Article Text

Abstract
Rationale The European Quality of Life 5-Dimensions 5-Levels questionnaire (EQ-5D-5L) is a multidimensional patient-reported questionnaire that supports calculation of quality-adjusted life-years. Our objectives were to demonstrate feasibility of use and to calculate the minimum important difference (MID) of the EQ-5D-5L and its associated visual analogue scale (EQ-VAS) in patients with fibrotic interstitial lung disease (ILD).
Methods Patients who completed the EQ-5D-5L were identified from the prospective multicentre CAnadian REgistry for Pulmonary Fibrosis. Validity, internal consistency and responsiveness of the EQ-5D-5L were assessed, followed by calculation of the MID for the EQ-5D-5L and EQ-VAS. Anchor-based methods used an unadjusted linear regression against pulmonary function tests (PFTs) and dyspnoea and other quality of life questionnaires. Distribution-based method used one-half SD and SE measurement (SEM) calculations.
Results 1816 patients were analysed, including 472 (26%) with idiopathic pulmonary fibrosis. EQ-5D-5L scores were strongly correlated with the dyspnoea and other quality of life questionnaires and weakly associated with PFTs. The estimated MID for EQ-5D-5L ranged from 0.0050 to 0.054 and from 0.078 to 0.095 for the anchor-based and distribution-based methods, respectively. The MID for EQ-VAS ranged from 0.5 to 5.0 and from 8.0 to 9.7 for the anchor-based and distribution-based methods. Findings were similar across ILD subtypes, sex and age.
Conclusion We used a large and diverse cohort of patients with a variety of fibrotic ILD subtypes to suggest validity and MID of both the EQ-5D-5L and EQ-VAS. These findings will assist in designing future clinical trials and supporting cost-effectiveness analyses of potential treatments for patients with fibrotic ILD.
- interstitial fibrosis
- health economist
Statistics from Altmetric.com
Key messages
What is the key question?
What is the minimum important difference (MID) of the European Quality of Life 5-Dimensions 5-Levels questionnaire (EQ-5D-5L) and visual analogue scale (EQ-VAS) in patients with fibrotic interstitial lung disease (ILD)?
What is the bottom line?
The MID of the EQ-5D-5L identified in this study for patients with ILD will help in the design of clinical trials and support cost-effectiveness analyses of potential therapies.
Why read on?
This study offers insight into the difference between disease-specific and generic health-related quality of life, as well as suggests the utility and describes the performance characteristics of the generic EQ-5D-5L health-related quality of life questionnaire in patients with ILD.
Introduction
Fibrotic interstitial lung diseases (ILDs) are progressive disorders that typically cause worsening dyspnoea and negatively impact health-related quality of life.1 Alleviating symptoms and improving health-related quality of life are the main goals in the management of fibrotic ILD given the high associated morbidity and mortality combined with the absence of curative treatment. Quality of life is thus an important patient-reported outcome in fibrotic ILD; however, there are many ways of measuring quality of life and no standard approach for patients with ILD.
The European Quality of Life 5-Dimensions 5-Levels questionnaire (EQ-5D-5L) is a frequently used patient-reported multidimensional measure of health that supports calculations of quality-adjusted life years (QALYs), which would allow for cost-effective analyses of ILD therapies.2 3 The EQ-5D-5L has been validated in the general Canadian population and in many other respiratory and non-respiratory diseases4–9; however, key performance characteristics remain uncertain in patients with fibrotic ILD. The minimum important difference (MID), defined as the minimum change that is important to patients, is an important threshold that can be used to evaluate the impact of therapy or quantify progression.10 Our objective was to calculate the MID for the EQ-5D-5L for fibrotic ILD based on data from a large prospective registry, with the overall goal that this will provide a useful measure for future clinical trials and cost-effectiveness analyses.
Methods
Study overview and study population
The CAnadian REgistry for Pulmonary Fibrosis (CARE-PF) is a prospective multicentre observational cohort study that was designed to evaluate the outcomes of patients with fibrotic ILD.11 At the time of this substudy, CARE-PF consisted of seven specialised ILD centres from the four most populated Canadian provinces, including British Columbia (two sites), Alberta, Ontario (two sites) and Quebec (two sites). Eligible patients had fibrotic ILD, were ≥18 years of age, provided informed consent and were able to complete questionnaires in English or French. Patients enrolled in CARE-PF were excluded from this substudy if they did not have an EQ-5D-5L measurement within 3 months of a pulmonary function test (PFT). ILD diagnoses were made at multidisciplinary conferences according to established guidelines where available.12 Patients were considered to have probable idiopathic pulmonary fibrosis (IPF) if they did not meet contemporaneous guideline criteria for IPF but were deemed to have IPF following multidisciplinary discussion.13 Patients without a clear diagnosis were labelled with unclassifiable ILD. All patients were enrolled between January 2015 and April 2018.
EQ-5D-5L measurement
The EQ-5D is a standardised preference-based health-related quality of life instrument that provides a measure of health status based on five dimensions that include mobility, self-care, usual activities, pain or discomfort, and anxiety or depression.14 There are two versions of the EQ-5D questionnaire: the EQ-5D-3L, which consists of three levels of severity within each dimension; and the newer EQ-5D-5L, which consists of five levels of severity within each dimension. We exclusively used the EQ-5D-5L questionnaire for this analysis because of its superior reliability and validity.15 Each dimension of the EQ-5D-5L is scored on a 5-point scale (range 1–5), corresponding to no problems, slight problems, moderate problems, severe problems and extreme problems. The scores obtained for each of these five dimensions are combined to form a 5-digit score, which is then converted into an index score based on set values obtained from a reference population.16 The index EQ-5D-5L score ranges from −0.148 to 0.949, from worst to best health state, with these values subsequently used to generate QALYs.16 The negative score indicates that some health states are considered worse than death.17 The EQ-5D-5L has been evaluated in other populations (eg, chronic obstructive pulmonary disease (COPD), cardiovascular disease, diabetes, cancer patients), showing validity and responsiveness as an outcome measure.4 5 8 9 The EQ-5D-5L also includes a vertical visual analogue scale (EQ-VAS), with participants asked to mark on the provided line or provide a whole number that represents how their health is today on a scale of 0–100. A higher number reflects a better quality of life for both the EQ-5D-5L and the EQ-VAS.
Additional measurements
Demographic data and smoking history were obtained from standardised patient-completed questionnaires as previously described.11 Additional measurements included health-related quality of life (St. George’s Respiratory Questionnaire (SGRQ))18 and dyspnoea (University of California at San Diego Shortness of Breath Questionnaire (UCSDSOBQ)).19 The SGRQ was derived and validated primarily in patients with obstructive lung disease, including three domains each scored from 0 to 100, with worse quality of life indicating higher scores.20 The UCSDSOBQ is a 24-item questionnaire that assesses severity of dyspnoea.19 21 Each question asks patients to rate their dyspnoea on a scale from 0 to 5, with 0 being ‘not at all’ and 5 being ‘maximal’, producing a total score that ranges from 0 to 120, with higher scores representing worse dyspnoea. PFTs, including forced vital capacity (FVC) and diffusing capacity of the lung for carbon monoxide (DLCO) and 6-minute walk distance (6MWD), were performed approximately every 6 months as clinically indicated.
Statistical analysis
Data are reported as mean±SD, median (IQR) or number (percent). All analyses were performed using RStudio V.1.1.456 (RStudio Team (2016). RStudio: Integrated Development for R. RStudio, Boston, Massachusetts, USA).
Validity of EQ-5D-5L
Validity of the EQ-5D-5L at baseline was assessed using Spearman’s correlations between both EQ-5D-5L and EQ-VAS scores with other health related quality of life assessments, dyspnoea and PFT measures. The strength of association was considered large if the Spearman’s correlation coefficient was >0.5, moderate if between 0.3 and 0.5, and small if between 0.1 and 0.3.22 Associations are presented as absolute r values (‘|r|’) given the varying direction of worsening for these measures (ie, worsening is indicated by an increasing score for some measures and decreasing score for others).
Internal consistency of the EQ-5D-5L
Internal consistency of the EQ-5D-5L at baseline was determined using the Cronbach’s alpha, which describes whether individual items of a questionnaire reflect the same underlying concept.23 The Cronbach’s alpha ranges from 0 to 1, with values between 0.70 and 0.95 considered acceptable internal consistency.23
Responsiveness of the EQ-5D-5L
Responsiveness analysis was performed to evaluate changes in both the index EQ-5D-5L and EQ-VAS at 6-month follow-up in patients with available longitudinal data (allowable range was 3–9 months to permit inclusion of patients with variable follow-up intervals). Patients were categorised into tertiles based on magnitude of change observed within the SGRQ, UCSDSOBQ, 6MWD, FVC and DLCO. The changes in index EQ-5D-5L and EQ-VAS among these tertiles were compared using a one-way analysis of variance.
Calculation of MID for EQ-5D-5L
Both anchor-based and distribution-based methods were used to calculate the MID for EQ-5D-5L and EQ-VAS using baseline values. The SGRQ, UCSDSOBQ, 6MWD, FVC%, and DLCO% were identified as potential anchors for the MID analysis based on their suggested MID values in the literature and their associated clinical utility. We used an MID range of 5–8 for SGRQ, 5–10 for UCSDSOBQ, 2%–6% for %-predicted FVC, 11% for %-predicted DLCO and 20.7 –35.4 m for 6MWD.20 24–27 Each anchor was included in the final analysis if it had at least moderate correlation with the EQ-5D-5L or EQ-VAS (ie, an r value >0.30). To determine the MID of the EQ-5D-5L, we first performed an unadjusted linear regression between the index EQ-5D-5L and the above described anchors, with the index EQ-5D-5L as the dependent variable. The range of corresponding MID for EQ-5D-5L was then generated from the corresponding regression equations based on the previously established MID values for the chosen anchors. The same calculations were repeated to generate MID values for the EQ-VAS. For the distribution-based method, we used the one-half baseline SD and one SE measurement (SEM) approaches for calculating the MID of the EQ-5D-5L and EQ-VAS.28 Analyses were repeated in subgroups of interest, stratifying patients by age, sex and ILD diagnosis.
Association between EQ-5D and mortality
Cox proportional hazard analysis was done using transplant as a competing risk between both baseline EQ-5D-5L and EQ-VAS values with mortality, reporting results per 0.1-unit change in EQ-5D-5L and per 10-unit change in EQ-VAS given the different scales of these measures. The same analysis was repeated for changes in EQ5D-5L and EQ-VAS values between baseline and 6-month follow-up with mortality.
Results
Patient characteristics
A total of 1816 patients with fibrotic ILD were included (table 1). Mean age of the cohort was 64±12 years old, 914 (50%) were male and 1108 (61%) were ever-smokers with a mean of 24 (8-36) pack-years among those who smoked. On average, patients had mild and moderate reduction in FVC and DLCO, respectively (74±20 and 57±20, respectively). A total of 665 (37%) patients had connective tissue disease (CTD)-associated ILD, 472 (26%) had IPF, 135 (7%) had hypersensitivity pneumonitis and 314 (17%) had unclassifiable ILD (online supplemental table E1). All other subtypes of fibrotic ILD made up 13% of the study population. Six-month follow-up data were available in 636 patients at the time of data export (online supplemental table E2). There were no substantial differences between this group and the remaining patients, with the lack of follow-up in most patients relating to the relatively recent enrolment of the study cohort.
Supplemental material
Baseline characteristics
Validity and internal consistency of the EQ-5D-5L
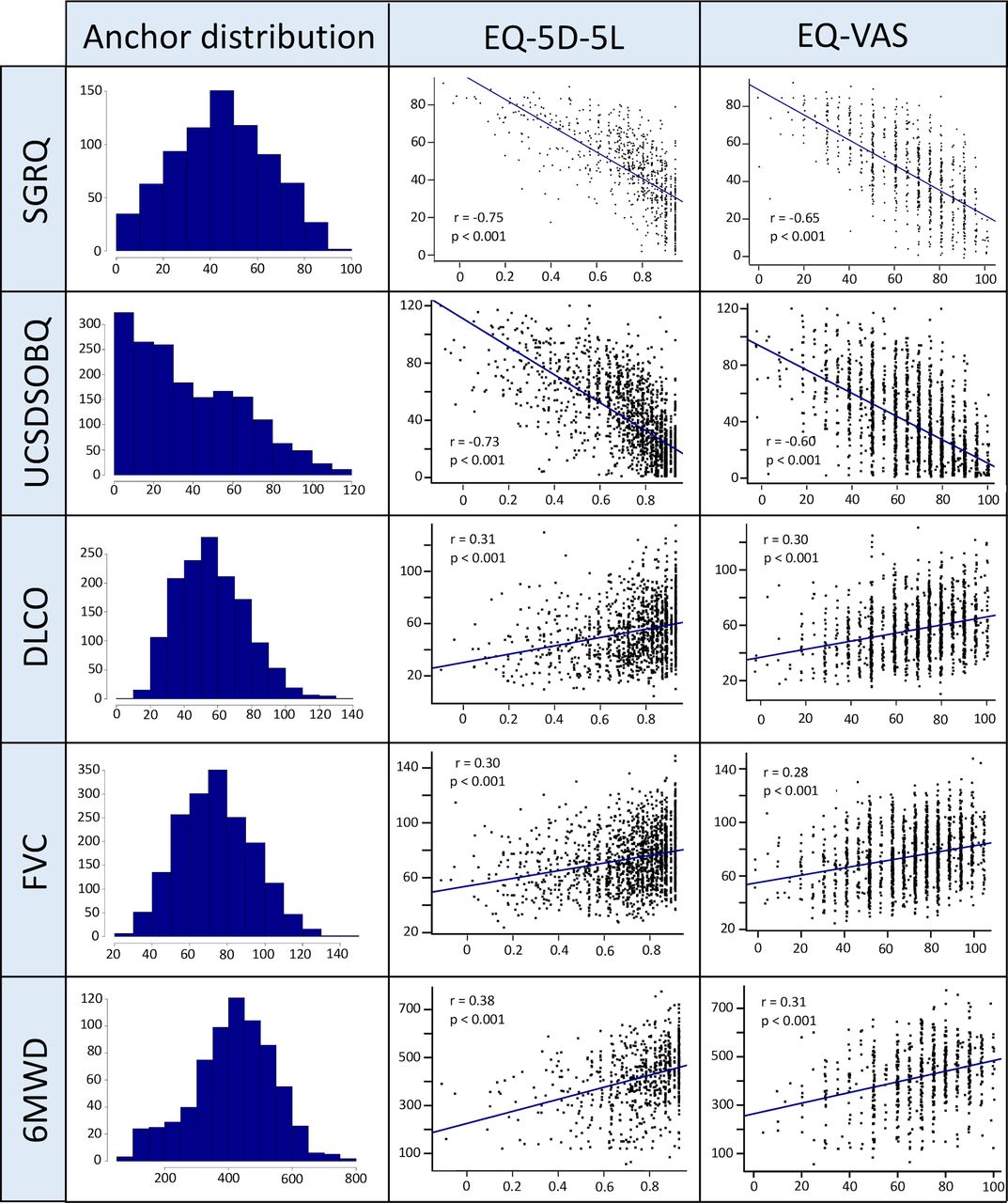
The r between EQ-5D-5L and EQ-VAS was 0.65. Both the EQ-5D-5L and the EQ-VAS had moderate-to-strong correlations with the SGRQ, UCSDSOBQ, DLCO and 6MWD, with |r| ranging from 0.30 to 0.75 (figures 1 and 2). The associations of EQ-5D-5L and EQ-VAS with FVC% were between weak and moderate, with r being 0.30 and 0.28, respectively. The internal consistency of EQ-5D-5L assessed by Cronbach’s alpha was 0.83, indicating acceptable internal consistency. Findings were similar in the IPF group, with Cronbach’s alpha values of 0.80. There were 340 patients (19%) with perfect scores of EQ-5D-5L at 0.949, which constitutes a significant ceiling effect.29 Within the subset of patients with perfect EQ-5D-5L scores, only 7% had perfect EQ-VAS scores and 1% had the lowest (best) SGRQ score. Patients with perfect EQ-5D-5L scores had a mean age of 65±12 years, FVC of 83%±19% and DLCO of 66%±19%. There were no patients with the worst EQ-5D-5L score, and thus no significant floor effect. There were no significant ceiling or floor effects for EQ-VAS.

Frequency distribution showing the number of patients for the European Quality of Life 5-Dimensions 5-Levels questionnaire (EQ-5D-5L) and European Quality of Life Visual Analogue Scale (EQ-VAS). CTD-ILD, connective tissue disease-associated ILD; EQ-5D-5L, European Quality of Life 5 Dimensions 5 Levels questionnaire; EQ-VAS, European Quality of Life visual analogue scale; ILD, interstitiallung disease; IPF, idiopathic pulmonary fibrosis.
{kind=link}
{kind=link}
Association of the EQ-5D-5L and EQ-VAS with selected anchors. DLCO, diffusing capacity of the lung for carbon monoxide; EQ-5D-5L, European Quality of Life 5-Dimensions 5-Levels questionnaire; EQ-VAS, European Quality of Life Visual Analogue Scale; FVC, forced vital capacity; SGRQ,St. George’s Respiratory Questionnaire; UCSDSOBQ, University of California, San Diego Shortness of Breath Questionnaire; 6MWD, 6-minute walk distance.
Responsiveness of the EQ-5D-5L
Patients with available longitudinal data were subcategorised into tertiles according to 6-month change in SGRQ, UCSDSOBQ, FVC, DLCO and 6MWD. Change in each anchor was in general alignment with the change in EQ-5D-5L for each tertile (table 2). Change in SGRQ and UCSDSOBQ varied significantly across tertiles of change for both EQ-5D-5L and EQ-VAS. There was less consistent difference across these same tertiles for FVC, DLCO and 6MWD. Results were similar comparing IPF and non-IPF subgroups, and in patients with CTD-ILD.
Change in anchors across tertiles of change in EQ-5D-5L over 6 months
Estimation of MID for EQ-5D-5L
Estimates of the MID for the EQ-5D-5L and EQ-VAS are provided in table 3. The anchor-based MID for the EQ-5D-5L ranged from 0.0050 to 0.054, depending on which anchor was used. The distribution-based MID for EQ-5D-5L was 0.095 according to the one-half SD method, and 0.078 according to the SEM method. Anchor-based MID values for EQ-VAS were between 0.5 and 5.0, depending on which anchor was used. The distribution-based MID for the EQ-VAS was 9.7 according to the one-half SD method, and 8.0 according to the SEM method. Findings were similar between IPF and non-IPF patients and in patients with CTD-ILD for all analyses (online supplemental tables E3 and E4). MID estimates were also similar comparing men to women and patients older and younger than the cohort’s median age.
Anchor-based and distribution-based estimates of the MID for EQ-5D-5L and EQ-VAS
Association between EQ-5D and mortality
Baseline EQ-5D-5L was strongly associated with mortality with a HR of 0.79 (p<0.001) per 0.1-unit of change in EQ-5D-5L with transplant as a competing risk. Baseline EQ-VAS was similarly associated with mortality with a HR of 0.78 (p<0.001) per 10-unit change in EQ-VAS. Although underpowered, the association of 6-month changes in EQ-5D-5L or EQ-VAS with mortality had similar direction of association (HR of 0.84 per 0.1-unit of change in EQ-5D-5L, p=0.11; HR of 0.97 per 10-unit change in EQ-VAS, p=0.7).
Discussion
There is no cure for fibrotic ILD, making health-related quality of life an important component of patient assessment. The EQ-5D-5L is a generic patient-reported quality of life questionnaire that has the advantage of translating into QALYs, which are critical in the cost-effectiveness assessment of new interventions and comparison of fibrotic ILD with other health states that is necessary to provide greater understanding of the health burden of fibrotic ILD. This prospective multicentre study of a large and diverse cohort of patients with fibrotic ILD suggests the validity of the EQ-5D-5L and provides a robust estimate of the MID for this population. These findings support the use of the EQ-5D-5L and EQ-VAS in future clinical trials and cost-effectiveness analyses in patients with fibrotic ILD, but with the limitation that there is a significant ceiling effect for the EQ-5D-5L that predominantly affected patients with milder disease.
Establishing an MID is useful as a benchmark target for an intervention, providing a general goal for patients and also allowing calculation of the number needed to treat. We used both anchor-based and distribution-based methods to estimate the MID for both the EQ-5D-5L and the EQ-VAS. As expected, the distribution-based approach provided higher values given its reliance on the distribution of data that often come from a heterogeneous population,10 while the anchor-based method likely provides a more clinically relevant MID. Also, as expected, the wide range in the anchor-based MID reflects the wide range for the reported MID in some of the anchors that were used, which may not reflect clinical practice. For example, a decline in FVC between 5% and 10% portends a worse prognosis and is generally accepted in clinical practice30; however, the accepted MID for FVC is between 2% and 6% in the literature, which is used in our analysis. For this reason, we place greater emphasis on the higher end of the MID range generated in our analysis. The MID for the EQ-5D-5L for COPD patients has previously been reported to be between 0.037 and 0.063,5 and between 0.034 and 0.049 for adults with type 2 diabetes.8 Our results are lower than both COPD and diabetes, with the MID for all of these diseases also being lower than the suggested population values (the MID for the EQ-5D-5L for Canadian population values is 0.045–0.06731), suggesting that a smaller change in quality of life is more important to patients with a chronic disease compared with the general public. These differences indicate the importance of establishing a disease-specific MID such that future clinical trials and cost-effectiveness analyses provide results that are appropriate for the target population.
Compared with disease-specific instruments, generic health-related quality of life questionnaires such as the EQ-5D-5L offer additional information by capturing not only the direct consequences of disease, but also adverse effects of treatments and the impact of the patients’ comorbidities.32 Generic instruments also enable comparison across different disease states, and support cost-effectiveness analyses that facilitate prioritisation of healthcare budgets based on relative benefits and costs of treatment. For example, although antifibrotic medications (pirfenidone and nintedanib) are clinically effective, there is less evidence that these are cost-effective when analysing generic health-related quality of life measures such as the EQ-5D-5L.3 This difference between therapeutic efficacy and cost-effectiveness highlights the need for a better understanding of generic health-related quality of life measures such as EQ-5D-5L. Most clinical trials in fibrotic ILD have focused on disease-specific quality of life questionnaires (eg, SGRQ, K-BILD), while clinicians, patients and other stakeholders instead place greater priority on a treatment’s overall impact on quality of life. This is an important consideration in the design of future trials.
We found that the EQ-5D-5L and EQ-VAS did not correlate strongly with either lung function or 6MWD, similar to what has previously been observed in other cohorts.25 33 Our longitudinal analysis examining tertiles of change similarly shows that patient-reported outcomes such as the SGRQ and UCSDSOBQ are associated with a corresponding change in EQ-5D-5L and EQ-VAS, while there was again weaker association with changes in objective measures of ILD severity. This finding was observed across all ILD subtypes, demonstrating that the lack of association between a generic quality of life instrument and measures of ILD severity was not driven by the presence of extrapulmonary manifestations in patients with CTD-ILD that impact quality of life while not typically affecting lung function. This relative disconnect between objective markers of ILD severity and a subjective measure of general health status indicates the need to assess both types of variables in order to gain a complete understanding of disease severity and progression.
Two large IPF registries have recently examined health-related quality of life in patients with ILD. The German INSIGHTS-IPF registry reported the association of health-related quality of life (both SGRQ and EQ-5D) with outcomes such as functional class, hospitalisations and use of long-term oxygen,34 while the Australian IPF Registry examined the correlation of SGRQ with dyspnoea and lung function.35 Our larger and more diverse ILD cohort showed similar associations of EQ-5D with dyspnoea and lung function, as well as with mortality. Consistent with the Australian IPF registry, we also found that health-related quality of life is more strongly associated with symptoms compared with objective pulmonary function measures. This finding highlights the obvious need for clinicians to focus patient discussions on common ILD symptoms rather than solely focusing conversations on objective pulmonary function measures that are also important factors in management decisions.
Although our study is based on a large Canadian multicentre cohort, all participating sites are specialised ILD referral clinics. Referral bias is thus a possibility; however, our consistent results across multiple ILD subtypes and patient subgroups in this large and diverse population alleviates much of this concern. MID estimates were also similar across different ILD subtypes, and comparing men to women, and older versus younger. The validation approach used in the statistical analysis for obtaining the MID for EQ-5D-5L and EQ-VAS focuses on convergent validation through strong correlation of EQ-5D-5L and EQ-VAS with other similar health-related quality of life measures, such as SGRQ and UCSDSOBQ. The statistically significant correlations of the EQ-5D-5L and EQ-VAS with mortality further strengthen the importance of applying subjective measures of health-related quality of life to patient management and future clinical trials. Even though we were underpowered to test the association of change in EQ-5D-5L or EQ-VAS with mortality, the direction of association was still consistent with what was expected.
Additional inherent limitations are the enrolment of patients from a single country and thus would benefit from further validation to document performance characteristics of the EQ-5D-5L and EQ-VAS in other potentially unique populations. We also lacked follow-up data for most patients in our cohort at the time of data analysis, and we were thus underpowered to evaluate the association of changes in EQ-5D-5L and EQ-VAS with mortality. However, our longitudinal analyses revealed expected findings and were still based on over 600 patients who had similar baseline features compared with the remaining patients. The significant ceiling effect seen in EQ-5D-5L suggests that it may not be a sensitive measure in mild disease; however, there was no ceiling effect for the EQ-VAS, suggesting this is likely a more robust measure for those with milder impairment in health-related quality of life.
In summary, we used a large and diverse cohort of patients with a variety of fibrotic ILD subtypes to suggest validity of both the EQ-5D-5L and the EQ-VAS and to determine their MIDs, with consistent findings among major ILD subtypes and other patient subgroups. We specifically found that the upper limit of the MID is 0.054 for the EQ-5D-5L index score and 5.0 for the EQ-VAS using an anchor-based approach. These findings will assist in the design of future clinical trials and support cost-effectiveness analyses of potential treatments for patients with fibrotic ILD.
Acknowledgments
CARE-PF is supported by Boehringer Ingelheim. The study sponsor had no input on the research question, study design, data analysis, interpretation of results or production of the manuscript.
References
Footnotes
Contributors Study conceptualisation and design: CJR and APYT. Data collection: all authors. Statistical analysis: APYT, SAH and CJR. Interpretation of results: all authors. Manuscript preparation: APYT, SAH, AWW and CJR. Approval of final version of the manuscript: all authors.
Funding CARE-PF is funded by Boehringer Ingelheim. Grant number 20R23666. The sponsor did not have input on any aspect of this work.
Competing interests CJR, MRJK, JM, KF, NH and DA report personal fees and grants from Boehringer Ingelheim and Hoffman La Roche outside the submitted work. HM reports grants from Boehringer Ingelheim. SS reports personal fees and grants from Boehringer Ingelheim and AstraZeneca Canada, and participation in clinical trials as site PI in Prometric Canada, Sanofi-Aventis, Gilead Pharmaceuticals, and Galapagos. KF also reports personal fees and grants from Theravance, Blade Therapeutics, Chest Foundation, University of Calgary School of Medicine, Pulmonary Fibrosis Society of Calgary, UCB Biopharma SPRL. NH also reports personal fees and grants from Actelion, Bayer and Novartis. MK also reports personal fees and grants from GSK, Gilead, Actelion, Respivert, Genoa, Alkermes, Pharmaxis, Prometric, Indalo and Third Pole. DA also reports personal fees and grants from Novartis. APYT, AW, SAH, GC, PGW, JF, MS, AG, CF, NK, AH and TT report no competing interests.
Patient consent for publication Not required.
Ethics approval The research ethics boards of all CARE-PF centres approved this substudy (coordinating centre: University of British Columbia and Providence Healthcare Research Ethics Board #H18-00993).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Deidentified participant data are available upon request from the corresponding author. Research Ethics Board and CARE-PF Steering Committee approvals are required before release of any data.