Article Text

Abstract
Background There is limited knowledge regarding the quality of dying and death (QODD) and end-of-life interventions in patients with interstitial lung disease (ILD). Hence, differences in QODD and end-of-life interventions between patients with ILD and those with lung cancer (LC) remain poorly understood.
Methods The primary aim of this study was to explore the differences in QODD and end-of-life interventions among patients dying with ILD versus those dying with LC. We performed a mail survey to quantify the QODD of a bereaved family’s perspective using the Good Death Inventory (GDI) score. Moreover, we examined the end-of-life interventions by medical chart review.
Results Of 361 consecutive patients analysed for end-of-life interventions, 167 patients whose bereaved families completed questionnaires were analysed for QODD. Patients with ILD had lower GDI scores for QODD than those with LC (p=0.04), particularly in domains related to ‘physical and psychological distress relief’ and ‘prognosis awareness and participation in decision making’ (p=0.02, respectively). In end-of-life interventions, patients with ILD were less likely to receive specialised palliative care services (8.5% vs 54.3%; p<0.001) and opioids (58.2% vs 73.4%; p=0.003). Additionally, lower frequencies of participation of patients with ILD in end-of-life discussion were also observed (40.8% vs 62.4%; p=0.007).
Conclusion Patients with ILD had lower QODD and poorer access to palliative care and decision making than those with LC. Additional efforts to improve QODD in patients with ILD, particularly in symptom relief and decision-making processes, are urgently warranted.
- interstitial fibrosis
- idiopathic pulmonary fibrosis
- palliative care
- lung cancer
Statistics from Altmetric.com
Key messages
What is the key question?
Are there differences in quality of dying and death (QODD) and end-of-life interventions between patients with interstitial lung disease (ILD) and those with lung cancer?
What is the bottom line?
Patients with ILD had lower QODD and poorer access to palliative care and decision making than those with lung cancer.
Why read on?
The present study highlights the necessary improvement to achieve a good death in patients with ILD.
Introduction
Interstitial lung diseases (ILDs) are progressive and incurable diseases that induce fibrotic destruction of the lung parenchyma.1 2 Among ILDs, idiopathic pulmonary fibrosis (IPF) is the most common form of fibrosing ILDs and has a worse prognosis than most malignancies, with a median survival of approximately 3 years from the time of diagnosis.2 ILDs are characterised by cough, fatigue, anxiety, depression and deteriorating breathlessness. Notably, patients with ILD often experience equivalent or more severe symptoms for longer periods versus those with cancer.3 4
Palliative care for non-malignant diseases, including ILD, has been attracting attention. However, palliative care remains underused in patients with ILD.5 Our group recently conducted a questionnaire survey for pulmonologists and reported that these specialists experience greater difficulty in providing palliative care for patients with IPF than for those with lung cancer (LC).6 Several unmet needs in palliative care for ILD have been proposed,7 but the quality of dying and death (QODD) and end-of-life interventions in clinical practice in patients with ILD have not been fully assessed yet, and the issues that need immediate improvement remain poorly understood.
This study was conducted to explore the differences in QODD and end-of-life interventions between patients with ILD and those with LC. The reason for the comparison with patients dying of LC was that an integrated model of palliative care is available for patients with cancer,8 and we expected that the comparison could provide a clinically interpretable insight.
Methods
We conducted the bereaved survey by sending self-reported questionnaires to the family members of decedents with ILD and those with LC in Japan. Additionally, we performed a medical chart review of consecutive decedents with ILD and those with LC. The bereaved survey measurements were linked to the same patient’s information obtained by medical chart review. Informed consent was based on the choice to opt out. We sent written explanations regarding this study to the bereaved family members via mail, and those who refused to participate were excluded from this study.
Setting
This multicentre study was conducted at four major acute general hospitals in the western part of Shizuoka Prefecture, Japan. Participating hospitals were regarded representative of the region, considering that they are four of the six general hospitals with ≥500 beds and a respiratory department in this geographical area: Hamamatsu University Hospital (613 beds), Seirei Mikatahara Hospital (934 beds), Seirei Hamamatsu Hospital (750 beds) and Iwata City Hospital (500 beds).
In Japan, palliative care focuses mainly on patients with cancer, and specialised inpatient units and hospital consultation services for inpatients and outpatients are available. All four participating hospitals have hospital consultation services, and Seirei Mikatahara Hospital has a 27-bed inpatient hospice (palliative care unit), which is usually provided to patients with cancer because it is covered under medical insurance for such patients. Moreover, home physicians provide specialised home services throughout the region for patients with and without cancer.
Subjects and procedures
The medical records of consecutive patients who died in the participating institutes from October 2015 to March 2019 were reviewed. We consecutively enrolled 400 pairs (200 with ILD and 200 with LC) of patients and family members (one family member per patient). The sample size was determined by the number of patients in the area during the study period. Inclusion criteria were as follows: (1) diagnosis of fibrosing ILD or LC (for patients diagnosed with both ILD and LC, the disease that resulted in death was determined by reviewing the medical records prior to conducting statistical analyses); (2) age >20 years; and (3) patients with family members aged >20 years. Exclusion criteria were as follows: (1) family members who lacked the capacity to complete the questionnaire (as a result of dementia, cognitive failure, psychiatric illness, language difficulty or vision loss) and (2) family members who had severe emotional distress determined by their primarily responsible physician. We sent questionnaires to bereaved family members via mail between October and November 2019 and requested them to complete and return the questionnaires to the study office within 1 month.
Outcomes
The outcome of most interest was QODD, as rated on the Good Death Inventory (GDI) (online supplemental table E1).9–11 The other outcomes of interest were symptom severity at the end of life, as rated on the Memorial Symptom Assessment Scale12 13; family-perceived quality of care (QOC), as rated on the Care Evaluation Scale (CES)14; end-of-life interventions, as per the medical records, and details of end-of-life discussion15; and the association between QODD and interventions (ie, palliative care access and the patient’s participation in end-of-life discussion). The details of each measurement are described in the online supplemental file.
Supplemental material
Statistical analysis
First, we compared the characteristics of the patients and their bereaved family between the two diagnostic groups. We used Fisher’s exact test for categorical variables and Student’s t-test or Mann-Whitney U test for quantitative variables as appropriate. Summary statistics were calculated as numbers (with percentages), median (with IQR) and mean (with SD) as appropriate.
Second, we tested the association of patient diagnosis with all the outcomes (symptom burden, QODD, QOC and end-of-life interventions) using Fisher’s exact test, Student’s t-test or Mann-Whitney U test as appropriate. P values adjusted for confounders of the association between patient diagnosis and outcomes were also calculated according to regression models: logistic regression models for categorical outcome variables and linear regression models for quantitative outcome variables. QODD and QOC were adjusted for patient’s age at death, patient’s sex, age of the family member, and relationship between the patient and the family, whereas the other outcomes were adjusted for patient’s age at death and patient’s sex. Because the incidence of missing values was very low for independent variables (for only one participant, information regarding the bereaved family member’s characteristics was missing), imputation was not performed. In comparing QODD and QOC between groups, we calculated the effect size (ES; Hedges’ g) to evaluate the degree of these differences. For interpretation, Hedges’ g values of 0.2, 0.5 and 0.8 were regarded as small, moderate and large differences, respectively.
Finally, we hypothesised that the implementation of specialised palliative care and patients’ participation in end-of-life discussions—which, according to a Swedish national population-based study, is lacking for patients with ILD4—may be associated with QODD in patients dying of ILD. This hypothesis is based on the empirical finding that these interventions were associated with a higher QODD in patients with cancer.16–19 We divided patients with ILD into three groups based on the presence or absence of palliative care access (ie, specialised palliative care services, opioid use or both) and their participation in end-of-life discussions: patients without both palliative care access and participation in end-of-life discussion (group A); patients with either palliative care access or participation in end-of-life discussion (group B); and patients with both palliative care access and participation in end-of-life discussion (group C). Each group was ranked according to the intensity of the interventions, and the Jonckheere-Terpstra trend test was performed to explore the associations between these interventions and GDI score. Each group was ranked as follows: group A=1; group B=2; and group C=3.
A two-sided test was used to determine significant differences, and the significance level was set at p<0.05. Adjustment for multiple testing was not conducted due to the exploratory nature of this study. All statistical analyses were performed using EZR V.1.51 (Saitama Medical Center, Jichi Medical University, Saitama, Japan) software.20
Results
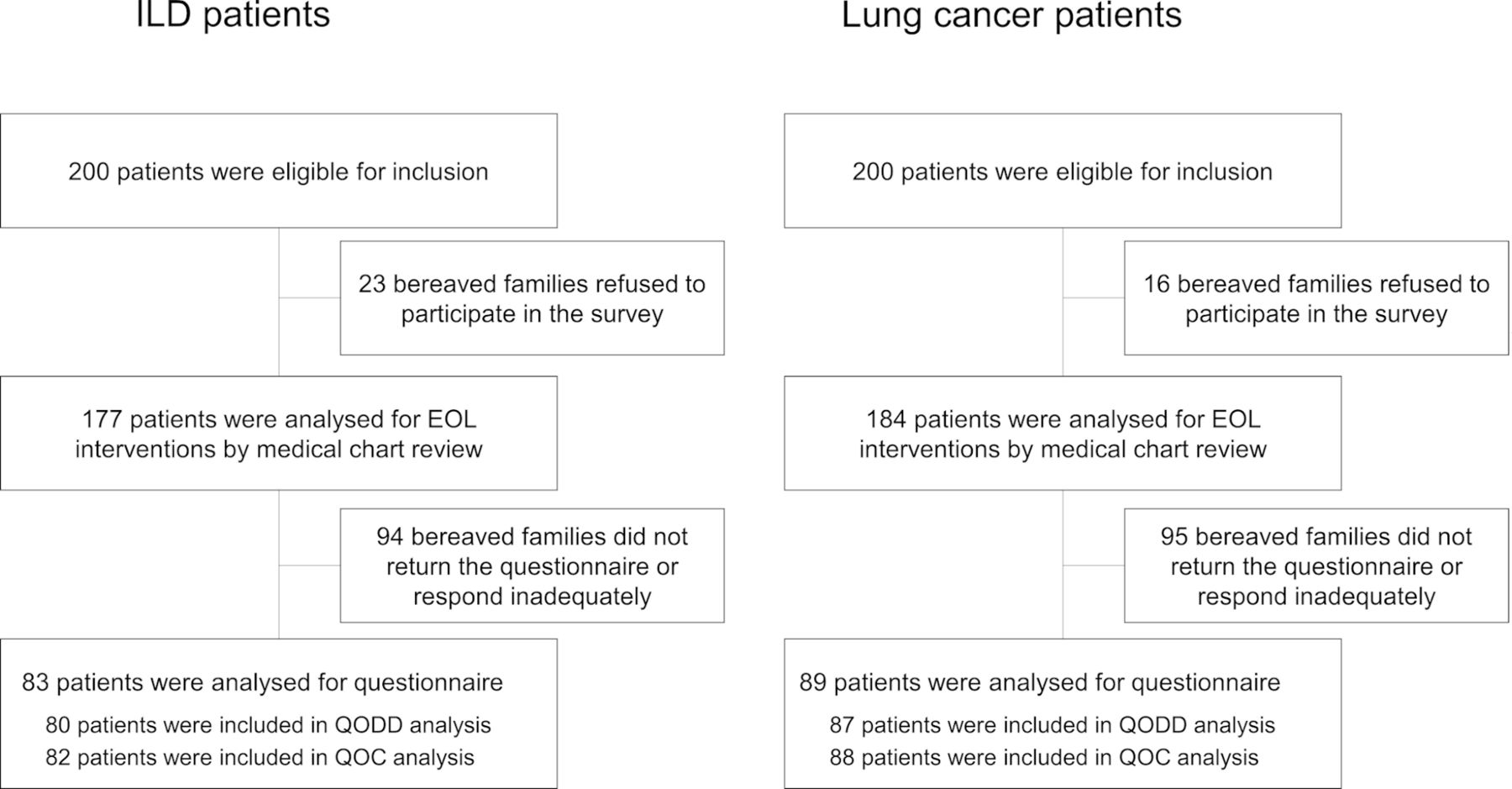
Among the 400 eligible pairs of patients and families, 39 families refused to participate in this study and 361 were included in the medical chart review survey: 177 with ILD and 184 with LC. Of these, 172 participants who responded adequately to the questionnaire were included in the bereaved questionnaire survey: 83 with ILD and 89 with LC. Because of missing data for the variable of interest, five participants were excluded from the QODD analysis and two were excluded from the QOC analysis (figure 1). The median time interval from patient death to survey participation was 19 months (IQR: 14–27 months).

Diagram of patient flow in the study. EOL, end of life; ILD, interstitial lung disease; QOC, quality of care; QODD, quality of dying and death.
Characteristics of patients and families
The baseline characteristics of patients at the time of last hospitalisation and the bereaved family members are shown in table 1. There were no differences found between the two groups in terms of age and sex. The frequency of long-term oxygen therapy usage was higher in patients with ILD versus those with LC (52.0% vs 15.5%; p<0.001). IPF was the most common type of ILD (44.1%), followed by idiopathic interstitial pneumonia excluding IPF (32.8%) and ILD associated with collagen tissue diseases (20.3%). More than half of the patients with ILD died due to acute exacerbations, and the median survival time from the time of diagnosis was 31 months (IQR: 6–61 months). Approximately half of the patients with LC had adenocarcinoma (50.8%), followed by squamous cell carcinoma (19.1%) and small cell carcinoma (13.7%). Most patients with LC (97.8%) died due to cancer progression, with a median survival of 11 months from the time of diagnosis. The characteristics of bereaved family members who responded to the questionnaires were similar between the two groups in terms of age, sex, relationship to patients and frequency of visits. There was no significant difference in the characteristics between patients who responded to the questionnaire and those who did not (ILD: online supplemental table E2; LC: online supplemental table E3).
Patients and bereaved family characteristics
Symptom burden at end of life
Symptom prevalence reported by bereaved families in both groups is shown in figure 2. Patients with ILD were more likely to experience breathlessness at the end of life than those with LC (94.8% vs 84.9%; p=0.043). Of note, the prevalence of the other six symptoms was similar between the two groups (figure 2A). Furthermore, patients with ILD had a significantly higher prevalence of very severe breathlessness than those with LC (55.8% vs 26.7%; p<0.001) (figure 2B).
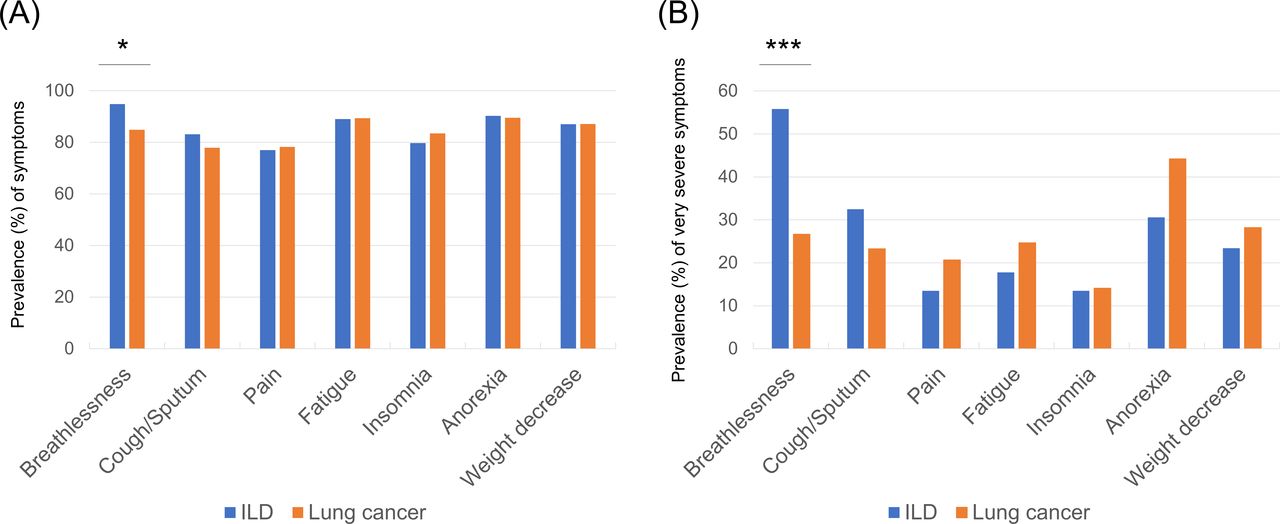
(A) Prevalence (%) of symptoms in ILD compared with lung cancer at end of life. (B) Prevalence (%) of very severe symptoms in ILD compared with lung cancer at end of life. *P<0.05, **P<0.01, ***P<0.001 (Fisher’s exact test). ILD, interstitial lung disease.
Quality of dying and death
Patients with ILD had a significantly lower mean GDI score for QODD than those with LC (4.33 vs 4.57; ES=−0.31; p=0.04) (online supplemental table E4). Domain scores according to groups are provided in figure 3. Among the domains, ‘physical and psychological comfort (domain related to physical and psychological distress relief)’ (3.99 vs 4.59; ES=−0.38; p=0.02), ‘environmental comfort (domain related to circumstances of the final place)’ (4.67 vs 5.09; ES=−0.31; p=0.048) and ‘control over the future (domain related to prognosis awareness and participation in decision making)’ (4.19 vs 4.71; ES=−0.35; p=0.02) were significantly lower in patients with ILD versus those with LC. These associations remained significant after adjustment for confounders.

Domain scores of quality of dying and death according to groups. Plots and error bars indicate mean and 95% CI. Scores in the quality of dying and death domains were measured using the Good Death Inventory. Scores range from 1 to 7 (higher scores indicate higher perceived quality of dying and death). *P<0.05 (Student’s t-test). ILD, interstitial lung disease.
Quality of care
The results for the QOC are presented in online supplemental table E5. Consistent with the findings for QODD, patients with ILD had a significantly lower mean CES score for QOC than those with LC (4.46 vs 4.72; ES=−0.37; p=0.02). Similar to the results obtained for QODD, the domains of ‘physical care by physician’, ‘psycho-existential care’, ‘physician’s explanation to the patient’ and ‘environment’ were significantly lower in patients with ILD versus those with LC (p<0.05 for all).
Interventions at end of life
The details of end-of-life interventions are summarised in table 2. Of those with ILD, 168 patients died in the general ward (94.9%), 8 died in the intensive care unit (4.5%), and only 1 patient died in an inpatient hospice (0.6%). In contrast, among those with LC, 67 patients (36.4%) died in an inpatient hospice and 117 died in the general ward (63.6%). The proportion of opioid administration at the last hospitalisation was significantly lower in patients with ILD versus those with LC (9.6% vs 32.1%; p<0.001). During the last hospitalisation, patients with ILD were significantly less likely to be referred to specialised palliative care services than those with LC (8.5% vs 54.3%; p<0.001). Blood tests and radiographs during the last 7 days of life were frequently performed in patients with ILD versus those with LC (thrice vs once weekly; p<0.001). Comparing the medical interventions performed during the last 2 days of life, patients with ILD were less likely to receive opioids (58.2% vs 73.4%; p=0.003). However, they were more likely to undergo treatment with steroids, antibiotics, blood transfusion, a large volume of infusion and life-prolonging procedures (eg, vasopressor agents, nasoenteric feeding, invasive mechanical ventilation and non-invasive ventilation) than those with LC. Fewer patients with ILD made a life-sustaining care decision at 48 hours prior to death than those with LC (72.3% vs 95.7%; p<0.001).
Interventions at end of life
End-of-life discussion
Details of the end-of-life discussion are summarised in table 3. Most cases in both groups had end-of-life discussion (91.6% vs 95.5%; p=0.36). However, patients with ILD were less likely to participate in end-of-life discussion than those with LC (40.8% vs 62.4%; p=0.007). Patients with ILD and their family members were more likely to discuss ‘resuscitation’ (66.7% vs 34.1%; p<0.001) and less likely to discuss ‘place of death’ (14.5% vs 57.3%; p<0.001). In most cases of ILD, end-of-life discussions were initiated by the pulmonologists in an inpatient setting. The first end-of-life discussion was held within 1 month of death in 44% of ILD cases.
Details of end-of-life discussion
Association of QODD with palliative care access and participation in end-of-life discussion
Patients with ILD were divided into the following three groups according to the presence or absence of palliative care access and end-of-life discussion participation: patients without both palliative care access and participation in end-of-life discussion (group A, n=36); patients with either palliative care access or participation in end-of-life discussion (group B, n=27); and patients with both palliative care access and participation in end-of-life discussion (group C, n=13). The GDI score in each group is summarised in figure 4. As the intensity of the interventions of interest increased, the GDI scores showed a significant monotonic increasing trend (p=0.03, according to the Jonckheere-Terpstra trend test); the GDI scores were the highest for group C (median: 4.65, IQR: 4.24–5.14), followed by group B (median: 4.50, IQR: 3.98–4.81) and group A (median: 4.06, IQR: 3.67–4.68).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Distribution of QODD in patients with ILD according to the presence or absence of palliative care access and EOLD participation. The upper and lower box sides represent 75th and 25th percentiles, respectively. The thick line indicates the median. QODD domains were measured using GDI. Scores range from 1 to 7 (higher scores indicate higher perceived quality of dying and death). EOLD, end-of-life discussion; GDI, Good Death Inventory; ILD, interstitial lung disease; PC, palliative care; QODD, quality of dying and death.
Discussion
To the best of our knowledge, this is the first study to explore in detail the differences in QODD and end-of-life interventions between patients with ILD and those with LC through a bereaved family survey and medical chart review. The bereaved family survey revealed that patients with ILD were more likely to suffer from very severe breathlessness and had a lower GDI score for QODD than those with LC, especially in domains related to ‘physical and psychological distress relief’ and ‘prognosis awareness and participation in decision making’. In end-of-life interventions, patients with ILD had poorer access to palliative care despite their distress. Additionally, for more than half of patients with ILD, end-of-life discussions were held in their absence. These findings suggest that patients with ILD face serious problems with symptom relief and decision-making processes.
Our study raised the issue of symptom relief in patients with ILD. In our cohort, patients with ILD were significantly less likely to receive opioids and specialised palliative care services than those with LC, despite experiencing severe breathlessness more often. Moreover, the bereaved family survey showed that the score of the domain related to ‘physical and psychological distress relief’ in patients with ILD was lower than that obtained for patients with LC. These results suggest that physicians may underestimate patients’ needs regarding palliative care, and patients with ILD do not experience sufficient relief from severe symptoms (eg, breathlessness and cough) before death. Severe breathlessness has been reported to be associated with a transition to the hospital at the end of life.21 Therefore, for patients with ILD who want to die at home, successful management of breathlessness may help fulfil their wishes.22 Notably, integrated palliative and respiratory care has been shown to improve breathlessness and has the potential to improve psychological outcomes and survival.23 24 Importantly, healthcare professionals caring for patients with ILD should make efforts to recognise palliative care needs and provide appropriate medical interventions.
Next, we found that patients with ILD were not involved in decision making at end-of-life planning. The present study revealed that more than half of patients with ILD did not participate in their end-of-life discussion. Additionally, patients with ILD had a higher frequency of undecided life-sustaining care plan until immediately prior to death than patients with LC. As a result, the score of the domain related to ‘prognosis awareness and participation in decision making’ of patients with ILD was lower than that of patients with LC. Several studies have reported that patients with ILD did not have sufficient discussion regarding their prognosis and had a poor understanding of disease behaviour at the end stages and their prognosis.25 26 Prognostication in patients with ILD is uncertain and more difficult than in patients with cancer. Especially, acute exacerbation, which was the most common cause of death in patients with ILD in our cohort, is life-threatening and unpredictable. These aspects would make it difficult for physicians to explain disease progression to patients with newly diagnosed or stable ILD. However, both patients with ILD and family members wished to receive more information from physicians.26 Therefore, sharing disease information, including disease behaviour and also ‘uncertainty in prognosis’, among physicians, patients and their families may increase understanding of ILD and awareness of prognosis and promote advance care planning.
Our study showed lower frequencies of ‘access to palliative care’ and ‘participation of patients themselves in end-of-life discussion’ in patients with ILD versus those with LC. These findings are generally consistent with previous reports,4 25 27 suggesting that implementing these interventions is an important concern for patients with ILD, regardless of region or culture. In patients with cancer, specialised palliative care referral has been associated with higher QODD.16 17 Additionally, patients with advanced cancer who participated in the decision-making process and had an awareness of the terminal illness had higher QODD than those who did not.18 19 Hence, we explored the association of QODD with palliative care access and participation in end-of-life discussion in patients with ILD. As expected, the implementation of these interventions was associated with higher QODD. Therefore, providing palliative care and promoting patient participation in end-of-life discussion may lead to improved QODD in this setting. A multidisciplinary team approach may assist in these efforts. Barratt and colleagues28 recently reported that a multidisciplinary team meeting among a palliative physician, a psychologist and an ILD specialist resulted in a significant increase in specialist palliative care referral and advance care planning discussions. Further investigation is warranted to examine the effectiveness of these measures and develop better interventions for patients with ILD and their family members.
This study has several mentionable limitations. First, the present study was conducted in a limited area of Japan, and the number of bereaved survey participants was relatively small. A nationwide survey should be conducted to confirm these results. Second, we enrolled patients who died in hospitals or inpatient hospices belonging to the hospitals and excluded those who died at home or a nursing facility. Thus, we could not exclude the potential for selection bias. However, most patients with ILD die in the hospital,29 30 and approximately 80% of patients terminally ill with cancer died in acute care hospitals in Japan,31 suggesting that this bias is unlikely to influence the conclusion. Third, there is bias associated with selection, recall, proxy and missing data in the bereavement survey. A careful interpretation after integrating other results is warranted. Fourth, medical records contain data that are only recorded by healthcare professionals. Recording practices may vary among different professionals, which could have influenced the findings. Fifth, although we tried to address confounding, residual bias might have influenced the findings. Sixth, there are some concerns about whether the comparisons with patients with LC were the best comparisons. A study comparing ILD with other diseases, such as COPD, whose clinical course is as difficult to predict as that of ILD, is warranted.
In conclusion, this study showed that patients with ILD had lower QODD than those with LC, and the domains related to ‘physical and psychological distress relief’ and ‘prognosis awareness and participation in decision making’ were especially lower. Patients with ILD had poorer access to palliative care despite their distress. Furthermore, patients with ILD had a lower frequency of patient participation in end-of-life discussions. These findings suggests that patients with ILD have insufficient distress relief and are not well informed. Therefore, more efforts to improve QODD in patients with ILD, particularly in symptom relief and the decision-making processes, are urgently required. Although further investigation is warranted, our study highlights the necessary improvement to achieve a good death in patients with ILD.
Acknowledgments
The authors would like to thank all the participants who participated in this study. The authors would like to thank Mariko Oishi, Hiromi Takeuchi, and Keiko Ohnaka for running the study office. The authors would like to thank Enago (www.enago.jp) for the English language review.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors TK: conception and design, data collection, data analysis and interpretation, and manuscript writing. YS, KS: conception and design, data analysis and interpretation, manuscript writing, and final approval of the manuscript. HH, MK, KF, TF, NE, YN, NI, KY, SI, HN: data collection, and data analysis and interpretation. TM: conception and design, data collection, and data analysis and interpretation. TS: manuscript writing, final approval of the manuscript and administrative support.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the ethics board of Hamamatsu University School of Medicine (approval number: 18-296), Seirei Hamamatsu Hospital (approval number: 3025), Seirei Mikatahara Hospital (approval number: 18-72) and Iwata City Hospital (approval number: 2019-001). The study procedures were carried out in accordance with the tenets of the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Participants of this study did not agree for their data to be shared publicly, so supporting data are not available.
Linked Articles
- Airwaves