Article Text

Abstract
Objectives Up to 77% of patients with obstructive sleep apnoea (OSA) have positional OSA (POSA) but traditional positional therapy (PT) methods have failed as they were poorly tolerated. New convenient vibratory PT devices have been invented but while recent studies suggest high treatment efficacy and adherence, there are no published data comparing these devices directly with continuous positive airway pressure (CPAP). Our objective is to evaluate if a convenient vibratory PT device is non-inferior to CPAP in POSA treatment.
Methods In this crossover randomised controlled trial, we enrolled patients with POSA with significant daytime sleepiness (Epworth Sleepiness Scale (ESS)≥10). POSA diagnosis was based on: (1) total Apnoea/Hypopnoea Index (AHI)>10/hour and non-supine AHI<10/hour (2) supine AHI≥2 × non-supine AHI. Patients used their initial allocated devices (PT or CPAP) for 8 weeks before crossing to the alternative intervention after a 1 week washout. The primary aim is to measure changes in ESS between the two treatments. Secondary outcomes include sleep study parameters and patient treatment preference (ClinicalTrials.gov: NCT03125512).
Results 40 patients completed the trial between April 2017 and December 2018. Difference in ESS after 8 weeks of device use (PT minus CPAP) was 2.0 (95% CI 0.68 to 3.32), exceeding our predetermined non-inferiority margin of 1.5. AHI on CPAP was lower than with PT (4.0±3.2 vs 13.0±13.8 events/hour, respectively, p=0.001), although both were lower than at baseline. Time spent supine was significantly lower with PT than CPAP (p<0.001). 60% of patients preferred CPAP, 20% preferred PT, while 20% preferred neither device.
Conclusions The non-inferiority ESS endpoint for PT compared with CPAP was not met and the results were inconclusive. Future trials with larger sample sizes or in less symptomatic patients are warranted to provide further insight into the role of these new vibratory PT devices.
- sleep apnoea
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is the key question?
Can the promising new convenient vibratory positional therapy (PT) devices replace the poorly tolerated gold standard continuous positive airway pressure (CPAP) in positional obstructive sleep apnoea (POSA) treatment?
What is the bottom line?
The non-inferiority endpoint for PT compared with CPAP was not met in this study and the study results were inconclusive; CPAP was the preferred patient treatment choice primarily due to greater improvements in subjective symptoms.
Why read on?
This is the first published randomised controlled trial to compare a new vibratory PT device to the gold standard CPAP in the treatment of POSA, and the trial’s findings challenged the recent highly positive PT trials which suggested that these new devices may potentially change current practice and replace CPAP.
Introduction
Obstructive sleep apnoea (OSA) is a common sleep-related breathing disorder with an estimated prevalence as high as 38% in the general population.1 OSA is associated with significant daytime sleepiness that impair function and quality of life (QOL)2 and several health risks such as drug resistant hypertension,3 coronary artery disease,4 cardiac arrhythmias,5 stroke and sudden cardiac death.6 Continuous positive airway pressure (CPAP) has been the first-line OSA treatment for more than three decades but while its efficacy in obliterating upper airway obstruction is well established, patient treatment acceptance and adherence is low.7 Current alternative treatment modalities for OSA such as oral appliances8 and upper airway surgery9 are neither completely efficacious nor universally accepted by patients and evidence on their clinical outcomes is limited compared with CPAP. Thus, there is a need to search for an alternative, more acceptable and convenient OSA treatment modality which has comparable efficacy to CPAP.
Up to 77% of patients with OSA have ‘positional OSA’ (POSA) where obstructive respiratory events are reduced in a non-supine sleeping position.10–12 For these patients, positional therapy (PT) is an attractive strategy. PT refers to the avoidance of sleep in a supine position, which is typically the most detrimental sleeping position for OSA.13 The traditional PT method is the ‘tennis ball technique’ which involves sewing a tennis ball into the back of a shirt worn during sleep, so that the discomfort from lying on the tennis ball will force the patient into a non-supine position.14 However, despite being effective in reducing upper airway obstruction, the ‘tennis ball technique’ or its mimickers have failed as they were cumbersome and poorly tolerated.15
Recent technological advances have renewed interest in PT and more sophisticated PT devices have been invented in the past few years. These petite, neck or chest worn devices will vibrate with increasing intensity when a supine position is detected until the patient changes to a non-supine position. Preliminary studies have shown these new PT devices to be efficacious in reducing upper airway obstruction in patients with POSA.16–18 Better treatment adherence to these new PT devices compared with the traditional PT has also been observed.19 Additionally, these new PT devices have an advantage of being able to record usage information, thereby facilitating adherence monitoring.
However, there is currently no published randomised controlled trial (RCT) comparing these new PT devices head-to-head with the gold standard CPAP in the treatment of POSA. There are also paucity of data on clinical outcomes and patient treatment preference with these new PT devices. Hence, we conducted this study to compare a convenient PT device used for 8 weeks to CPAP used for 8 weeks in 40 patients with POSA in a crossover RCT. Our aim was to evaluate if PT was non-inferior to CPAP in the treatment of POSA.
Methods
Study design and subject recruitment
This is a crossover RCT conducted at Changi General Hospital, a 1000-bed teaching hospital in Singapore. Patients were recruited from sleep medicine clinics between April 2017 and August 2018 and final patient follow-up was completed in December 2018. Physicians provided a brief description of the study to eligible patients and enquired if they were keen to be contacted by the study’s research staff for further details. If a patient was agreeable to proceed with study participation after an appointment with the research staff, written informed consent was obtained.
Patient eligibility criteria included a diagnosis of POSA, age 21 years and above, an Epworth Sleepiness Scale (ESS) of 10–16 and no CPAP treatment or PT treatment for the past 6 months. The diagnosis of POSA was based on all following three criteria: (1) a full in-laboratory overnight polysomnography with total Apnoea/Hypopnoea Index (AHI)>10/hour and non-supine AHI<10/hour, (2) supine AHI greater than or equal to two times the non-supine AHI, (3) at least 15 min of supine and non-supine sleep. Patients were excluded if they had excessive daytime sleepiness (ESS≥17), were commercial drivers, unable or unwilling to use both treatments (CPAP and PT) or had concurrent use of therapy for OSA such as mandibular advancement splints. They were also excluded if they had uncontrolled severe medical conditions or conditions that precluded their ability to lie in a non-supine position. This study was approved by the Singhealth Centralised Institutional Review Board Ref: 2016/3154 (7 Feburuary 2017) and underwent trial registration (ClinicalTrials.gov: NCT03125512).
Study interventions, randomisation and masking
Patient recruitment was performed by the research team’s sleep physicians (AT and YM). After written informed consent was obtained, the patients were randomised by the hospital research unit to one of the study groups for their respective allocated treatment (CPAP then PT or PT then CPAP) according to a randomisation sequence that was generated a priori in random permutated blocks. The recruiting physicians (AT and YM) remained blinded to the randomisation sequence, scoring of the sleep studies, data analyses and study outcomes.
After randomisation, patients were asked to use their initial allocated devices nightly during sleep for 8 weeks. For CPAP therapy, patients were provided with Airsense 10 (Resmed) CPAP devices in the automated mode. The automated algorithm in the CPAP device allows CPAP pressures to vary according to the patient’s requirements during the night. Mask fitting and CPAP education was conducted by experienced sleep technologists prior to CPAP commencement. For PT, patients were provided with the Night Shift positional device which was recently approved by FDA in 2014 for the treatment of POSA. The Night Shift is a small, vibratory PT device that is worn at the back of the neck using a latex-free silicone rubber strap. When a supine position is detected, the device vibrates with increasing intensity until the subject changes to a non-supine position. Information recorded by the PT device includes usage hours each night, percentage of time in a non-supine position, sleep efficiency, frequency of awakenings and data can be stored for at least 4 months.
At the end of 8 weeks (Part 1), the patients underwent a Level 1 in-laboratory polysomnogram (PSG) with their respective device in situ (see figure 1). The sleep studies were scored in accordance with the American Academy of Sleep Medicine 2012 standard criteria.20 Subsequently, after a 1-week washout period, patients were crossed over to the alternative intervention arm for another 8 weeks (Part 2). After the second 8 week period, a Level 1 in-laboratory PSG was again performed with the allocated device in situ. Body position was initially recorded with a chest position sensor placed at the level of the mid sternum during the sleep study. The position recording was verified subsequently with video images by an unblinded assistant.

Trial flow diagram. CPAP, continuous positive airway pressure; ESS, Epworth Sleepiness Scale; OSA, obstructive sleep apnoea; PT, positional therapy.
A single experienced sleep technologist, who was blinded to patient treatment, performed the scoring of all PSG studies to decrease interobserver variability. As the montage (the set of sensor channels on display) of sleep studies performed with or without a CPAP device in situ appeared slightly different, the following measures were taken to ensure the scorer of the studies remained blinded: (1) The pressure flow channel of a sleep study montage performed with PT device was prospectively labelled as ‘Treatment flow’ during study acquisition, in order to resemble a study with CPAP in situ. (2) After the sleep studies were performed, an unblinded assistant removed the videos (after verifying body position) and the CPAP pressure channel in the studies performed with CPAP. The assistant therefore ensured all the sleep studies appeared similar in their montage before handing them over to be scored by the blinded sleep technologist.
Research staff assessing the outcomes of the study and data analyses were also blinded. Given the nature of the two interventions and crossover design of the trial, the patients, the medical staff performing the sleep studies at night, and clinical staff involved with administering or providing troubleshooting support for the two interventions could not be blinded.
Follow-up care and outcome assessments
As per routine clinical care for CPAP users, patients received a phone call at week 1 and week 3 after CPAP commencement to troubleshoot any CPAP mask or device problems. This might include simple advice over the phone or a face-to-face troubleshooting session at the CPAP clinic. Patients in the PT intervention arm also received a phone call at day 3, week 1 and week 3 of PT commencement to enquire on difficulties with device use. In addition, all patients were given the sleep laboratory number to call for any assistance. To enhance treatment adherence, patients were sent reminder messages on their mobile phones weekly as well as phone call reminders at week 1, week 3 and week 6 of Part 1 and Part 2 of the study respectively.
Patients completed questionnaires at randomisation and at the end of each 8-week period after device use. These questionnaires assessed the degree of daytime sleepiness, sleep quality, QOL and mood. At the end of the trial, patients were asked to state their treatment preference (CPAP, PT, no preference, neither). Adherence data were downloaded from both the CPAP and PT devices after each 8week period.
Outcomes
The primary outcome was the difference in sleepiness measured by the ESS after 8 weeks of device use. Secondary outcomes included the difference in QOL indices (Functional Outcomes of Sleep Questionnaire (FOSQ) and 36-item Short Form survey (SF-36)), sleep quality (Pittsburgh Sleep Quality Index (PSQI)), mood symptoms (Depression Anxiety Stress Scale 21 (DASS21)), treatment adherence after 8 weeks of device use and patient treatment preference. Sleep study parameters such as AHI and oxygen indices during the sleep studies conducted after 8 weeks of device use were also compared.
Sample size estimation and statistical analysis
Sample size calculation was based on another trial21 where the SD of the difference in ESS between two positional training devices was calculated to be 3.5 (difference between interventions 0.6, p=0.393, n=26). Based on clinical judgement, the minimally clinically significant change in ESS was determined to be 1.5. Hence, using a non-inferiority margin of 1.5 for the ESS, with 80% power and one-tailed significance of 0.05, 36 patients were needed to complete this crossover trial. Allowing for dropouts, we targeted a recruitment of 40 patients. Dropouts were replaced when time and resource permitted.
The primary analysis was conducted by intention to treat. The primary outcome of the difference in ESS after 8 weeks of PT therapy versus CPAP therapy was analysed using linear mixed effects model. The model included fixed effects for intervention (PT or CPAP), order (PT first or CPAP first), the intervention-by-order interaction and potential confounders such as patients’ demographics and baseline ESS. Other outcomes such as the difference in PSQI, FOSQ, SF-36, DASS, treatment adherence, sleep study parameters of AHI and oxygen indices were compared using similar mixed models. A two tailed, p<0.05 was considered statistically significant. Continuous variables were presented as means with 95% CI limits while categorical variables were presented as numbers and percentages. Statistical analysis was performed using SPSS V.19.0 (IBM, Armonk, New York, USA).
Results
Study participants
A total of 41 patients were enrolled and 40 patients completed the study (figure 1). One patient randomised to start PT therapy first withdrew after 5 weeks as he wished to proceed with CPAP treatment and declined further participation in the study. This dropout was replaced, and the additional patient was randomised into the arm commencing with CPAP treatment. Five patients did not have sleep studies performed; four had personal reasons while one was unable to continue PT after developing neck pain. All five patients were willing to continue with all other aspects of the study protocol and completed participation. The target sample size of 40 was achieved and final analysis was performed on all 40 patients who completed the study.
Patient baseline characteristics are shown in table 1. The patient group was predominantly male (72.5%) with a mean age of 44 years. The mean body mass index (BMI) was 26.1 kg/m2, mean ESS was 12.1, mean AHI was 23.4 events/hour and the main ethnicity was Chinese (72.5%).
Baseline characteristics of patients (n=40)
Primary outcome of ESS
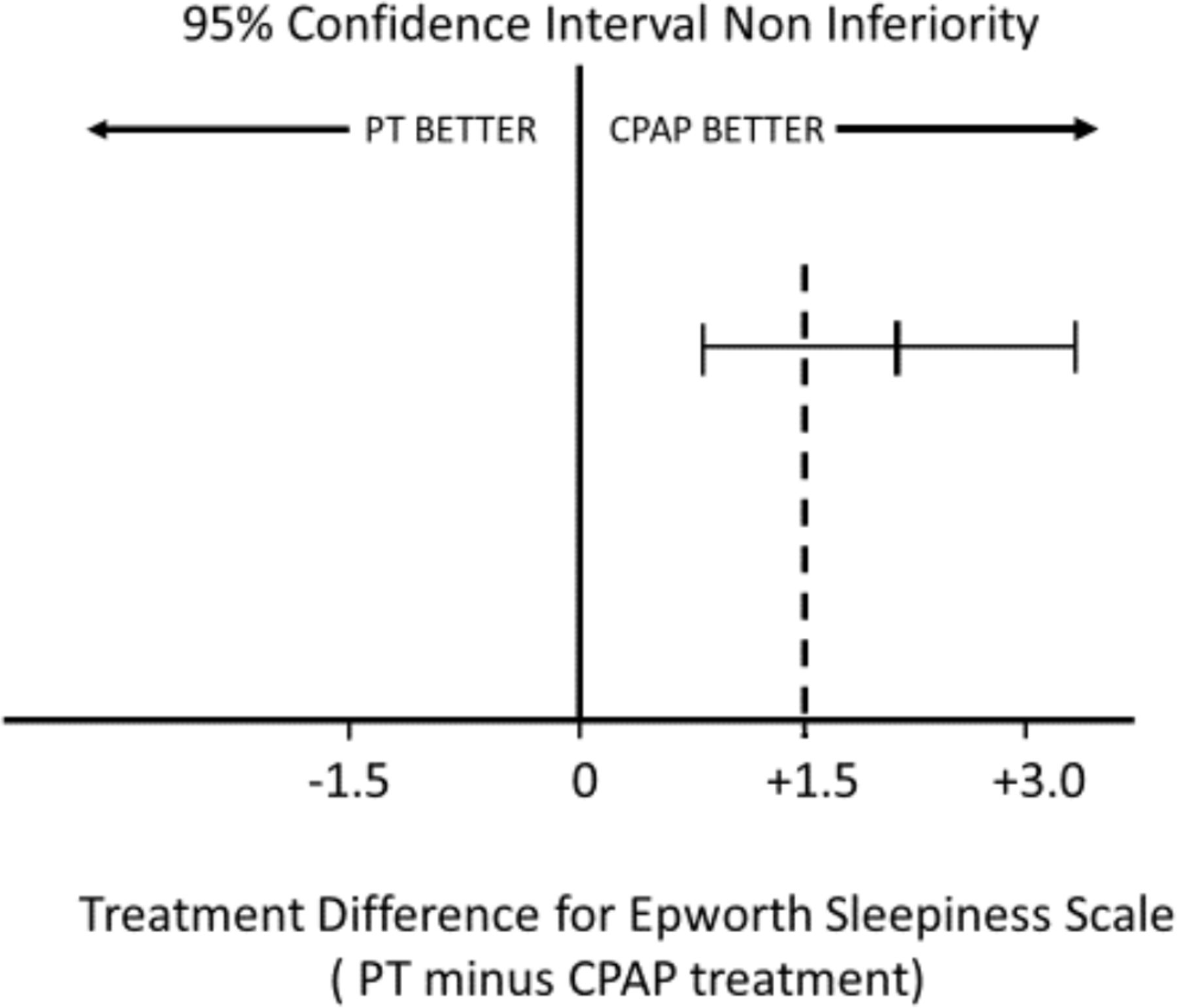
The difference in ESS score after 8 weeks of device use (PT minus CPAP) was found to be 2.0 (95% CI 0.68 to 3.32). The post-CPAP arm and post-PT arm had a mean ESS of 8.9±4.5 and 10.9±4.0, respectively. The adjusted difference in ESS between PT and CPAP was 2.28 (95% CI 0.96 to 3.61), after adjusting for gender, age, race, BMI, randomisation sequence, baseline ESS, baseline AHI, device’s adherence and device*randomisation sequence (figure 2).
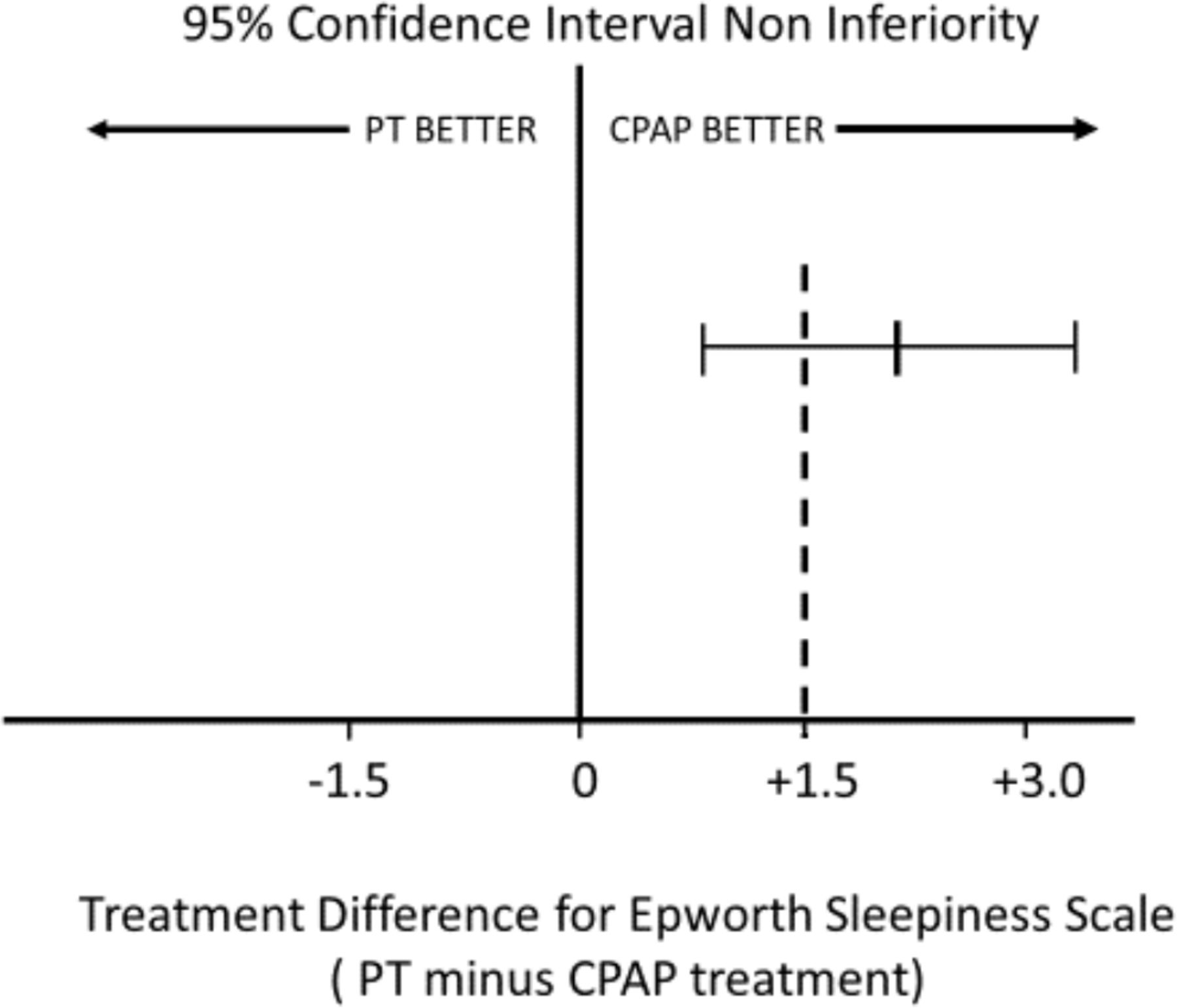
Graph demonstrating that the non-inferiority endpoint of ESS for PT was not met. The criteria for non-inferiority would be met if the mean difference in ESS and its 95% CIs lay to the left of the non-inferiority margin of +1.5. CPAP, continuous positive airway pressure; ESS, Epworth Sleepiness Scale; PT, positional therapy.
Secondary outcomes
Sleep study parameters
CPAP was more efficacious in controlling obstructive respiratory events, as demonstrated by the AHI on CPAP being significantly lower than with PT, although both were lower than at baseline. Correspondingly, oxygen indices such as the oxygen desaturation index was lower, and lowest oxygen saturation (SpO2) was significantly higher with CPAP compared with PT. As expected, time spent supine was significantly lower with PT than CPAP (table 2).
Sleep study parameters between CPAP and PT
Sleep quality, quality of life and mood indices
No significant difference was seen in sleep quality between PT and CPAP treatment as measured by the PSQI questionnaire. In the QOL assessment by SF36, only the subcategory of ‘energy/fatigue’ demonstrated a statistically significant difference between PT and CPAP, with the post-CPAP arm having a higher adjusted score (mean difference: −6.0, 95% CI −0.6 to −11.4, p=0.030). There was no difference in QOL scores assessed using the FOSQ questionnaire. In assessing mood symptoms between CPAP and PT using the DASS21 questionnaire, state of depression showed a statistically significant higher score in post-PT arm (mean difference: 1.0, 95% CI 0.1 to 2.0, p=0.029) but this is unlikely of clinical significance. There were no significant differences observed in states of anxiety and stress (table 3)
Quality of life, sleep quality and mood indices between CPAP and PT
Treatment adherence after 8 weeks of device use
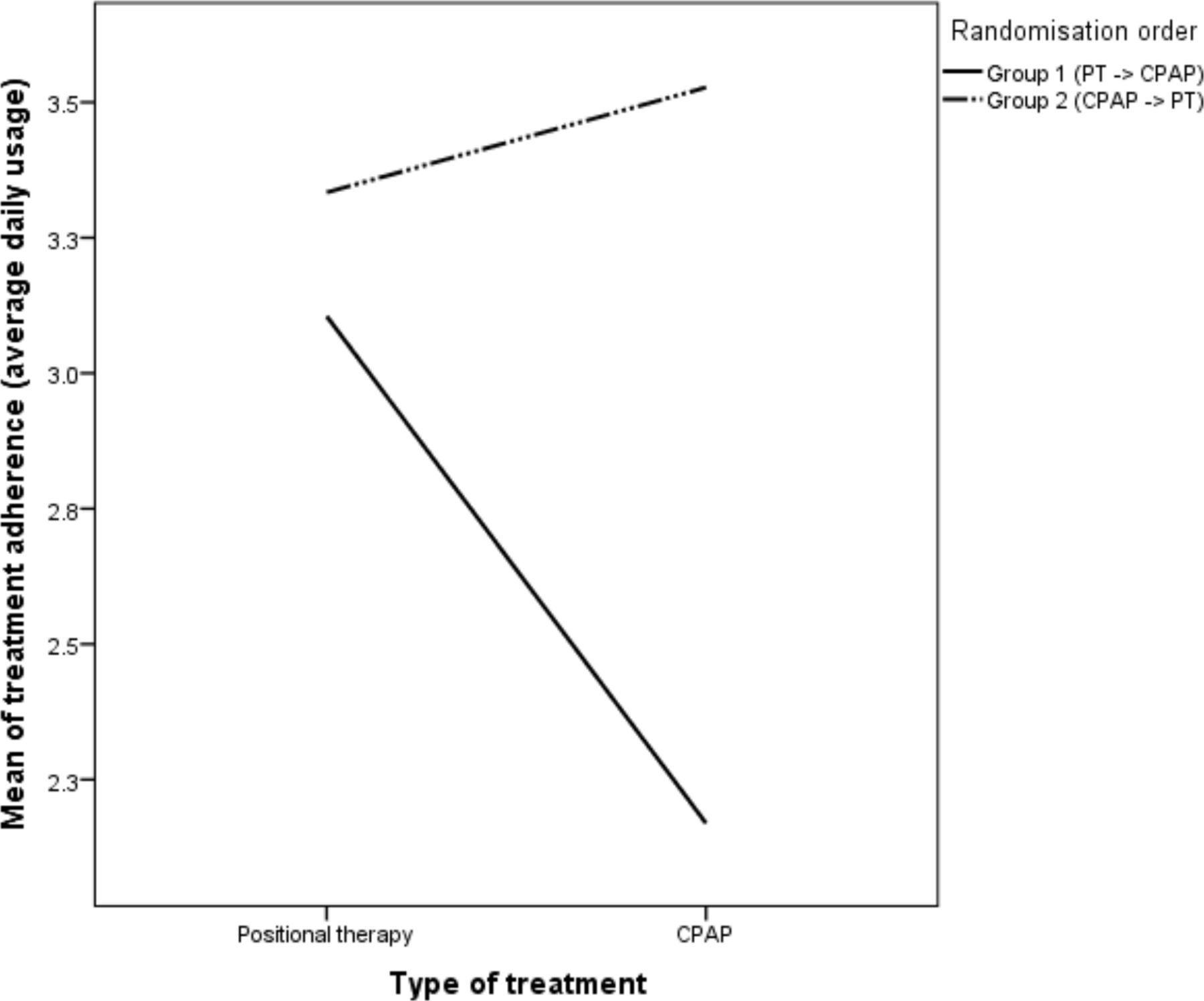
A significant intervention-by-order interaction was found during the analysis of treatment adherence (figure 3). For patients randomised to the intervention arm commencing with PT first then CPAP, mean adherence (defined by average daily usage over all days) was 3.1 hours for PT and 2.2 hours for CPAP.

Patient treatment adherence. CPAP, continuous positive airway pressure; PT, positional therapy.
For patients randomised to the alternative intervention arm commencing with CPAP first then PT, mean adherence was 4.6 hours for CPAP and 4.3 hours for PT. These results suggest that PT treatment followed by CPAP treatment resulted in longer PT usage hours compared with the converse. In addition, the results also suggest that CPAP adherence is lower if CPAP treatment occurs after PT.
Patient treatment preference
Sixty per cent (95% CI 44.6% to 73.7%) of patients preferred CPAP, 20% (95% CI 10.5% to 34.8%) preferred PT, while 20% (95% CI 10.5% to 34.8%) preferred neither device (figure 4). Of the eight patients who preferred PT, device user friendliness and ease of operation was the top reason for preference (75%). Of the 24 patients who preferred CPAP, being able to obtain a better night’s rest and feeling more energised in the day was the main reason (75%). For the eight patients who preferred neither treatment, device discomfort was the predominant reason (75%).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patient treatment preference. (A) Patients were asked which treatment device they prefer at the end of the trial. (B) Patients were asked which treatment device they prefer if both devices cost the same. CPAP, continuous positive airway pressure.
Adverse events
A total of six adverse events were reported by five patients. Two patients reported a facial rash with CPAP use while three patients reported neck itchiness or redness during PT treatment. These events were all mild. One patient reported neck pain in the first week of PT use and was subsequently diagnosed with cervical spondylosis. The neck pain eventually resolved with physiotherapy (additional details are provided as data in online supplementary file).
Supplemental material
Discussion
Hence, the non-inferiority endpoint was not met and the results were inconclusive as the CIs for the difference in ESS included the predetermined non-inferiority margin of 1.5 units, even though PT appeared worse than CPAP. Majority of patients indicated preference for CPAP treatment, citing the primary reason to be CPAP’s ability to achieve greater improvements in subjective symptoms of daytime sleepiness.
There are currently no published data from high quality RCTs comparing the new vibratory PT devices to the gold standard CPAP in the treatment of patients with POSA. A total of three cross-over RCTs, including the current trial, have therefore sought to address this clinical question. The other two trials are being conducted in the USA and Australia and likely involve a predominantly white population, providing a contrast to our study’s multiethnic Asian patients in Singapore. The PT devices used are also different in the three trials. Our study evaluated the NightShift PT (USA), which is a neck-worn device. The POSAtive study (ClinicalTrials.gov: NCT03061071) used the Nightbalance Sleep Position Trainer (SPT) (Europe) while the Australian SUPA OSA trial (ACTRN12613001242718) used the BuzzPOD PT (Australia), both of which are chest-worn devices. These are the three currently available new vibratory PT devices. We believe results from our study, together with potential findings from the two other trials, would provide interesting insights in comparing and contrasting POSA patient treatment outcomes and preferences across diverse ethnic populations.
Our study findings on patient treatment adherence to PT appear to contrast that of current available literature. Only 44.7% of our patients were adherent to PT, when adherence was defined by percentage of days of PT use at least 4 hours. In a prospective single arm study from Netherlands of 36 patients with mild to moderate POSA by van Maanen et al, a very high treatment adherence rate (defined by >4 hours device use/day) of 92.7% with the Nightbalance SPT was observed.16 In another two studies using the Nightbalance SPT by Benoist et al, treatment adherence (defined as >4 hours device use/day at least 5 days in a week) was found to be 89.3%22 and 89.0%,23 respectively at 3 months. The much lower PT adherence rate seen in our Asian study population reinforces the importance of replicating positive results from Caucasian studies in other ethnic populations. The reason for this disparity remains to be elucidated but it is possible that similar to CPAP, psychosocial factors involving wearing a device may play a role. Additionally, we would like to hypothesise that differing OSA pathophysiological traits in our population may be another plausible reason for poorer treatment efficacy and tolerance. For example, in a recent study by Lee et al, differences in arousal thresholds have been found between the Caucasian and Chinese patients with OSA24 although data comparing OSA mechanisms across diverse ethnic groups remain scarce.
We noted an interesting intervention-by-order interaction during the analysis of treatment adherence. Patients who used PT after initial CPAP treatment achieved a mean PT adherence of 4.3 hours compared with only 3.1 hours if they started PT treatment first. We theorise that patients on CPAP could have experienced faster symptom improvement compared with PT as it takes time to adapt to postural change. It is also possible that although PT appears to work, symptom improvement may be slower due to less complete resolution of obstructive respiratory events compared with CPAP. Hence, patients using CPAP first may have felt more confident in their overall treatment due to early benefit, leading to greater patient motivation even when trialled subsequently on an alternative therapy such as PT. The switch from a more complex CPAP device to a simpler and user-friendly PT could also have promoted positive behavioural reinforcement. From a clinical viewpoint, if the above hypotheses were true, it would suggest that patients with POSA may still benefit from PT therapy after initial CPAP treatment. More studies are warranted to investigate this novel finding.
Our study sought to address the lack of data on patient treatment preference between CPAP and the new PT devices. We demonstrated that CPAP was the preferred treatment choice for patients with POSA with significant daytime sleepiness primarily due to greater improvements in subjective symptoms. However, there remained a fifth of patients with POSA who preferred PT in part due to its user friendliness. With an estimated global OSA prevalence as high as 38%1 and a prevalence of POSA up to 77% in patients with OSA,10 11 the absolute number of patients with POSA who prefer PT to CPAP is still potentially in the millions. Hence, it remains important for research and innovation to further refine current PT devices’ design to cater to the many patients with POSA who would otherwise reject or not tolerate CPAP. Ultimately, patient treatment preference is likely to impact long-term adherence.
The strength of our study is its crossover RCT design and successful completion of all 40 study subjects. To the best of our knowledge, it is the first published data directly comparing the new PT to the gold standard CPAP, both in efficacy and in patient treatment preference. Compared with prior PT studies which mainly included patients with mild to moderate POSA,16 22 25 our study inclusion criteria did not place any restrictions on OSA severity. Patients ranging from mild to severe POSA were included in our study, enhancing generalisability.
Our study is limited by its relatively small sample size and due to the nature of the two interventions, the patients could not be blinded. While best efforts were made to blind the scoring sleep technologist by altering the flow channel label of the sleep study performed with CPAP in situ to resemble one without CPAP, given the nature of CPAP treatment, an experienced sleep technologist may still be able to discern the slight differences in flow waveform morphology. However, we are not aware of any methods that would enable the CPAP-supported respiratory flow to have a morphology that is identical to that of unsupported respiratory flow, as in the case with PT. Our study did not compare the use of PT in OSA subtypes,26 for example, rapid eye movement OSA versus POSA, nor take into account patients who may still snore in lateral sleep. It also used only a single definition of POSA while there are various definitions of POSA in the literature. However, there is no universal definition of POSA available. PT in a broad sense should include head elevation and neck extension but our study’s PT is based on neck rotation. This remains a limitation for all the latest vibratory PT devices which employ either neck or body rotation as the main treatment principle. As only patients with POSA with significant daytime sleepiness were enrolled, further study in patients with POSA who are less symptomatic would be required. A single PT device was evaluated in this study as it was the only device available in Singapore at the time the study started. We look forward to more research data from comparable trials involving other types of vibratory PT devices.
In conclusion, the non-inferiority endpoint of PT was not met in this study and the result was overall inconclusive. CPAP was the preferred patient treatment choice primarily due to greater improvements in subjective symptoms. Therefore, we recommend CPAP to remain as first-line treatment for patients with POSA with significant daytime sleepiness.
Acknowledgments
We would like to thank our patients for their time and contribution to the study, SG Medical and Advanced Brain Monitoring for the discounted CPAP and PT devices, respectively, our CGH Sleep Lab team of sleep technologists: Liang Jieying, Goh Kiat Lian, Astar Thant, Jehni Wong, Cynthia Lim, Felicia Lim, staff from Changi General Hospital Clinical Trials & Research Unit with special thanks to Nur Shameerah, Yan Junjie, Carmen Kam, Geraldine Lim, Ann Cheung, Yew Lay Hwa, Tan Pei Ting, Department of Otorhinolaryngology, Department of Respiratory and Critical Care Medicine, Department of Finance, Human Resource, Office of Innovation (with special thanks to Lydia Tan) and Supply Chain Management, for their support in this trial. We would also like to thank our anonymous reviewers for helping us to improve our manuscript.
References
Footnotes
Correction notice This article has been corrected since it was published Online First. The format of tables 1 and 3 have been corrected.
Contributors YM was the primary investigator of the study and was responsible for study design, data acquisition, data analyses and writing of the manuscript. KW was involved in study design, data analyses and manuscript writing. YHC was involved in study design, data analyses and manuscript review. All other authors were involved in data acquisition and collection and manuscript reviews.
Funding The study was funded by the National Medical Research Council, Singapore.
Disclaimer The sponsor had no role in study design, data collection, analysis, interpretation, manuscript writing nor the decision to submit for publication.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.