Article Text

Abstract
We examined 4388 children from the 2003 to 2006 National Health and Nutrition Examination Survey and used survey-design-adjusted multivariable logistic regression to evaluate associations between dietary advanced glycation end product (AGE) and meat consumption frequencies and respiratory symptoms. Higher AGE intake was significantly associated with increased odds of wheezing (adjusted OR 1.18; 95% CI 1.02 to 1.36), wheeze-disrupted sleep (1.26; 95% CI 1.05 to 1.51) and exercise (1.34; 95% CI 1.08 to 1.67) and wheezing requiring prescription medication (1.35; 95% CI 1.13 to 1.63). Higher intake of non-seafood meats was associated with wheeze-disrupted sleep (2.32; 95% CI 1.11 to 4.82) and wheezing requiring prescription medication (2.23; 95% CI 1.10 to 4.54).
- asthma
- asthma epidemiology
- paediatric asthma
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Dietary advanced glycation end products (AGEs) are highly oxidant, proinflammatory compounds, with highest levels present in cooked meats.1 AGEs are ligands for the AGE receptor (RAGE), a pattern recognition and danger signal receptor, with highest expression in the lungs, and an important driving force behind downstream Th-2 inflammation.2 The relationship between AGEs and inflammatory airways disease is unclear.1 We investigated the effects of dietary AGE intake and meat consumption on respiratory symptoms within a paediatric cohort from the National Health and Nutrition Examination Survey (NHANES), a cross-sectional survey assessing the health and nutritional status of the US population.3
Methods
We included 4388 children aged 2–17 years from NHANES 2003–2006 (online supplemental figure S1), for whom data on dietary patterns (assessed by the 139-item Food Frequency Questionnaire (FFQ)), and respiratory symptoms were available. Only participants from NHANES 2003–2006 were included, as FFQ data were unavailable in other years. We calculated unitless meat consumption frequency scores using the FFQ, and AGE scores in keeping with prior published methodology (online supplemental appendix 1, online supplemental figure S2).4 The primary outcome was presence of wheezing over the past year; secondary outcomes included the presence of more specific wheezing symptoms (online supplemental table S1).
Supplemental material
Supplemental material
Supplemental material
The covariates age, sex, race/ethnicity, poverty to income ratio, body mass index (BMI) percentile, asthma status, total Healthy Eating Index (HEI) score and total caloric intake were collected from questionnaires. Survey logistic regression models were used to investigate associations between AGE and meat consumption scores, and dichotomised respiratory outcomes, adjusting for covariates. Interaction effects by age, sex, BMI percentile, asthma status and race/ethnicity were assessed, and total HEI score was removed from the multivariable model as a sensitivity analysis. Further analytical details are described in online supplemental appendix 1.
Results
Survey-weighted demographics of the 4388 paediatric participants are summarised in table 1, with 537 (13%) reporting wheezing in the past year (online supplemental table S2). In the adjusted models, higher AGE scores were significantly associated with increased odds of wheezing (OR 1.18; 95% CI 1.02 to 1.36), at least one sleep disturbance due to wheezing (OR 1.26; 95% CI 1.05 to 1.51), wheezing during exercise (OR 1.34; 95% CI 1.08 to 1.67) and wheezing requiring prescription medication (OR 1.35; 95% CI 1.13 to 1.63) in the past year (table 2).
Analytical population characteristics in relation to AGE intake
Associations between age scores and respiratory symptoms
There were no significant interactions by age (pint=0.46), sex (pint=0.31), BMI percentile (pint=0.73) or asthma status (pint=0.26), but a significant interaction effect for race (pint=0.04) (online supplemental appendix 2). Removing the total HEI score covariate from the main model did not significantly alter the associations between AGE intake and respiratory symptoms (data not shown).
We found a moderate but statistically significant positive correlation between AGE score and any non-seafood meat consumption (Pearson’s correlation coefficient of r=0.69, p<0.0001) (online supplemental figure S3), consistent with meats containing high amounts of AGEs.1 Higher consumption of non-seafood meat was associated with increased odds of wheezing requiring prescription medication (OR 2.23; 95% CI 1.10 to 4.54), and wheezing disrupting sleep (OR 2.32; 95% CI 1.11 to 4.82) (figure 1, online supplemental table S3).
Supplemental material
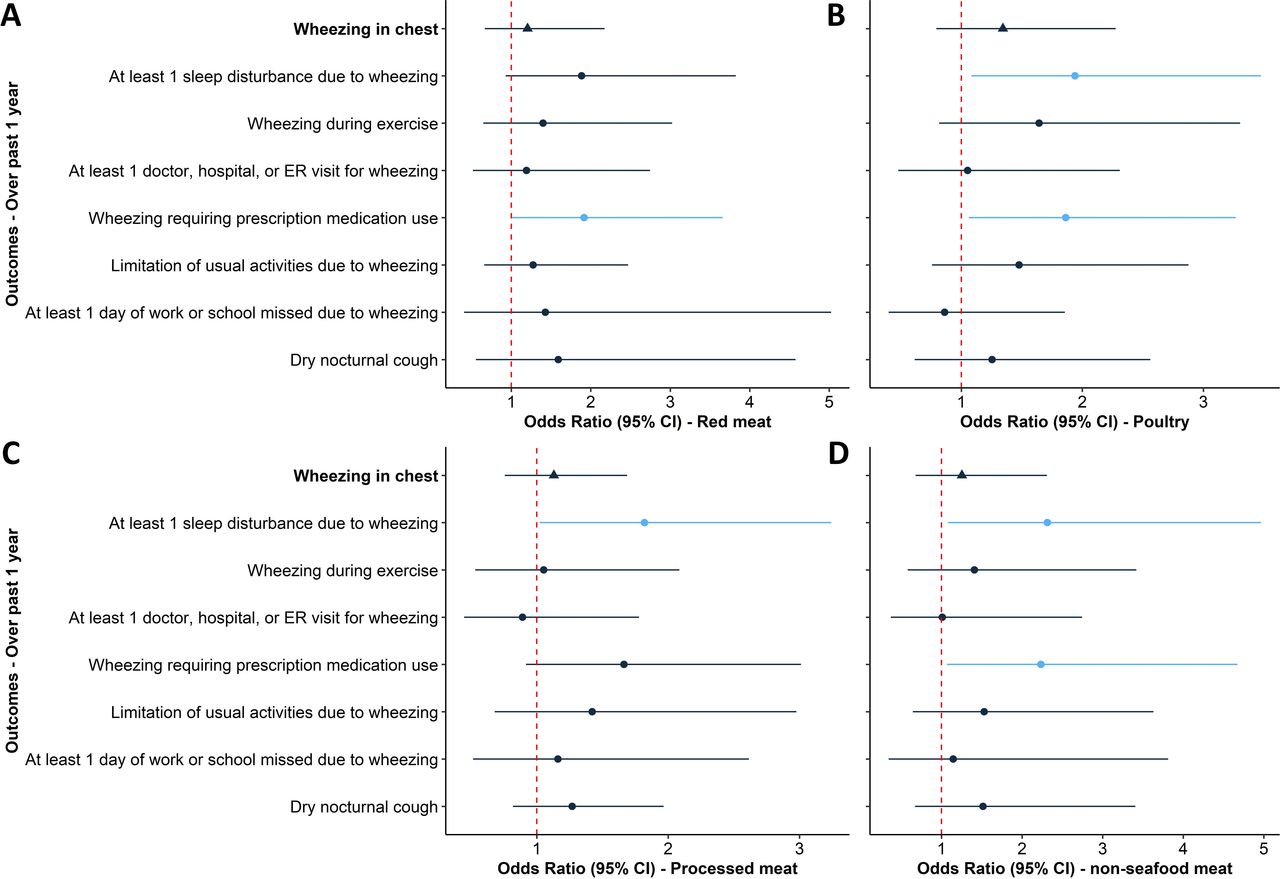
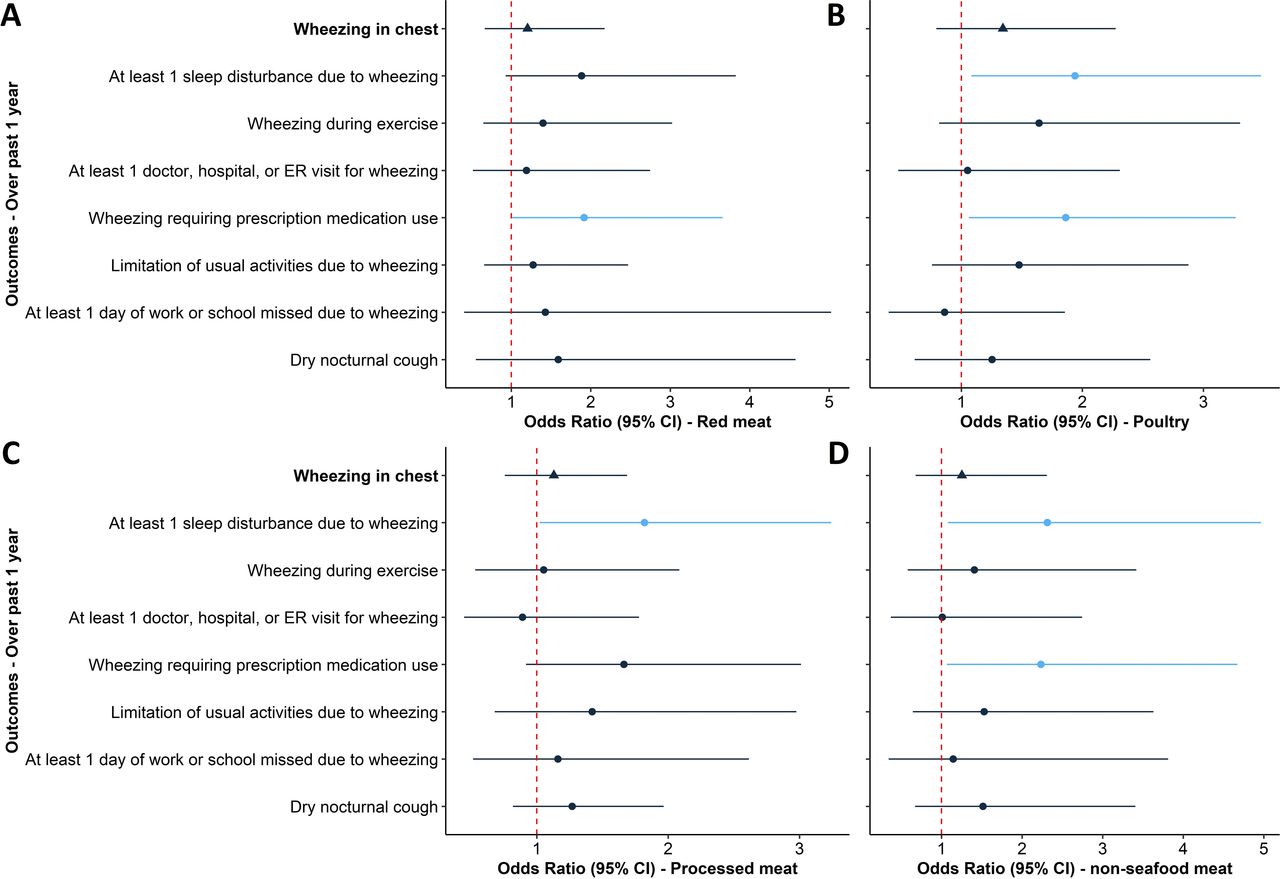{kind=link}
Associations between consumption scores for (A) red meat, (B) poultry, (C) processed meat and (D) any non-seafood meat (combination intake frequencies of red meat, poultry and processed meat) and respiratory symptoms, adjusted for age, sex, race/ethnicity, poverty to family income ratio, body mass index percentile, current asthma, total health eating index score and total caloric intake. ER, emergency room.
Discussion
To our knowledge, this is the first study in a national paediatric population demonstrating an association between dietary AGE intake and wheezing symptoms, including wheezing disruptive enough to interfere with exercise and sleep, and require prescription medication. Similarly, higher non-seafood meat consumption was associated with wheezing interfering with sleep and requiring prescription medication. Importantly, as non-seafood meats are a major dietary source of AGEs,1 our results suggest that a AGE-rich diet is adversely associated with childhood wheeze independent of overall diet quality.
Our results expand on current literature supporting a link between a proinflammatory dietary pattern and wheezing.4 5 The Western dietary pattern, characterised by increased consumption of AGE-rich foods, namely meats and saturated fats, may promote activation of the toll-like receptor 4 pathway and NF-κB inflammatory cascade, thereby contributing to airway inflammation and asthma pathogenesis.6 Additionally, a recent cohort study demonstrated that a pro-inflammatory diet measured by the Dietary Inflammatory Index, was associated with increased wheezing in atopic children.5 Conversely, the Mediterranean dietary pattern, characterised by lower consumption of saturated fatty acids and red meats, may have important anti-inflammatory effects, with one systematic review and meta-analysis demonstrating that adoption of a Mediterranean diet in children was associated with lower risk of wheezing symptoms and having ever had asthma.7 Finally, as several cohort studies have suggested an adverse effect of meat consumption on paediatric airways health,8 9 confirmation of a positive correlation between AGE intake and non-seafood meat consumption in our cohort strengthens our a priori hypothesis that dietary AGEs may have an important role in airway inflammation in children.
Biologic plausibility for our findings draws from emerging literature demonstrating that AGEs interact with RAGE, a critical modulator of type 2 cytokine signal transduction with a prominent role in allergic asthma pathogenesis.2 10 However, whether increased dietary AGE intake leads to overactivation and upregulation of RAGE-mediated airways inflammation remains unclear and warrants further exploration.
There are several limitations. First, causality cannot be implied due to the cross-sectional design, although these novel, hypothesis-generating findings provide a foundation for subsequent longitudinal studies to assess AGE intake as a modifiable dietary risk factor in the development of airways disease. Second, while there is no validated method of quantifying AGE consumption, AGE scores presented reasonably represent relative intake within our cohort, and associations between meat intake and wheezing were consistent with these findings. Finally, we recognise that the aetiology of wheezing may be highly variable in the wide age range of our cohort; however, we demonstrated no significant interaction effects by age.
In conclusion, higher dietary intake of AGEs, in part from non-seafood meat consumption, was associated with increased risk of clinically impactful wheezing in children. Further longitudinal studies examining the impact of dietary AGEs on airways disease in children are warranted.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @jing_gennieWang
Contributors JGW and SB took responsibility for the integrity of the data and accuracy of the analyses. SB, JGW and BL contributed to the conception of the study. BL, JGW and JU contributed to the data collection. BL, JGW, SC, FK, CH, AV and SB contributed to data analysis and interpretation. JGW and SB drafted the manuscript. All authors revised the manuscript for intellectual content and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests SC reports personal fees, equity and stock options from REnalytixAI, personal fees and stock options from pulseData and personal fees from CHF Solutions, Quark, Takeda, Janssen, Goldfinch, Relypsa and Bayer.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.