Article Text

Statistics from Altmetric.com
An 87-year-old man was admitted to Jikei University Hospital presenting with fever and fatigue. Physical examinations revealed inspiratory coarse crackles on the left lung field. A chest CT detected a tumour-like consolidation around the thoracic aorta (figure 1A). Biochemical examinations found a high number of white blood cells and elevated C-reactive protein level, and a diagnosis of pneumonia was made. Penicillin antibiotics (ampicillin/sulbactam) were administered. Two days later, methicillin-sensitive Staphylococcus aureus (MSSA) was detected in two sets of blood cultures. An echocardiogram showed no vegetation and a urine culture was negative. A sputum culture was unobtainable, but pneumonia was the only focus of infection for the MSSA. Penicillin antibiotics were continued, but the patient suddenly developed cardiopulmonary arrest on day 7 after admission. Postmortem pathological examination revealed that aortic rupture was the cause of death. The intima of the autopsied aorta revealed an approximately 40 mm hole on the ruptured wall (figure 1C), and the autopsied lung indicated an area of pneumonia around the aorta (figure 1B). Pneumonia appeared to have caused an abscess at the posterior mediastinum and there was a flux of neutrophil infiltration spreading to the descending aorta from the lung, especially to the area with aortic wall rupture (figure 2A, B). These findings suggested that the MSSA pneumonia progressed to the aortic wall rather than MSSA aortitis leaking out into the lung.
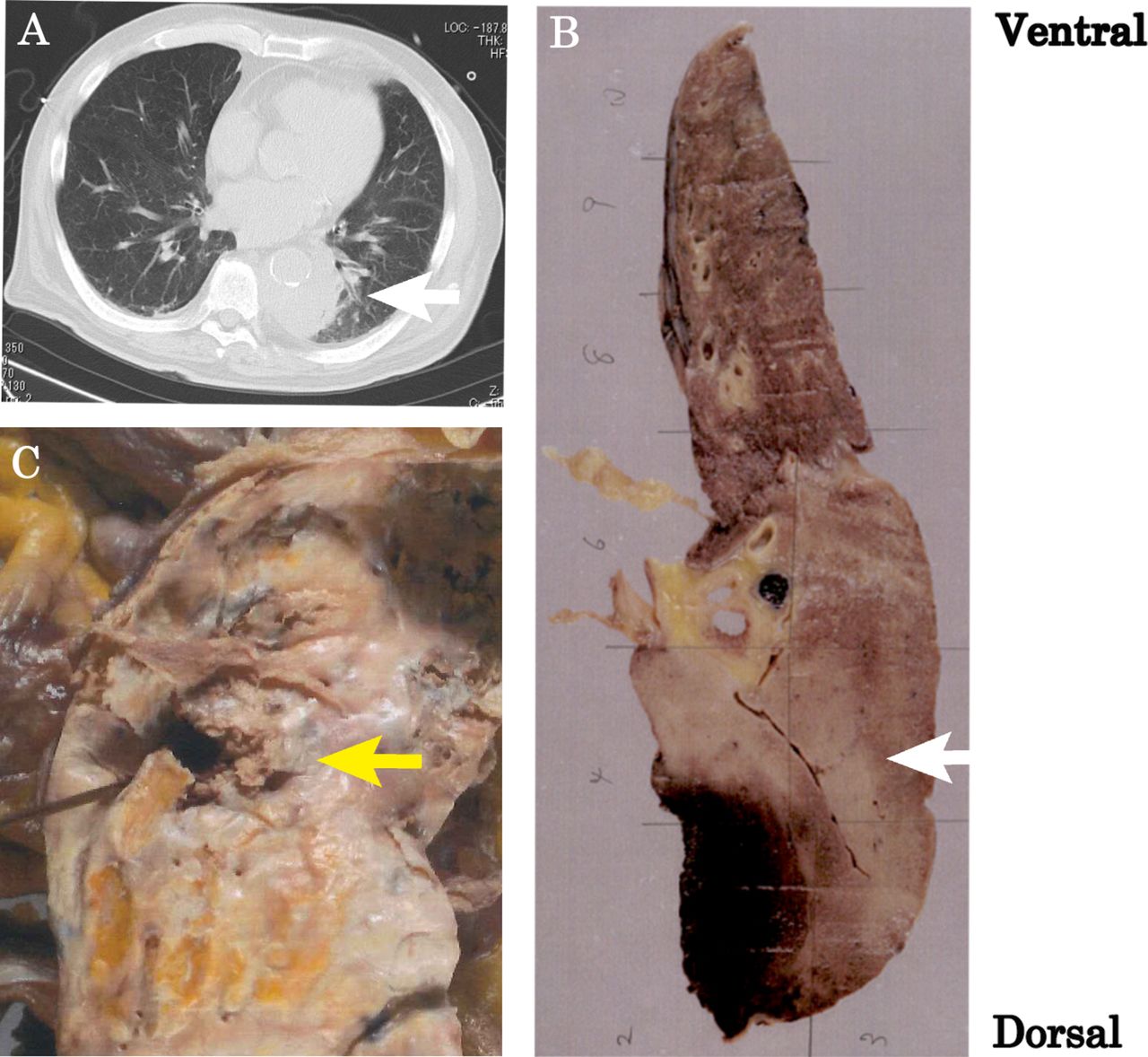
(A) Chest CT showed a tumour-like consolidation around the thoracic aorta. (B) Autopsied lung showed an area of pneumonia around the aorta (white arrow). (C) The intima of the autopsied aorta revealed strong atherosclerotic change and an approximately 40 mm hole on the ruptured wall (yellow arrow).

{kind=link}
{kind=link}
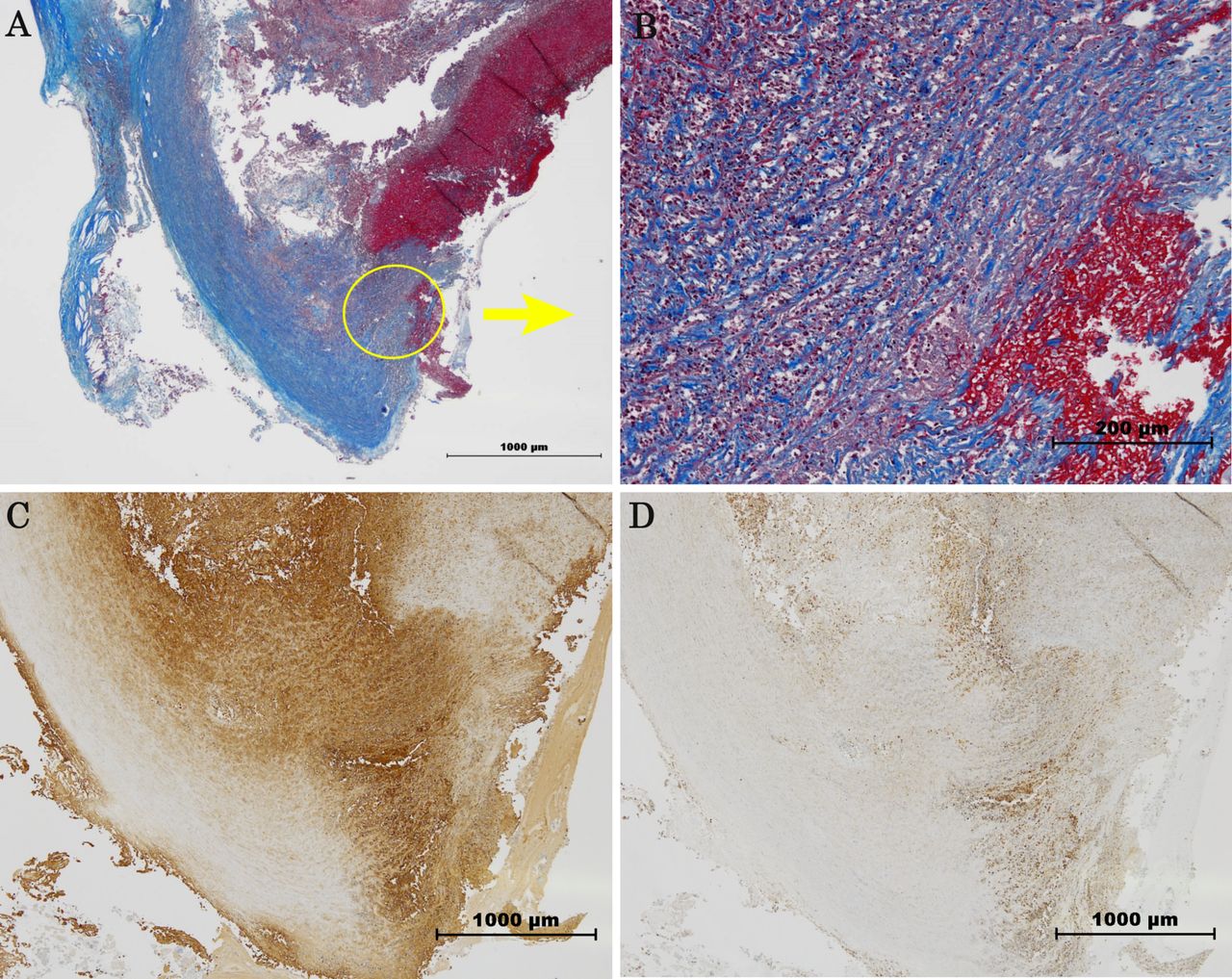
(A) The point of rupture of the aortic wall (Masson staining). (B) The magnified image of the ruptured wall (yellow-circled area on (A)) revealed significant infiltration of neutrophils from adventitia towards intima. (C) The immunohistochemistry (IHC) stains of the ruptured wall were strongly positive for matrix metalloproteinase (MMP)-9. (D) The IHC stains of MMP-8 were weakly positive on the same area of the ruptured wall.
A previous experimental report showed that S. aureus peptidoglycan elevated matrix metalloproteinase (MMP)-9 secretion by neutrophils.1 Moreover, bronchoalveolar lavage samples from patients with S. aureus pneumonia contained high concentrations of MMP-8 and MMP-9, which are important enzymes in the degradation and remodelling of the extracellular matrix.2 Pyo et al demonstrated that inflammatory cell expression of MMP-9 played a critical role in aortic aneurysmal degeneration by using MMP-9-deficient mouse model.3 Our immunohistochemical (IHC) examination of the aorta showed diffuse staining of MMP-8 and MMP-9 especially at the cleavage point of aortic rupture (figure 2C, D). The IHC stains of the ruptured wall were strongly positive for MMP-9 (figure 2C), and the stained area of the protease clearly correlated with the area of neutrophil infiltration. This was consistent with Pyo’s conclusion that MMP-9 released by inflammatory cells plays a critical role in aortic aneurysmal degeneration. These data suggested that the rupture could have been due to increased neutrophil proteases’ expression, including MMPs, in response to S. aureus in this case of MSSA pneumonia.
In conclusion, we experienced a very rare aortic rupture occurring secondary to MSSA pneumonia, in which neutrophil proteases, including MMPs, were suggested to be involved in the mechanism of wall rupture.
Footnotes
Contributors MH was responsible for the conception, design and drafting the work. JA, KN and KK were responsible for the final approval of the manuscript. All authors were involved in the multidisciplinary team consultation.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Chest clinic