Article Text

Statistics from Altmetric.com
Case report
Maged Hassan (MH): I would like to present three cases of patients who presented with symptoms of lower respiratory tract infection, fever and cough productive of small amount of sputum. The three patients had complained of symptoms for at least 2 weeks before presentation. The chest X-rays showed large encysted collections (figure 1A) which required chest CT to delineate the source of the abnormality. The CT studies (case 1: figure 1B, C; case 2: figure 2A and case 3: figure 2C) caused prolonged discussion between the treating clinicians with opinions divided on the nature of the lesion in each case being either an encysted empyema or a large peripheral lung abscess. Clinically, the differentiation between empyema and lung abscess was important because empyema is treated with tube drainage which is only resorted to in limited situations in lung abscess with the attendant risk of creating a bronchopleural fistula or extending the infection to the pleura.
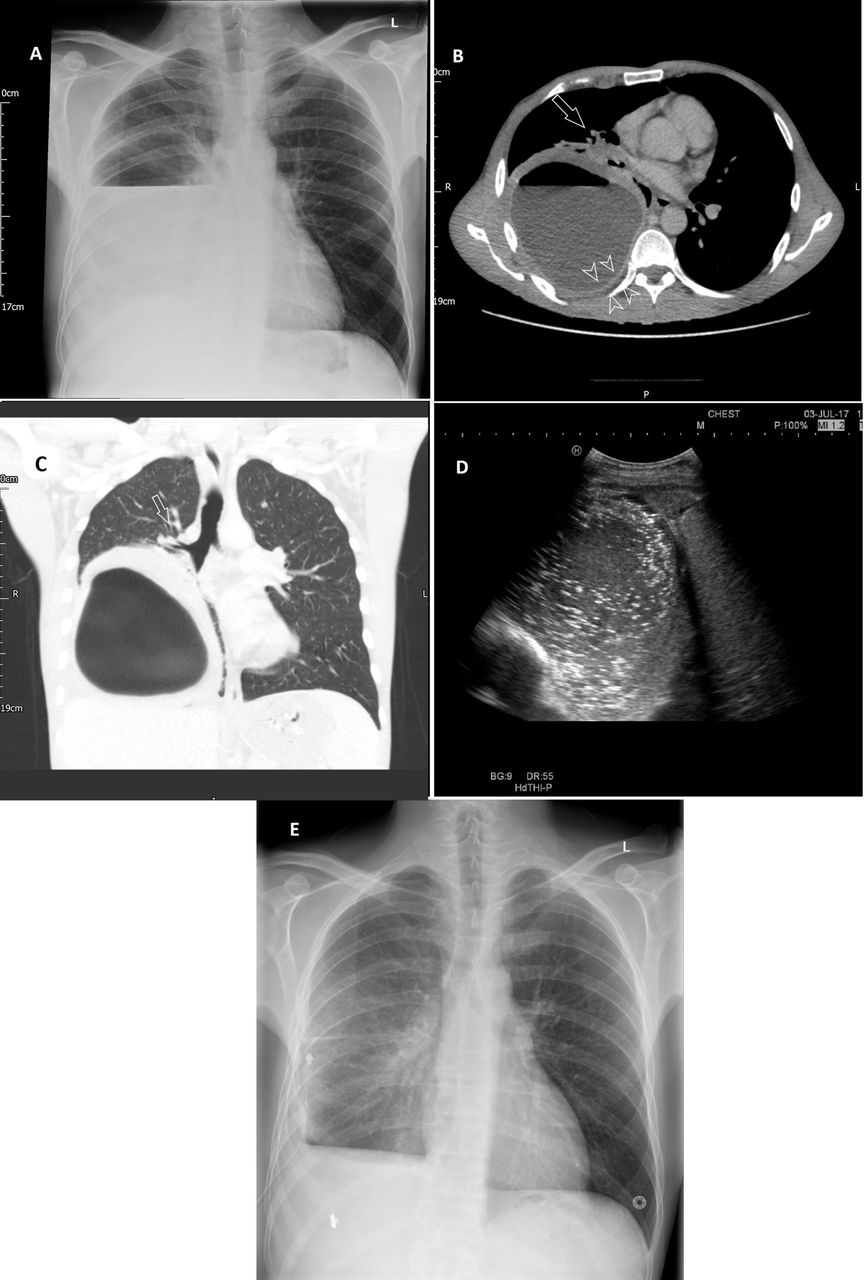
Case 1. (A) Chest X-ray shows right side cavity with air-fluid level. (B) Chest CT with contrast, axial cut, shows right side spherical lesion with air-fluid level causing lung collapse at the hilum (hollow arrow). Note pleural enhancement and extrapleural fat hypertrophy (arrowheads). (C) Chest CT, coronal reconstruction in lung window shows the acute angle the lesion makes with the chest wall and the pushed distorted airways proximal to the lesion (hollow arrow). (D) Thoracic ultrasound shows multiple hyperechoic shadows inside an echogenic collection. (E) Follow chest X-ray 48 hours after chest tube insertion (seen in situ) shows lung re-expansion.

{kind=link}
{kind=link}
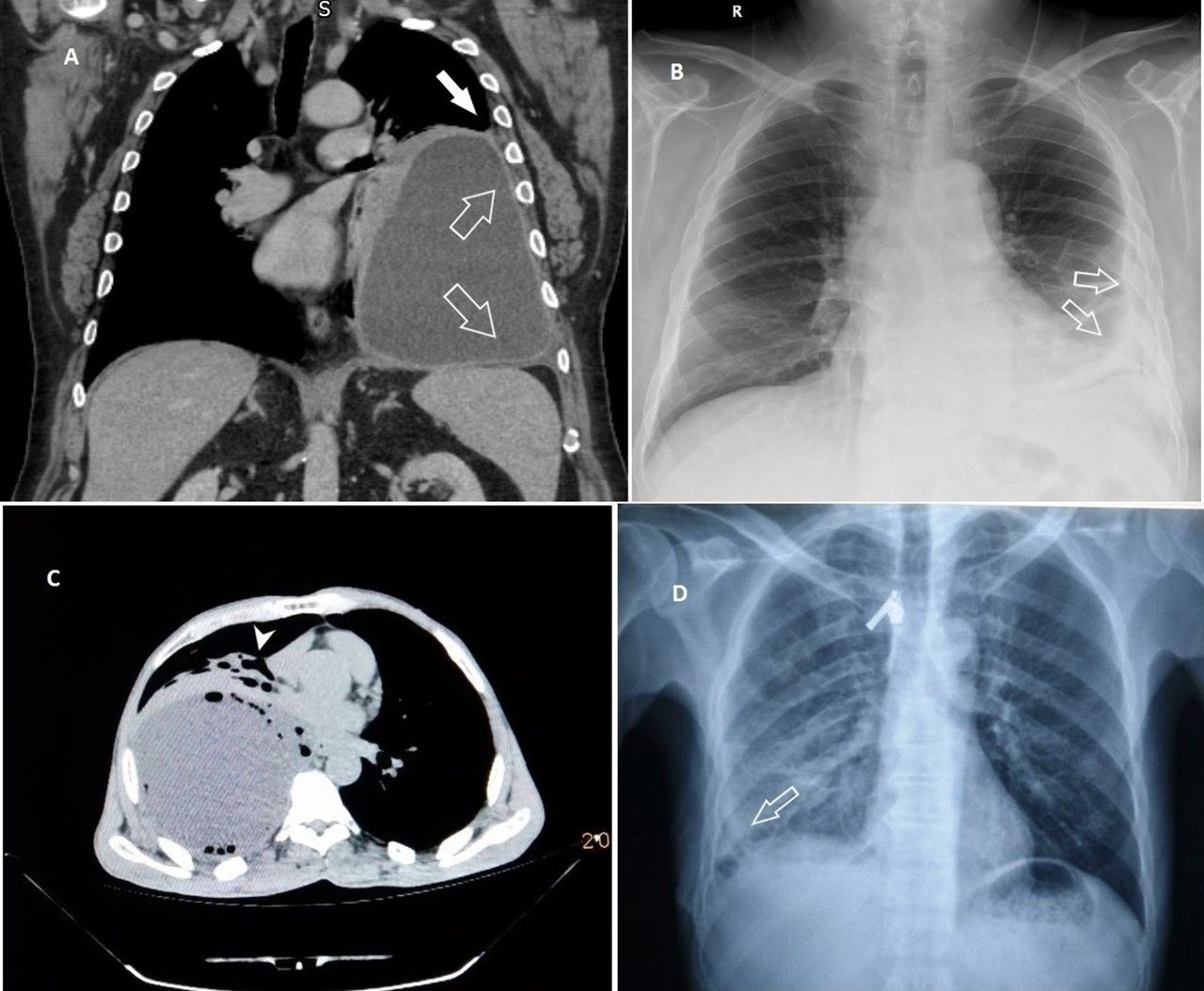
Case 2. (A) Baseline CT chest with contrast, coronal cut showing large left collection that is making an acute angle with chest wall (arrow) and uniformly thin wall with smooth inner margins (hollow arrows). (B) Chest X-ray following chest tube removal. Note thickened visceral pleura (hollow arrows). Case 3. (C) Baseline CT chest, axial cut showing right collection with making acute angle with the chest wall and causing lung collapse at the hilum (arrowhead). (D) Follow-up chest X-ray after chest drain removal showing lung re-expansion with visceral pleural thickening (hollow arrow) and small residual pneumothorax.
Najib M Rahman (NMR): The typical presentation of lung abscess is characterised by a few days of fever and chest pain with a sudden onset of coughing large volumes of purulent sputum which happens when the focus of necrotising lung infection erodes into an airway creating a passage for drainage of the infected collection. An empyema would not typically present with large-volume expectoration unless it is complicated with a bronchopleural fistula, but more commonly presents with fever and chest pain with or without cough. A large peripheral lung abscess and an encysted empyema can be confused on a chest X-ray (figure 1A). Thoracic CT is usually needed to make the distinction. The differentiating feature that is classically taught is that empyema tends to form a lenticular shape with the edges creating an obtuse angle with the adjacent chest wall, while lung abscesses appear spherical with acute angles at the abscess-chest wall interface.1 Applying this rule, the three presented cases should be diagnosed as lung abscesses (note solid arrows in figure 2A) on the basis of the CT findings. Despite being widely taught, these signs are not 100% sensitive for differentiation, and while empyemas typically appear lenticular in structure, it has been noted that they can appear rounded on CT.2 The angle the lesion makes with the chest wall and the size of the collection have been reported to be less useful signs for differentiation.2
Fergus V Gleeson (FVG): A lung abscess typically appears as a cavity with a thick wall. The abscess wall exhibits varying thickness across the circumference, which usually has an irregular internal margin.3 Conversely, empyema is more likely to have thinner walls which exhibit a smooth lumen.1 3 As shown by hollow arrows in panel 2A, the walls of the collection appear thin with smooth internal lumen and external margins, which is more typical for empyema on CT. A previous study has shown that, on average, the mean parietal pleural thickness does not exceed 3.5 mm regardless of empyema stage4 (the average wall thickness in the CT cut in figure 1B is 3 mm).
Among the other CT features that point towards empyema rather than lung abscess in this case include pleural enhancement (increase in attenuation after intravenous contrast administration) which is seen if the pleura is involved in an inflammatory or malignant process. This feature is reported in the majority of cases of empyema.4
Close assessment of the extrapleural fat can yield useful information about contiguous pleural inflammation, causing oedema in the fat layer, and appearing as hypertrophy of the fat layer in the affected hemithorax. This is best appreciated by comparing the thickness of the fat layer with the unaffected side. Increased attenuation of the extrapleural fat (due to increased water content, which is more radio-opaque) is described with empyema and is present if the attenuation of the extrapleural fat is higher by 50 Hounsefield units (HU) or more than that of subcutaneous fat.4
MH: The CT studies of cases 1 and 2 are contrast enhanced. The wall of the lesion shows enhancement (figure 1B and figure 2A). In figure 1B, there is hypertrophy of extrapleural fat (arrowheads). The attenuation of subcutaneous fat is measured at −69 HU, while it is on average 1 HU at the extrapleural region, denoting abnormally increased attenuation of this layer.
NMR: Studying the appearance of the surrounding lung on CT also provides important information. A lung abscess is typically surrounded by normal-looking lung. Bronchi and blood vessels are typically seen to be normally branching with abrupt cut-off at the abscess wall without distortion. In contrast, empyema pushes the adjacent lung parenchyma which appears compressed at the vicinity of the empyema wall.2 3
MH: Deep to the collection, compressed lung and distorted airways are noted. These are marked by a hollow arrow in figure 1B and C and by an arrowhead in figure 2C.
FVG: Among the well-known CT signs for empyema is the split pleura sign which depicts the delineation of both visceral and parietal pleural layers due to abnormal thickening and the presence of fluid between them. This sign is, however, less useful in differentiating a peripheral lung abscess from empyema as it can be seen in both conditions.5
MH: The constellation of the above signs favoured a diagnosis of thoracic empyema, and a decision to put a chest tube to drain the collection was taken in all the three cases. Prior to inserting the chest drain, an ultrasound scan was conducted to localise the site of the collection and direct the insertion site of the tube. The ultrasound picture from case 1 (figure 1D) shows multiple fairly large echogenic shadows that were seen to be moving from the distal screen towards the probe.
NMR: This appearance is the suspended microbubble sign which has been described in patients with pyopneumothorax6 and represents air bubbles inside the fluid. It is not specific to empyemas, as it is seen in other purulent collections caused by gas-forming organisms.5 6
FVG: Ultrasound can potentially differentiate between lung abscess and empyema by observing the distal lung parenchyma. Similar to features described on CT, in lung abscesses, ultrasound demonstrates normal branching airways (on greyscale) and vasculature (on Doppler) with abrupt interruption at the lung abscess wall while in the empyema wall, either distorted airways/vessels are seen or only echogenic compressed lung.3 Additionally, ultrasound is more sensitive than CT in delineating the presence of loculations/septations1 which can guide the site for chest tube insertion towards the largest loculus.
MH: The follow-up of the patients revealed acceptable lung expansion on chest X-ray in all three cases. All cases received intravenous antibiotics until chest drain removal and were discharged on oral antibiotics. None of the cases required further pleural intervention on subsequent clinic follow ups.
NMR: The clinical management of empyema involves timely drainage of the infected collection by means of chest tube with the institution of intravenous antibiotics. In addition, adequate nutrition and venous thromboembolism prophylaxis are necessary. Initial antibiotic choice depends on local microbiology but in general requires coverage for anaerobic organisms. This should be modified according to culture results.
Typically, a chest tube is left in situ until the collection is drained on subsequent X-rays, the drained fluid becomes clear and the daily output of the tube is less than 50 mL. The follow-up chest X-rays following drain removal in cases 2 and 3 (hollow arrows in figure 2B, D) show significantly thickened visceral pleura and a small rim of residual pneumothorax. These appearances are not concerning and the majority of patients on appropriate antibiotics (for 4–6 weeks) will show resolution over several weeks.
Lung abscess, on the other hand, is typically treated with intravenous antibiotics and chest physiotherapy to enhance drainage. Principles of antibiotic treatment for lung abscess are similar to empyema. In a minority of patients, drainage is suboptimal leading to ongoing sepsis and surgical removal of the diseased lobe is necessary. In frail patients, either bronchoscopic or percutaneous drainage is sometimes attempted either as a bridge to or substitute for surgery.7
Footnotes
Contributors MH and NMR conceived the report. MH, RA, RR, HS and NMR treated the patients. MH and RR collected the images of the report. FVG reviewed the radiology of the cases. MH drafted the manuscript. All authors reviewed the final manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves