Article Text

Abstract
Variable airflow obstruction is a pathophysiological hallmark of asthma; however, the interactions between acute bronchoconstriction and the cough reflex are poorly understood. We performed a randomised, single-blind, placebo-controlled, crossover study to investigate the interaction between bronchoconstriction and cough in asthma. Capsaicin was administered to evoke coughs and methacholine to induce bronchoconstriction. We demonstrated that acute bronchoconstriction increased capsaicin-evoked coughs, which improved as airway calibre spontaneously resolved. However, capsaicin-evoked coughing had no impact on methacholine-induced bronchoconstriction. This study provides evidence that bronchoconstriction increases the activation of capsaicin-responsive airway nerves, but the precise mechanisms and mediators involved require further evaluation.
Trial registration number ISRCTN14900082.
- Asthma
- Asthma Mechanisms
- Cough/Mechanisms/Pharmacology
Statistics from Altmetric.com
Background
The pathophysiological hallmarks of asthma are airway inflammation, bronchial hyperresponsiveness (BHR) and variable airflow obstruction, which manifest as symptoms of wheeze, cough, shortness of breath and chest tightness. However, the mechanisms linking the pathophysiology to symptoms are unclear. For example, the interactions between bronchospasm and cough are poorly understood. Our previous work in stable asthma has demonstrated that cough responses to citric acid and capsaicin are not correlated with methacholine BHR or FEV1.1 ,2 The effects of acute bronchoconstriction on cough responses evoked by capsaicin inhalation have only been studied in healthy volunteers where minimal bronchoconstriction (mean FEV1 fall 8.8%) had no effect on the capsaicin concentration provoking two coughs (C2).3 We aimed to investigate the interaction between acute bronchoconstriction and cough reflex activation in individuals with mild atopic asthma. See online supplement for additional details.
supplement data
Methods
Participants with controlled mild atopic asthma were recruited, but not selected for symptoms of cough. We performed an eight-visit, randomised, single-blind, placebo controlled crossover study (see online supplementary figure E1).
On visit 1, participants underwent history and examination, spirometry and capsaicin cough challenge; four inhalations of doubling concentrations of capsaicin (0.48–1000 µmol/L, 30 s apart), coughs counted in the first 15 s after each inhalation.4 The challenge was completed when the volunteer reached the final or maximum tolerated dose. The maximum evoked coughs were denoted Emax and the dose evoking half of this response as ED50. Individual ED50 doses of capsaicin were then used to evoke cough at subsequent visits. At visit 2, ≥48 hours later, participants underwent methacholine challenge (2 min tidal breathing) to evaluate PC20;5 the concentration preceding this was used to initiate bronchoconstriction at future visits. Participants next entered a three-period, single-blinded, randomised, crossover study with ≥48 hours between visits. At visits 3 and 4 (period 1), the effect of bronchoconstriction on capsaicin-evoked cough responses was assessed. Subjects were randomised to inhale either saline or methacholine for 2 min to achieve a fall in %FEV1 of 15%–25% (concentration from visit 2, next doubling concentration inhaled if required), followed immediately by ED50 capsaicin (four inhalations, 30 s apart). At visits 5 and 6 (period 2), the effect of cough reflex activation on BHR was assessed. Participants were randomised to either ED50 capsaicin or saline, followed by the methacholine concentration selected at visit 2. At visits 7 and 8 (period 3), we assessed the effect of spontaneous recovery of bronchoconstriction on evoked cough responses. Visits 7 and 8 were identical to visits 3 and 4, except after inhaling methacholine or saline, participants received ED50 capsaicin immediately and again at 30 and 60 min. Spirometry was performed before and after all challenges and participants were discharged when FEV1 returned to ≥90% of baseline. A cough monitor (Vitalograph, UK) was worn throughout visits to document the number of evoked coughs and also spontaneous coughing.
Results
Fourteen participants were enrolled and completed periods 1 and 2 (mean(±SD) age 24.2 years (±3.8), 64% female, body mass index 23.5 kg/m2 (±3.1), FEV1% predicted 96.4 (±11.1), PC20 2.0 mg/mL (±2.3) see online supplementary table E1). Fifty per cent were taking salbutamol as required, while the remainder were also taking low dose ICS (150 µg (±64.5) FP equivalent). Ten subjects returned to complete period 3.
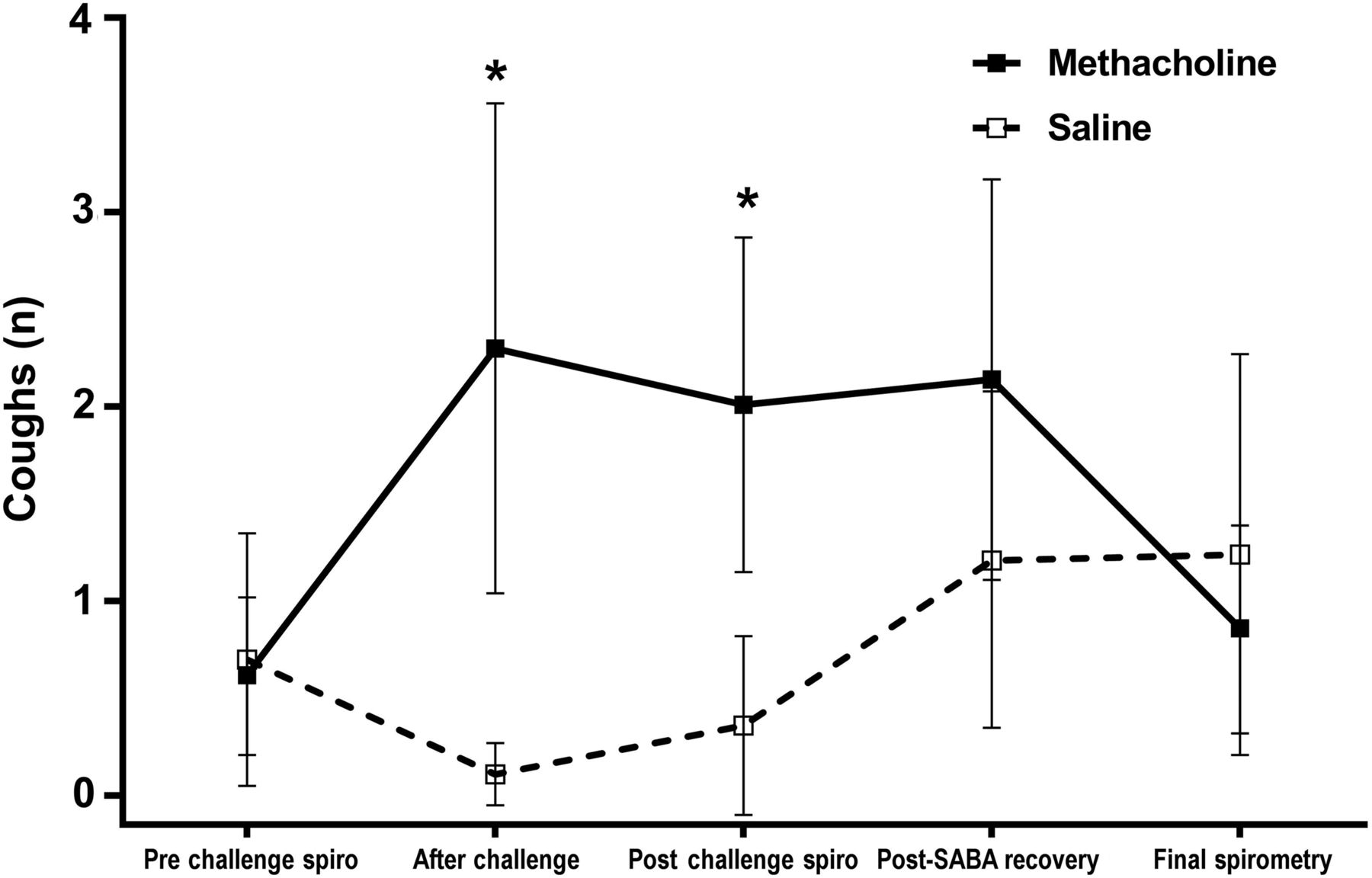
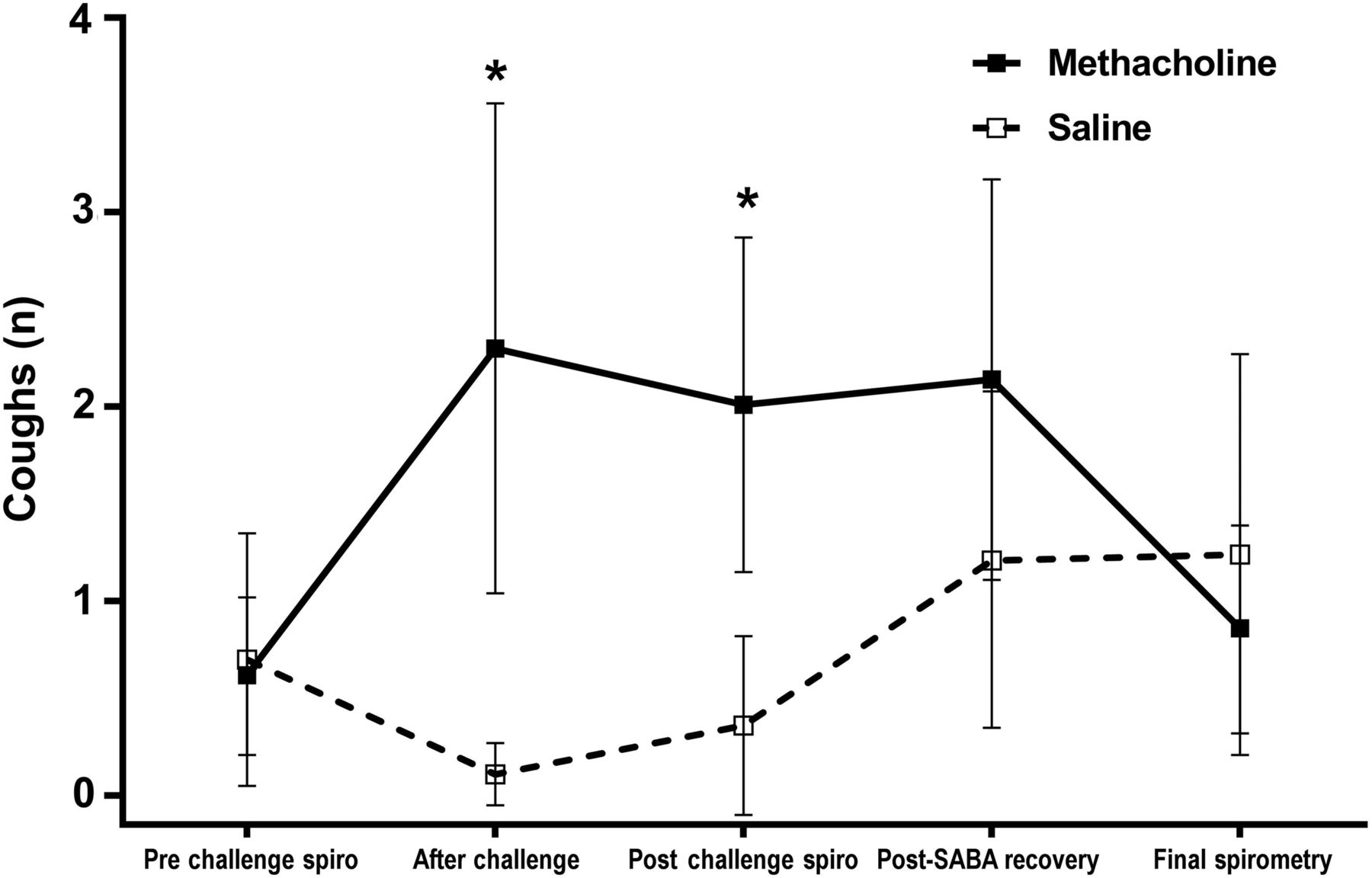
The mean % fall in FEV1 following methacholine was 19.1% (95% CI 17.3% to 21.0%) and after saline was 1.3% (95% CI 1.0 to 3.5). Bronchoconstriction increased capsaicin-evoked coughs (geometric mean 8.4 coughs (95% CI 6.6 to 10.7) vs 13.9 coughs (95% CI 10.9 to 17.8), 34.2% increase, p<0.001) (figure 1A). Spontaneous resolution of FEV1 over 60 min significantly reduced capsaicin-evoked coughs (p<0.001, figure 1B); each 10% improvement in FEV1 equated to a reduction of 2.4 coughs. Compared with saline inhalation, capsaicin-evoked coughing made no difference to the mean % fall in FEV1 after inhaling methacholine (geometric mean 13.7% (95% CI 18.7% to 8.7%) vs 12.3% (95% CI 15.7% to 8.9%), p=0.49, see online supplementary figure E2). Analysis of spontaneous coughs (when participants were not inhaling capsaicin) also demonstrated more coughs during bronchoconstriction compared with control (p<0.001, figure 2 and see online supplementary figure E3).

The effects of bronchoconstriction on capsaicin-evoked coughs. (A) Fall in %FEV1 from baseline (left y-axis) after methacholine and saline challenge with corresponding capsaicin-evoked coughs (right y-axis). (B) Spontaneous recovery of FEV1 after methacholine inhalation shown as arithmetic mean and 95% CI (left y-axis) with corresponding reduction in capsaicin-evoked coughs shown as geometric mean and 95% CIs (right axis). Cough data were log transformed for analysis to normalise distribution. All data were analysed by generalised estimating equation models adjusted for baseline ED50 coughs; there was no significant effect of gender, period or sequence. MCH, methacholine.
{kind=link}
{kind=link}
The effects of bronchoconstriction on spontaneous coughs. Visits were divided into five time periods to compare differences in spontaneous coughs; prechallenge spirometry, after methacholine/saline challenge, postchallenge spirometry, postsalbutamol recovery and after the final spirometry. Compared with saline inhalation, significant differences in spontaneous coughs were seen immediately after methacholine inhalation and after performing spirometry subsequently (both p=0.001, marked with asterisk). Coughs shown are arithmetic mean and 95% CI. A generalised estimating equation model was used to compare cough frequency between methacholine and saline during time periods when subjects were not inhaling capsaicin.
Discussion
To our knowledge, this is the first study that has investigated the interaction between acute bronchoconstriction and reflex cough in asthma. Methacholine-induced bronchoconstriction caused a significant increase in capsaicin-evoked cough responses and spontaneous coughing, which gradually resolves as airway calibre returns to baseline. In contrast, capsaicin-evoked coughing had no influence on BHR. Our data therefore challenge the concept that cough reflex responses and bronchoconstriction are independent in asthma.
There are several potential explanations for the findings in this study. First, the mechanical effect of bronchoconstriction on the epithelium, smooth muscle and other structural cells may result in the release of mediators capable of sensitising airway nerves and hence increasing cough responses to capsaicin, for example, ATP and TGF-β.6 ,7 Second, mechanosensitive afferent nerves in the airways are tonically active during tidal breathing and provide feedback to the central nervous system about changes in lung pressures/volumes. These same fibres are activated by bronchoconstriction and converge with those evoking cough in the brainstem, providing the opportunity to modify cough responses.8 Finally, bronchoconstriction alters the deposition of inhaled particles within the airways.9 During bronchoconstriction, capsaicin may have been deposited in areas more densely innervated with cough fibres. Such effects could similarly apply to real-world irritant exposures; however, as capsaicin has a very short-lived effect, the increase in spontaneous cough frequency during bronchoconstriction would argue against this explanation.
There are a number of limitations in this study. First, we have shown changes in coughs induced by capsaicin, a specific TRPV1 agonist; other tussive challenge agents provide further insights into changes in nerve function. Second, we recruited young mild atopic asthma subjects, and it is unclear whether similar results would be achieved in other phenotypes and moderate/severe disease. Third, we deliberately did not measure markers of airway inflammation in sputum or exhaled breath because performing these tests may have interfered with the challenge responses.
In conclusion, this study provides important mechanistic insights about how airway pathophysiology in asthma relates to the development of symptoms through neuronal activation. These data suggest that bronchoconstriction increases the activation of capsaicin-responsive airway nerves, but the precise mechanisms and mediators involved require further evaluation.
Acknowledgments
The authors would like to thank all the subjects who participated in the study, the National Institute for Health Research (NIHR) South Manchester Clinical Research Facility (CRF) and the NIHR/Wellcome Trust Central Manchester CRF.
Footnotes
Twitter Follow Imran Satia @lung_research
Contributors IS, HB, MW, PMO, SJF and JAS: concept and design. IS and HB: data generation. IS and JAS: statistical analysis and modelling. All authors reviewed the manuscript and approved the final draft.
Funding National Institute for Health Research, South Manchester Clinical Research Facility.
Competing interests JAS is a named inventor on a patent, owned by University Hospital of South Manchester, describing a method for generating output data licensed to Vitalograph; however, no financial benefits have been received.
Patient consent Obtained.
Ethics approval North West, Liverpool East Ethics Board (15/NW/0052).
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves