Article Text

Abstract
Rationale Individual assessment of airway obstruction in preschool-age children requires sensitive and specific lung function methods with low demand of cooperation. Although the forced oscillation technique (FOT) is feasible in young children, conventional measurements of respiratory impedance (Zrs) have limited diagnostic power in individuals.
Objective To find descriptors of within-breath Zrs that are sensitive indicators of airway obstruction during tidal breathing in children.
Methods Zrs was measured with (i) a standard multifrequency FOT (4–26 Hz) to assess the mean values of resistance and reactance for whole breaths and (ii) a 10 Hz signal to track the within-breath changes. Various Zrs measures obtained in healthy children (n=75) and those with acute wheeze (n=31) were investigated with receiver operator characteristic (ROC) analysis. The cut-off values obtained for airway obstruction were then tested in children with recurrent wheeze (n=20) before and after administration of salbutamol.
Results The largest area under the ROC curve (0.95) was observed for the tidal changes of resistance between the zero-flow values (ΔR). The ΔR cut-off value of 1.42 hPa s/L detected airway obstruction with sensitivity of 92% and specificity of 89% in children with acute wheeze and distinguished children with recurrent wheeze (16/20 above the cut-off value) from healthy children (22/23 below the cut-off value). Furthermore, ΔR significantly decreased after salbutamol in wheezy children but remained unchanged in healthy children.
Conclusions New lung function measure ΔR is able to detect airway obstruction with high sensitivity and specificity and is suitable for use in lung function testing in young children.
- Paediatric asthma
- Respiratory Measurement
Statistics from Altmetric.com
Key messages
What is the key question?
Can airway obstruction be detected in individual preschool-aged children with wheeze?
What is the bottom line?
Unlike previous lung function techniques that are able to detect differences between groups of children our novel method detects airway obstruction in individual children with sensitivity of 92% and specificity of 89%.
Why read on?
Measuring the volume dependence of resistance during tidal breathing using a modification of the forced oscillation technique has the potential to change the way asthma and other respiratory diseases are assessed in young children.
Introduction
Detection of acute pulmonary dysfunction in young children remains a challenge for physicians as there is no lung function method available in the routine clinical care that can be performed easily and reliably in sick young children.1–3 This is particularly important considering that more than half the children hospitalised for wheeze or asthma exacerbation are below 6 years of age.4 Spirometry, the ‘gold standard’ lung function test, has many limitations in preschool-age children, especially when they are unwell. In addition to the high cooperation required for the respiratory manoeuvres, the technique is not applied consistently in children below 6 years of age, as different outcome measures and cut-off points have been suggested for the assessment of airway obstruction.1 ,3 ,5–7 Alternative lung function methods have been developed in recent decades to overcome these problems; however, these techniques are more frequently employed in research studies assessing differences in lung function between healthy and diseased study groups, and are not routinely used in clinical practice.1 ,3 Objective measurements of lung function validated for detecting abnormalities in individual young children would present a significant advance.
The forced oscillation technique (FOT) has been employed widely in paediatric lung function testing due to its non-invasive nature and the lack of special breathing manoeuvres required from the subject. Several reports have addressed the utility of the FOT in paediatrics,1 ,3 ,8 ,9 and normative data are available;10–13 however, FOT methodology and data interpretation differ between commercial devices.1 In addition, current opinion suggests that FOT is more useful for showing differences between groups rather than following disease in individuals.1 ,3 This may, in part be due to the large variance of normal data in preschool-age children.10–13
Respiratory impedance (Zrs) is commonly determined at multiple oscillation frequencies and averaged over several breaths8 ,14 ,15 with the tacit assumption of linearity, that is, that the mechanical properties of the respiratory system do not change during quiet breathing. However, there is strong evidence that non-linear phenomena (flow and volume dependence of impedance) result in marked within-breath changes in respiratory resistance (R).16–19 Although the effect of the upper airways on R has not been fully established, previous research on the upper airway and vocal cord physiology demonstrated that the area of the glottic aperture achieved a minimum value in midexpiration and thus elevates the mean R during expiration. This effect was greater in the presence of airway obstruction.20 ,21 An important message from these studies was that the effects of flow and the geometry of the upper airways on R were significant in both health and disease, even during quiet breathing, and that the mean R values from total breaths or from whole inspiratory and expiratory phases separately are fundamentally dependent on the flow pattern.
The present study aimed to examine within-breath changes in Zrs, in order to determine R in phases of the breathing cycle that are the least affected by the breathing pattern (ie, airflow) and the rheology of the upper airways. We hypothesised that the change in R with tidal volume (measured between the zero-flow points at end-expiration and end-inspiration) would be a sensitive indicator of airway calibre and hence the airway obstruction during tidal breathing in wheezy preschool-age children.
Methods
Subjects and study procedures
Children with acute wheeze (study I)
Preschool-age children admitted with acute wheeze to the Emergency Department of the Royal Children's Hospital, Brisbane, Australia were enrolled in the study between June 2014 and August 2015. The relevant clinical information is shown in table 1. Children were eligible to participate if they (1) had detectable wheeze on auscultation; (2) needed treatment with short-acting β2 receptor agonist (SABA) and (3) did not require supplemental oxygen by the time of the lung function measurement. Lung function from children who had SABA 1 h prior to the study visit was excluded from the analysis. Parents completed a modified International Study of Asthma and Allergies in Childhood (ISAAC) questionnaire (see online supplementary appendix) for their child, and lung function was then measured. Another group of children (n=75) was recruited from local kindergartens as healthy controls. The consent form and a questionnaire regarding the respiratory status of their child were mailed to the parents and the forms were collected on the day of the visit. Children were defined as healthy based on the following criteria assessed in the questionnaire: (1) ≥37 completed weeks of gestation, (2) no prior diagnosis of asthma or other respiratory disease or known growth defects and (3) asymptomatic at least for 4 weeks prior to testing.
Supplementary appendix
Clinical symptoms and treatment of wheezy children from studies I and II
Children with recurrent wheeze (study II)
Children with stable wheeze or asthma (ie, more than three wheezy episodes after the first year of life and/or doctor diagnosis of asthma, table 1; symptom-free for at least 4 weeks prior to the study visit, n=20) were recruited from Asthma Clinics at the Royal Children's Hospital, Brisbane between April and November 2015. Informed consent was obtained and lung function measured before and after the administration of 400 µg inhaled salbutamol (Ventolin, GlaxoSmithKline, Ermington, New South Wales, Australia) via a spacer (Aerochamber, Trudell Medical International, London, Ontario, Canada). Bronchodilator response was also assessed in a subgroup of the healthy children (n=23).
Both studies were approved by the Children's Health Services Human Research Ethics Committee, Brisbane, Australia.
Impedance measurements
Custom-made FOT equipment, consisting of a loudspeaker and a wave tube was used to measure Zrs.22 A pneumotachograph was employed to record changes in flow and volume during tidal breathing (figure 1). Two types of FOT measurements were performed in each subject during tidal breathing. First, Zrs was measured with a multiple-frequency pseudorandom signal between 4 and 26 Hz for 16 s; these measurements were repeated until three reproducible Zrs spectra were obtained and these spectra were ensemble averaged. Second, the within-breath changes in Zrs were tracked with a single 10 Hz sinusoid, and all regular breathing periods from three recordings were selected for analysis. Details of the Zrs measurements are given in the online supplementary appendix.
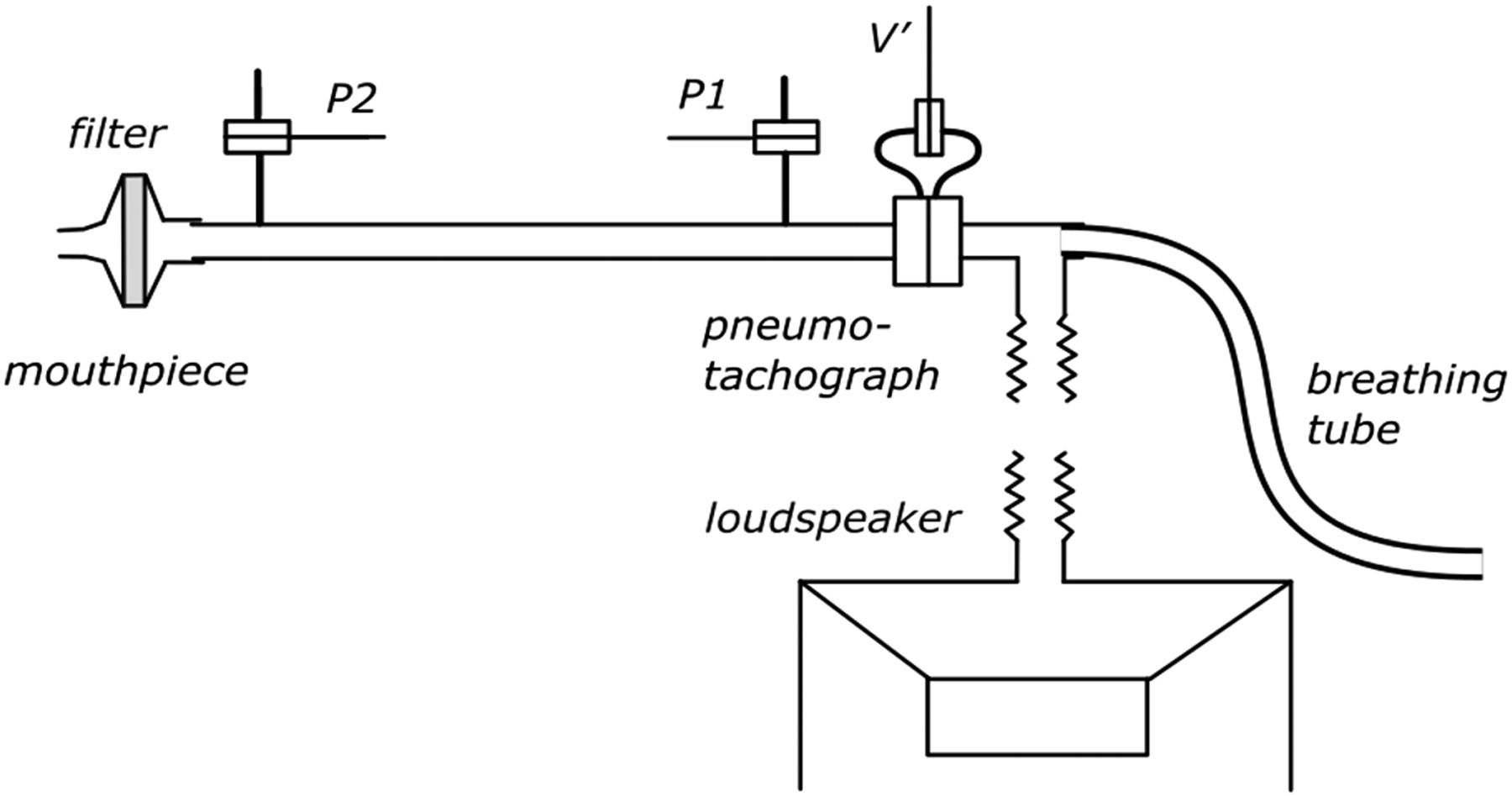
Forced oscillation technique device. P1 and P2 are two identical pressure transducers to measure the inlet and outlet pressures of the wave tube.
Data analysis
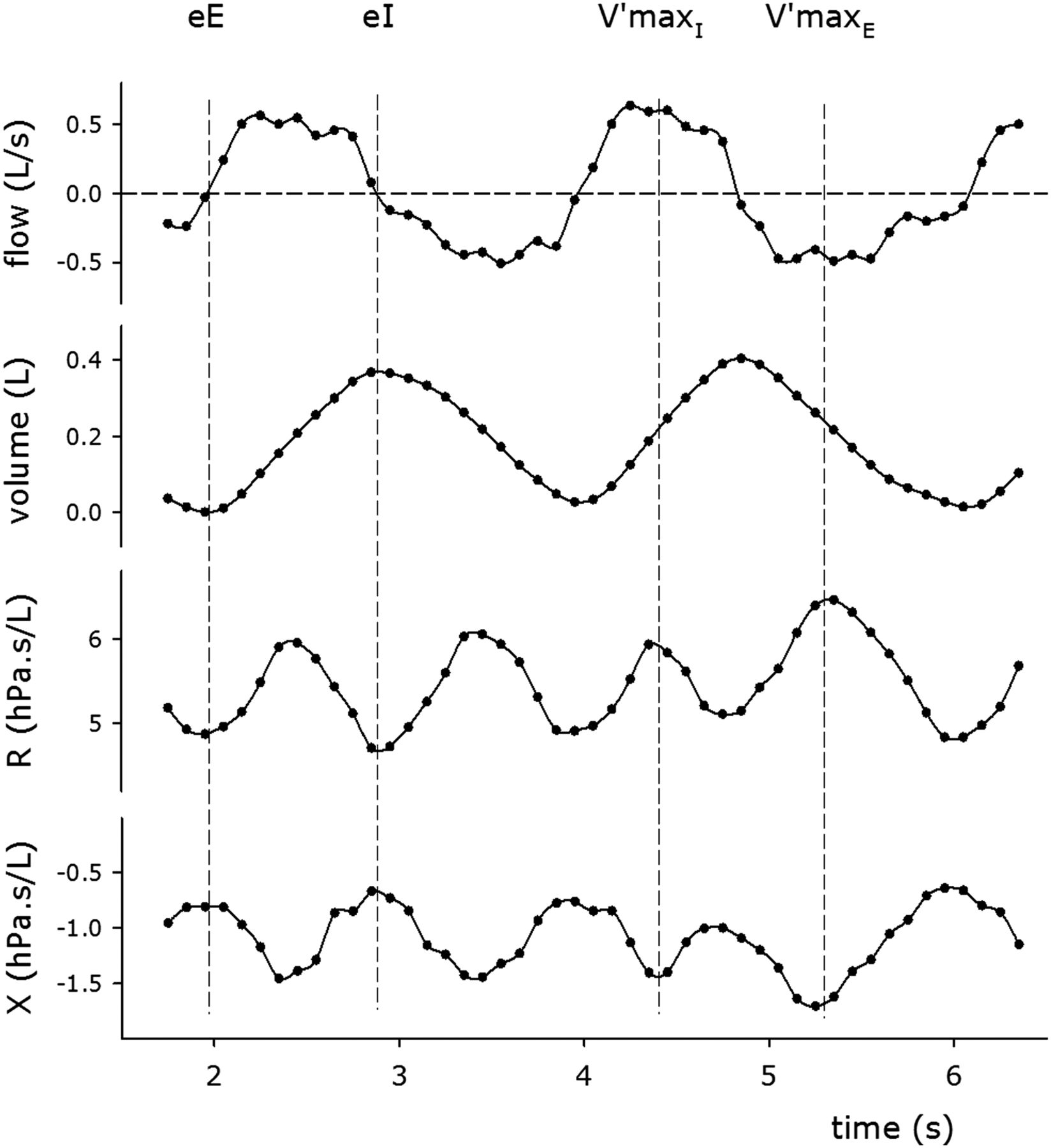
Mean values of R and X at each measured frequency were determined from the averaged Zrs spectra and those at 6, 8 and 10 Hz (R6, R8, R10, X6, X8 and X10) are reported. From the temporal recordings, R and X were obtained at every 0.1 s from all the artefact-free breathing cycles and their values were calculated at specific time points (figure 2 and table 2). The temporal variables are summarised in table 2. Tidal volume (VT), tidal inspiratory (V′maxI) and expiratory flows (V′maxE), breathing frequency (Fbr) and the expiratory time relative to the total breathing period (TE/Ttot) were obtained from the tidal flow signal.
Definitions of the within-breath impedance measures obtained from the 10 Hz recordings

Tidal changes in resistance (R) and reactance (X) with the flow and volume traces. Dashed lines indicate time points of end-expiration (eE), end-inspiration (eI), maximum inspiratory flow (V′maxI) and maximum expiratory flow (V′maxE).
Statistical analysis
Summary statistics for continuous variables are presented as either mean±SD or median (25% percentile; 75% percentile) as appropriate. The differences in Zrs and tidal breathing variables between the groups in study I were assessed with the Wilcoxon rank sum tests. A p value of <0.05 was considered statistically significant. The sensitivity and specificity, negative and positive predicted values (NPV and PPV, respectively) and likelihood ratios of the variables to detect airway obstruction were determined using receiver operator characteristic (ROC) analysis. Cut-off value for each of the variables was defined as the best relationship between sensitivity and specificity. The effect of salbutamol was analysed using the two-way repeated measures of analysis of variance.
Results
Children with acute wheeze (study I)
Three obstructed children who received SABA <1 h prior to the FOT measurements were excluded from the analysis while two children were not able to perform lung function testing (figure 3). The demographic characteristics of the children in the two groups are summarised in table 3.
Anthropometric and tidal breathing data of children (study I)

Flow chart of participants in study I. FOT, forced oscillation technique; ROC, receiver operator characteristic.
Respiratory function
Zrs data collected with the pseudorandom signal are shown in figure 4. The conventional FOT variables (R6, R8, R10, X6, X8 and X10) did not differ between the two groups (p=0.54, 0.88, 0.60, 0.72, 0.16 and 0.37, respectively). The expiration was proportionally longer and V′maxE was reduced in children with acute airway obstruction (table 3); however, minute ventilation was similar in the two groups (p=0.42). The mean values of R during inspiration (RmeanI) and expiration (RmeanE) did not distinguish between the two groups whereas the inspiratory and expiratory mean reactance (XmeanI and XmeanE, respectively) were significantly lower in children with acute airway obstruction. The differences between the corresponding inspiratory and expiratory mean values (ΔRmean and ΔXmean) did not differ between the groups (table 4).
Impedance measures calculated for expiration (RmeanE, XmeanE) and inspiration (RmeanI, XmeanI) and their differences (ΔRmean, ΔXmean) in the two groups of children (study I)

Impedance (Zrs) spectra between 6 and 26 Hz obtained in children with acute wheeze (open circles) and that in healthy subjects (closed circles). Bars represent SD.
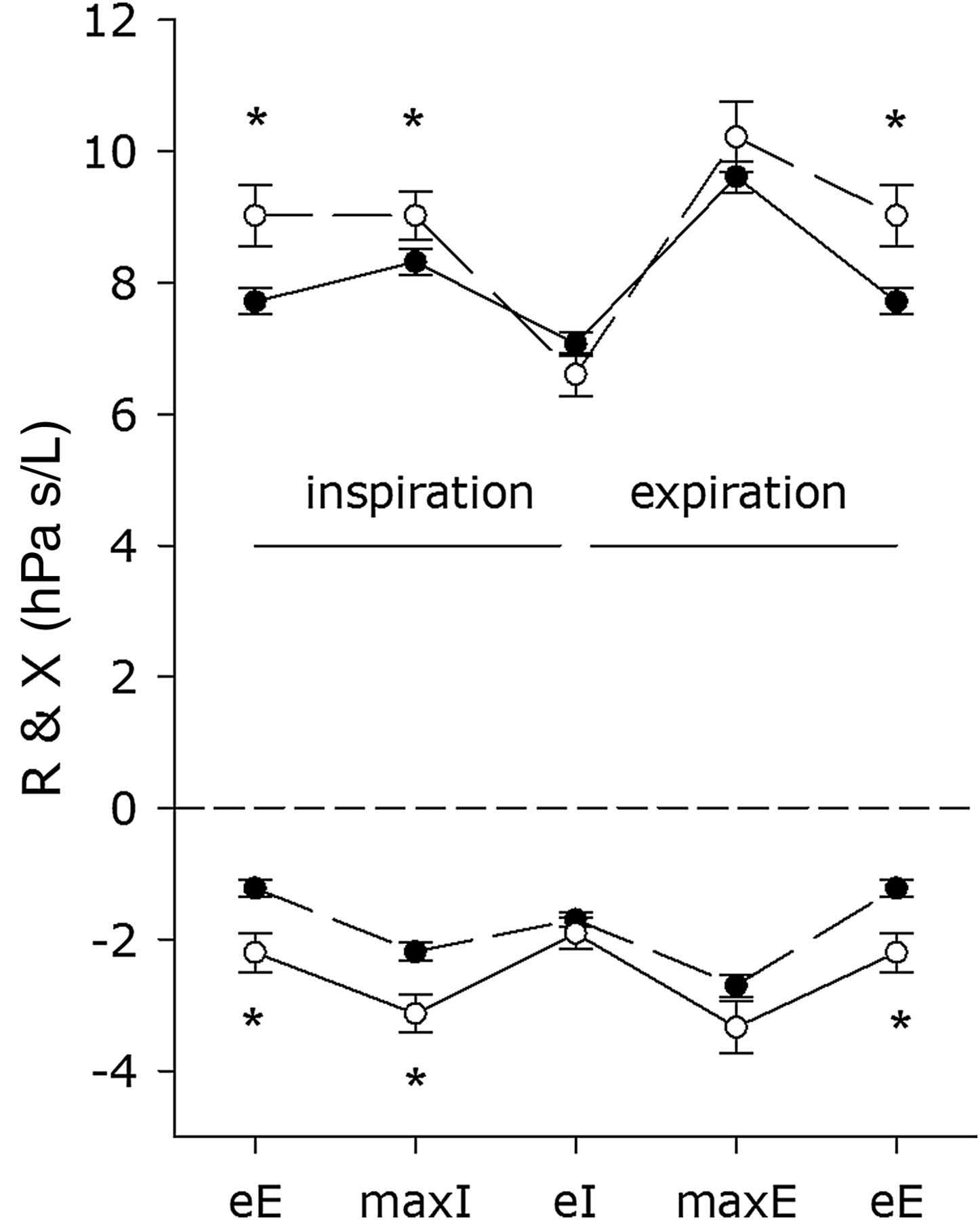
The changes in the group mean values of R and X during tidal breathing are illustrated in figure 5. At the end of expiration, R was significantly higher in children with acute airway obstruction compared with healthy subjects (p<0.001) and remained elevated at V′maxI (p=0.007). By the end of inspiration, R decreased, with the difference in R between the groups disappearing (p=0.51). The onset of expiratory flow resulted in a fast rise in R in both groups; however, in children with acute airway obstruction R was higher (p=0.02) and remained elevated at the end of expiration. The changes in X during tidal breathing mirrored the changes in R, with statistically significant differences between the two groups at end-expiration (p<0.001), at V′maxI (p<0.001) and V′maxE (p=0.005).

Mean values of resistance (R, top) and reactance (X, bottom) in children with (open circles) and without acute airway obstruction (closed circles) at the end of expiration (eE), maximum inspiratory flow (maxI), end of inspiration (eI) and maximum expiratory flow (maxE). Bars represent SEM values; *statistically significant difference between groups.
The most significant differences between the two groups were the changes in R and X between the beginning and the end of inspiration, as illustrated by typical R and X versus volume and flow loops in figure 6. Children with acute airway obstruction exhibited a significantly increased difference in R between end-expiration and end-inspiration (ΔR, figure 6B) compared with healthy children (figure 6A; 2.42±1.31 vs 0.61±0.66 hPa s/L, p<0.001), and this difference remained unchanged when ΔR was corrected for VT (7.73±5.83 vs 1.87±2.63 hPa s/L2, p<0.001). Furthermore, ΔR exhibited no relationship with the height-corrected tidal volume (cVT; r2=0.02, p=0.25) while both ReE and ReI were negatively related to cVT (r2=0.06 and r2=0.42, respectively, both p<0.001). There was a weak (although statistically significant) relationship between TE/Ttot and ΔR (r2=0.06, p=0.013); however, when height was included as a covariable in the regression, the significance disappeared (p=0.055). We note here that there was no relationship between VT, TE/Ttot and the conventional measures of respiratory resistance and reactance, that is, mean R and X at different frequencies (data not shown). The tidal change in X (ΔX) was similar in magnitude in the two groups but opposite in sign (0.29±1.08 vs −0.40±0.54 hPa s/L, p<0.001).

Tidal changes with volume (A and B) and flow (D and C) in resistance (R, top) and reactance (X, bottom) during inspiration (open circles) and expiration (closed circles) in a healthy subject (A and C) and in a child with acute airway obstruction (B and D).
Diagnostic value of impedance measures for detecting airway obstruction
The ROC curves for RmeanE, RmeanI, XmeanE, XmeanI, ΔR and ΔX are presented in figure 7. The largest area under the curve (AUC) was observed for ΔR (0.95) and ΔX (0.79), corresponding to higher values of sensitivity and specificity to detect airway obstruction than that of the mean inspiratory or mean expiratory Zrs variables (RmeanE: 0.60; RmeanI: 0.60; XmeanE: 0.65 and XmeanI: 0.70; all p<0.0001 vs ΔR). Optimal detection of airway obstruction was established with a ΔR of ≥1.42 hPa s/L, which corresponded to a sensitivity of 95% (75–99) and a specificity of 89% (80–95) with NPV and PPV of 97% (90–99) and 75 (57–89), respectively, calculated for the prevalence of wheeze in the study population (25.7%; 26/101 children). This prevalence is comparable with the expected proportion of preschool-age children with recurrent wheeze who go on to develop persistent asthma (30%). The cut-off values for potential outcome measures with values of sensitivity and specificity, NPV, PPV, positive and negative likelihood ratios are shown in the online supplementary appendix.

Receiver operator characteristic curves for within-breath resistance (A) and reactance measures (B). The open squares represent the difference between the end-expiratory and end-inspiratory resistance (ΔR) or reactance (ΔX) values; open circles and triangles indicate the mean values of the resistance and reactance in expiration (RmeanE, XmeanE) and inspiration (RmeanI, XmeanI), respectively.
Children with recurrent wheeze (study II)
Bronchodilator response
Baseline lung function was measured in 20 children with recurrent wheeze (age: 4.04±0.55 year, height: 101.3±7.4 cm) and 23 healthy children (age: 4.29±0.51 year, height: 99.6±5.3 cm). Three wheezy children were not able to repeat the lung function test after administration of salbutamol. Bronchodilator response in Zrs measured with the multiple-frequency signal is illustrated in figure 8. There was no significant difference between the groups either at baseline or in their responses to salbutamol. Despite the lack of differences in the conventional FOT variables, ΔR and RmeanI were significantly increased at baseline in the wheezy children compared with the healthy children (table 5). Sixteen of the 20 wheezy children had a baseline ΔR higher than the cut-off value defined for airway obstruction in study I, while ΔR was below the cut-off in 96% of the healthy children (22 out of the 23). The difference in ΔR between the groups disappeared after the administration of salbutamol (figure 9, p=0.38).
Resistance (R) and reactance (X) measures calculated at 6 Hz (R6 and X6), separately for expiration (RmeanE and XmeanE), inspiration (RmeanI and XmeanI) and the volume dependence (ΔR and ΔX) in two groups of children presalbutamol and postsalbutamol (study II)
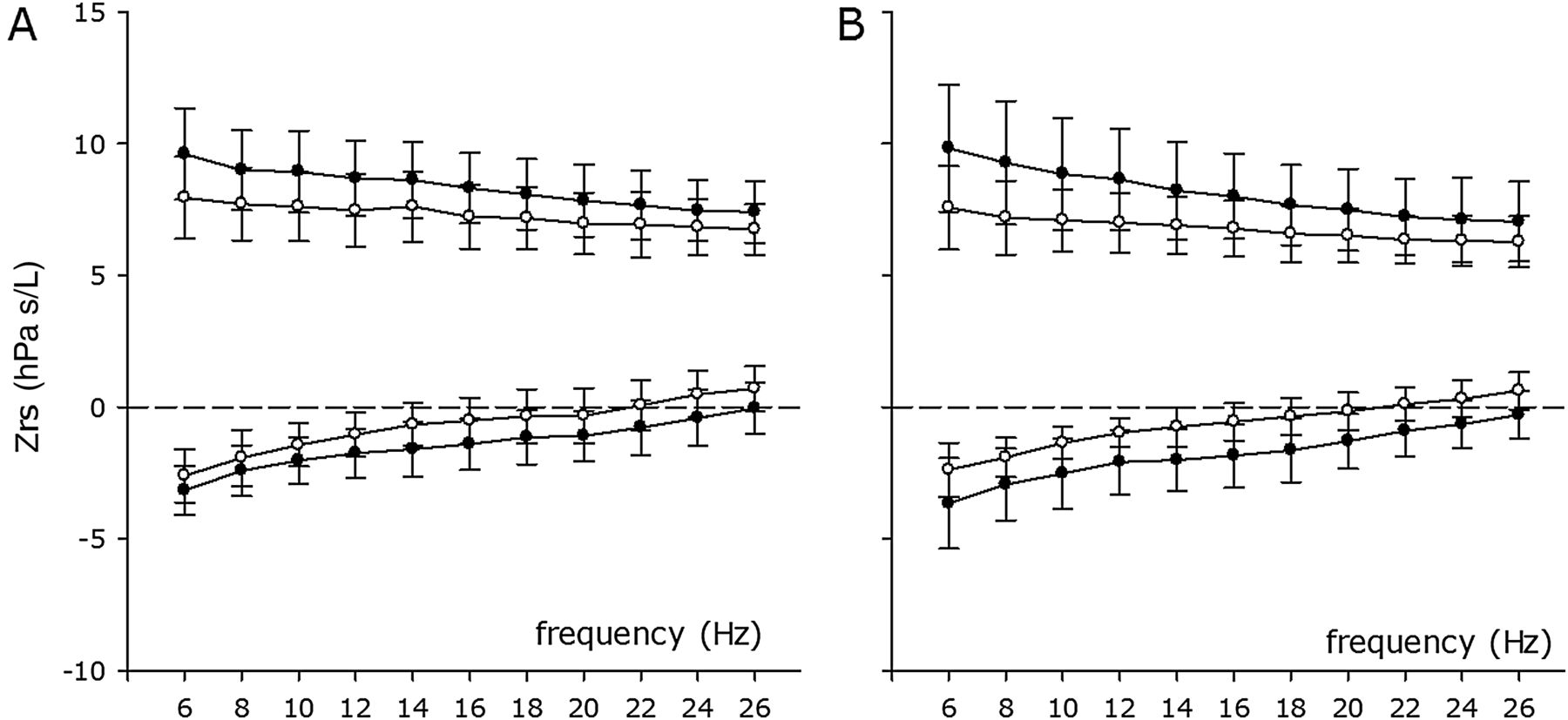
Respiratory impedance (Zrs) between 6 and 26 Hz in healthy (A) and children with recurrent wheeze (B) before (closed circles) and after administration of salbutamol (open circles). Bars represent SD.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Individual changes in volume dependence of resistance (ΔR) preadministration and postadministration of salbutamol. Symbols and lines represent data in healthy children (A) and children with recurrent wheeze (B). The horizontal dashed line shows the cut-off value of ΔR for airway obstruction (1.42 hPa s/L).
Discussion
The results from the present study demonstrate that the change of respiratory resistance during normal breathing is a highly specific and sensitive measure of airway obstruction in young children, whereas the conventional averaged estimates of respiratory resistance fail to discriminate between the wheezing and healthy preschool-age children. Together with the known feasibility of the FOT in young children and the achievable high success rate the extension of this technique to the within-breath analysis of respiratory mechanics has the potential to reveal physiologically and clinically important alterations in airway function.
Respiratory resistance is assumed to reflect airway calibre; therefore, FOT measurements have been employed widely in paediatric studies in various groups of patients with respiratory disease.23–28 While some of these studies suggested that, similarly to other methods, such as spirometry5 ,7 and multiple breath washout29 ,30 the FOT was able to distinguish between healthy and diseased subject groups,25 ,28 ,31–33 others raised concerns about the diagnostic value of the Zrs data, especially in young children.23 ,24 ,26 ,27 ,34 The controversies surrounding the FOT arise from the diversity of Zrs measures reported from the various studies and also from the wide range of the normal values in the paediatric population for any given age or height.10–13 The large variability of the Zrs in healthy preschool-age children can be explained, in part, by the unstable end-expiratory lung volume level and the variable breathing patterns adopted by young children.35 In agreement with the body of the literature we did not find a difference between healthy and wheezy children when using conventional mean values of Zrs measures from whole breathing cycles or considering only the inspiratory phase as proposed recently.19 ,32 ,36
Previous investigations suggested that R measured during spontaneous breathing reflects the overall airway calibre and is also determined by the airflow through the upper airways and larger conducting airways.37 In agreement with earlier findings,16–19 our within-breath Zrs data demonstrated that R increases with expiratory flow reaching its peak at the maximum flow that can be related to the vocal cord movements during tidal breathing (ie, during expiration, the glottic aperture narrows and reaches its smallest diameter at midexpiration).20 ,21 It is important to note that, the glottic aperture resumes its original area at the end of expiration in healthy adults. Since there are no data available on vocal cord movements in airway obstruction in children, we cannot exclude the possibility that, contrary to the findings in adults,20 ,21 the relatively narrow glottic aperture during expiration does not completely return to its original size by the time inspiration begins, possibly affecting R at the end-expiration, and hence ΔR. Although further investigations are required to localise the airway obstruction (ie, intrapulmonary vs extrapulmonary), our data suggest that independently of the exact location, ΔR is a sensitive and specific indicator of the airway obstruction in young children. These findings support our hypothesis that by the identification of the zero-flow resistance points we can minimise the effect of the non-linear, flow-dependent behaviour of the upper airways on R.
Although flow dependence of R is also significant in inspiration, the mean values of the inspiratory R have been suggested as a surrogate measure of airway resistance.16 In the present study, the diagnostic value of RmeanI was weak, which suggests that flow-dependent contributions to R during inspiration did not differ between groups. The flow dependence of R, present in both inspiratory and expiratory phases, is primarily related to the breathing pattern and not to the degree of obstruction, and this may exert a masking effect on the assessment of airway calibre. This finding may explain why the average R obtained with the conventional FOT is poor in separating normal and diseased subject groups. Indeed, significant improvements in sensitivity and specificity were attained in the present study when the influence of flow on R was eliminated by examining the change in R between the zero-flow, that is, end-inspiratory and end-expiratory points (ΔR). The diagnostic power of ΔR reported in the present study is much greater than that of any lung function index, including that of the FOT, reported previously in the preschool-age group.27 ,33
The mechanisms by which ΔR differs between healthy children and those with acute airway obstruction are likely to be complex, and their clarification needs further investigation. Nevertheless, the fact that the difference in R at end-expiration between the two groups diminishes during inspiration suggests that the airways of children with acute obstruction demonstrate an increased baseline constrictor tone before inspiration begins (ie, at functional residual capacity) that is reduced by a normal tidal expansion of the lungs but then re-established during expiration. This finding is consistent with the observation in precision-cut human lung slices where the acetylcholine-induced smooth muscle constriction of the individual intraparenchymal airways was reversed with the tidal expansion.38 It is also possible that inhomogeneity in the resistance of the distal airways at end-expiration is higher in children with obstruction; this is indicated by both a higher R and an increase in apparent elasticity of the lungs39 ,40 as reflected by the more negative X values that also return to a normal level at end-inspiration. The inhomogeneity of peripheral resistance might reach the degree of cyclic closure and reopening of some peripheral lung units, which would also be consistent with the observed changes in R and X. The coupling of the resistive and elastic parameters during the breathing cycle is also supported by the second highest value of the AUC (0.79) observed in the ROC analysis for ΔX.
Analysis of R as a bilinear function of flow and volume has proved useful in characterising the volume dependence before and after methacholine provocation18 ,37 and subsequent bronchodilatation in children with a history of cough or asthma.19 In the present study, expiratory flow limitation was present (and the ratio V′maxE/V′maxI reduced) in acute airway obstruction compared with that in healthy children. However, detailed analysis of our data suggests that changes in R with tidal volume are more specific for airway obstruction than the changes in the flow profile (data are not shown). On the basis of the cut-off value of ΔR established in children with acute airway obstruction, 80% of the children with recurrent wheeze were identified as having airway obstruction in our test population and 96% of the healthy children were properly classified as not having airway obstruction before the administration of salbutamol. Furthermore, all variables we studied changed in both groups significantly and uniformly in response to salbutamol, whereas ΔR only decreased in asthmatics and was thus able to differentiate between the groups. This finding suggests that although these children with well controlled stable asthma exhibit conventional lung function measures apparently very similar to that of the healthy children (this may partly be due to the relatively low contribution of the small airways to the total resistance of the respiratory system), a sensitive technique is able to reveal the alterations in their airway function. Further investigations are needed to establish whether the lack of a high ΔR and response to salbutamol in some of our wheezy children reflects a well controlled and/or early stage of disease without ongoing inflammation and airway remodelling, or it is associated with structural alterations of the airway wall that result in a decreased airway distensibility which cannot be eliminated by the administration of bronchodilator agonist.
Since the influences of height and age on ΔR and ΔX were not significant in the present study, the cut-off values established for children between 3 and 7 years of age can be applied safely to other populations of young children with similar demographics. However, it is important to note that the potential of ΔR as a descriptor of airway dynamics in children with paediatric respiratory conditions other than asthma, such as those associated with peripheral abnormalities (cystic fibrosis and interstitial lung disease) needs to be further investigated. Additionally, although the primary aim of this study was the comparison of the within-breath approach with conventional FOT, assessment of agreement with other techniques commonly employed in the preschool age (multiple breath washout, forced spirometry) would be informative. We nevertheless think that the present results document a methodological advance worthy of further investigation in larger and longitudinal studies.
In conclusion, the assessment of the tidal and flow-independent changes in forced oscillatory resistance in the present study has resulted in a significant improvement in the sensitivity and specificity attained previously with the FOT and other lung function tests in the differentiation between healthy preschool-age children and those with acute bronchial obstruction. The cut-off value of ΔR used in a test population properly separated wheezy and healthy children. Our results demonstrate the potential of the within-breath approach of the FOT in the assessment of lung disease in individual patients.
Acknowledgments
The authors wish to thank all the staff members of the Respiratory Department and Respiratory Function Laboratories within the Royal Children's Hospital, Brisbane for their support with participant recruitment and testing throughout the study. We would also like to thank the children and their families for their time and help to participate in the present studies.
References
Footnotes
DC and CS contributed equally.
Contributors DC, CS, ZH and PDS conceived the study and designed the measurement principle. CS, DC, KT, AK and AC recruited patients and collected data. DC, ZH, GM, BR and ZG designed the methods of measurement and data processing. DC, CS and RSW processed the recordings and analysed the data. DC, ZH and PDS drafted the manuscript. All authors have seen and approved the submitted manuscript.
Funding The study has been supported by the National Health and Medical Research Council of Australia (#1002035 and #1078600), the Office of Health and Medical Research, Government of Queensland (#50133) and the Royal Children's Hospital Foundation, Brisbane, Queensland, Australia (#50005), Hungarian Scientific Research Fund (#105403), European Respiratory Society Clinical Research Collaboration Award ERS-CRC-2013-02.
Competing interests None declared.
Ethics approval Children's Health Services Human Research Ethics Committee, Brisbane, Australia.
Provenance and peer review Not commissioned; externally peer reviewed.