic, coinciding with the introduction of these public health measures. Even after the nationwide lockdown was lifted from June 2020, our institution observed zero cases of COPD admissions with concomitant PCR-positive RVI, an observation unprecedented in the preceding 2 years of surveillance.
Our study’s limitations are as follows. It is possible that a reduction in admissions could be driven by a reluctance to present to hospital during the COVID-19 pandemic. Seasonality may also result in potential variations in RVI rates; however while seasonality is prominent in temperate countries, in a tropical country such as Singapore, seasonality is only observed for specific viral pathogens like influenza, and even then, does not follow the annual trend seen in temperate regions.7 The single-centre nature of our study may also preclude generalisability. In addition, only hospitalisations but not outpatient attendances were included. Nonetheless, hospitalisation episodes are more significant in the prognosis of patients with COPD, highlighting the value of our observation.
In conclusion, we report a significant reduction in AECOPD admissions and RVI-associated AECOPD admissions coinciding with the widespread adoption of public health measures during a pandemic. This reduction was sustained even after the reversal of community-wide lockdown measures. The complementary role of simple preventive measures such as wearing of face coverings, hand hygiene and social distancing in reducing AECOPD admissions deserves further investigation. These public health measures may have an important role in the postpandemic era, for population health outcomes especially for patients with COPD.
Footnotes
Contributors JYT had full access to all the data in the study and takes responsibility for the integrity of the data and accuracy of data analysis. Concept and design: LEIW, JYT, IV. Acquisition, analysis or interpretation of data: JYT, LEIW, EPC, Drafting of manuscript: JYT. Critical revision of manuscript for important intellectual content: LEIW, IV. Statistical analysis: JYT, EPC. Supervision: XYJS, IV.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.