Article Text

Abstract
Background QVA149 is a once-daily (o.d.) inhaled dual bronchodilator containing a fixed-dose combination of the long-acting β2-agonist indacaterol and the long-acting muscarinic antagonist glycopyrronium for the treatment of COPD. The QUANTIFY study compared QVA149 with a free-dose bronchodilator combination of tiotropium plus formoterol (TIO+FOR) in improving health-related quality of life (HRQoL) of patients with COPD.
Methods This multicentre, blinded, triple-dummy, parallel-group, non-inferiority study randomised patients aged ≥40 years with moderate-to-severe COPD (post-bronchodilator forced expiratory volume in 1 s (FEV1) ≥30% to <80% predicted) to QVA149 110/50 µg o.d. or TIO 18 µg o.d.+ FOR 12 µg twice daily (1:1) for 26 weeks. The primary endpoint was to demonstrate non-inferiority in HRQoL assessed using St George's Respiratory Questionnaire-COPD (SGRQ-C). The prespecified non-inferiority margin was 4 units. Secondary endpoints included Transition Dyspnoea Index (TDI) score, pre-dose FEV1, forced vital capacity (FVC) and safety.
Results Of the 934 patients randomised (QVA149=476 and TIO+FOR=458), 87.9% completed the study. At week 26, non-inferiority was met for SGRQ-C (QVA149 vs TIO+FOR; difference: –0.69 units; 95% CI −2.31 to 0.92; p=0.399). A significantly higher percentage of patients achieved a clinically relevant ≥1 point improvement in TDI total score with QVA149 (49.6%) versus TIO+FOR (42.4%; p=0.033). QVA149 significantly increased pre-dose FEV1 (+68 mL, 95% CI 37 mL to 100 mL; p<0.001) and FVC (+74 mL, 95% CI 24 mL to 125 mL; p=0.004) compared with TIO+FOR at week 26. The incidence of adverse events was comparable between both treatments (QVA149=43.7% and TIO+FOR=42.6%).
Conclusions QVA149 is non-inferior to TIO+FOR in improving HRQoL, with clinically meaningful and significant improvements in breathlessness and lung function in patients with COPD.
Trial registration number NCT01120717.
- COPD Pharmacology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
-
What is the key question?
-
Is QVA149 non-inferior to tiotropium plus formoterol (TIO+FOR) combination in improving health-related quality of life (HRQoL) of patients with COPD?
-
What is the bottom line?
-
QVA149 is non-inferior to TIO+FOR combination with respect to HRQoL, but shows significant improvements in breathlessness and lung function.
-
Why read on?
-
This is the first non-inferiority trial comparing active pharmacological treatments using HRQoL as a primary endpoint.
Introduction
Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2014 strategy, and the 2010 National Institute for Health and Care Excellence (NICE) guidelines recommend the use of combined bronchodilators of different pharmacological classes in patients with COPD.1 ,2 Combining bronchodilators has proved to be more efficacious and reduces the risk of side effects compared with increasing doses of monotherapy.3–6 The complementary mechanisms of action of long-acting β2-agonists (LABAs) and long-acting muscarinic antagonists (LAMAs) significantly improve bronchodilation in patients with COPD in comparison with respective monotherapies,6–8 and hence are recommended first-line treatment in patients with moderate-to-severe COPD.1
QVA149 is an inhaled once-daily (o.d.) dual bronchodilator containing a fixed-dose combination of the LABA indacaterol9 and the LAMA glycopyrronium10, being approved for the maintenance treatment of patients with symptomatic COPD in the European Union. Clinical studies have demonstrated the efficacy and safety profile of once-daily QVA149 in patients with COPD.3 ,8 ,11 ,12 Tiotropium (TIO), a LAMA, and formoterol (FOR), a LABA, are well-accepted bronchodilators for the treatment of COPD.6 ,13 ,14 The free-dose combination of TIO plus FOR, delivered via two separate inhalers, has an established efficacy in a number of clinical trials, is recommended by COPD guidelines and has been widely used for many years. The combination has been shown to significantly improve lung function, symptoms, reduce the number of COPD exacerbations and improve health-related quality of life (HRQoL).6 ,14–17
The BEACON study had shown non-inferiority of QVA149 compared with the free-dose combination of its monocomponents.18 However, in view of the wide usage and standard-of-care treatment with TIO and FOR free-dose combination, it remains conjectural whether QVA149 is non-inferior to this LABA/LAMA combination. The question examined by this study pertains to a highly relevant comparison based on the expectation that single inhalation QVA149 would have comparable patient-reported outcomes, and safety profile as the TIO+FOR free combination treatment, taken twice-daily via two separate inhalers.
In the QUANTIFY study, QVA149 o.d. was compared with TIO o.d. plus FOR twice-daily (b.i.d.) over a period of 26 weeks in patients with moderate-to-severe COPD. This study, though conducted for German health authorities, has wider scientific implications considering the wide usage of the TIO+FOR combination. Assessment of non-inferiority of QVA149 to TIO+FOR combination was based on a prespecified non-inferiority margin of 4 units on the St George's Respiratory Questionnaire-COPD (SGRQ-C), which is a sensible definition for the limit of a clinically relevant effect for the improvement in SGRQ-C.19
Patients and methods
Study design and treatments
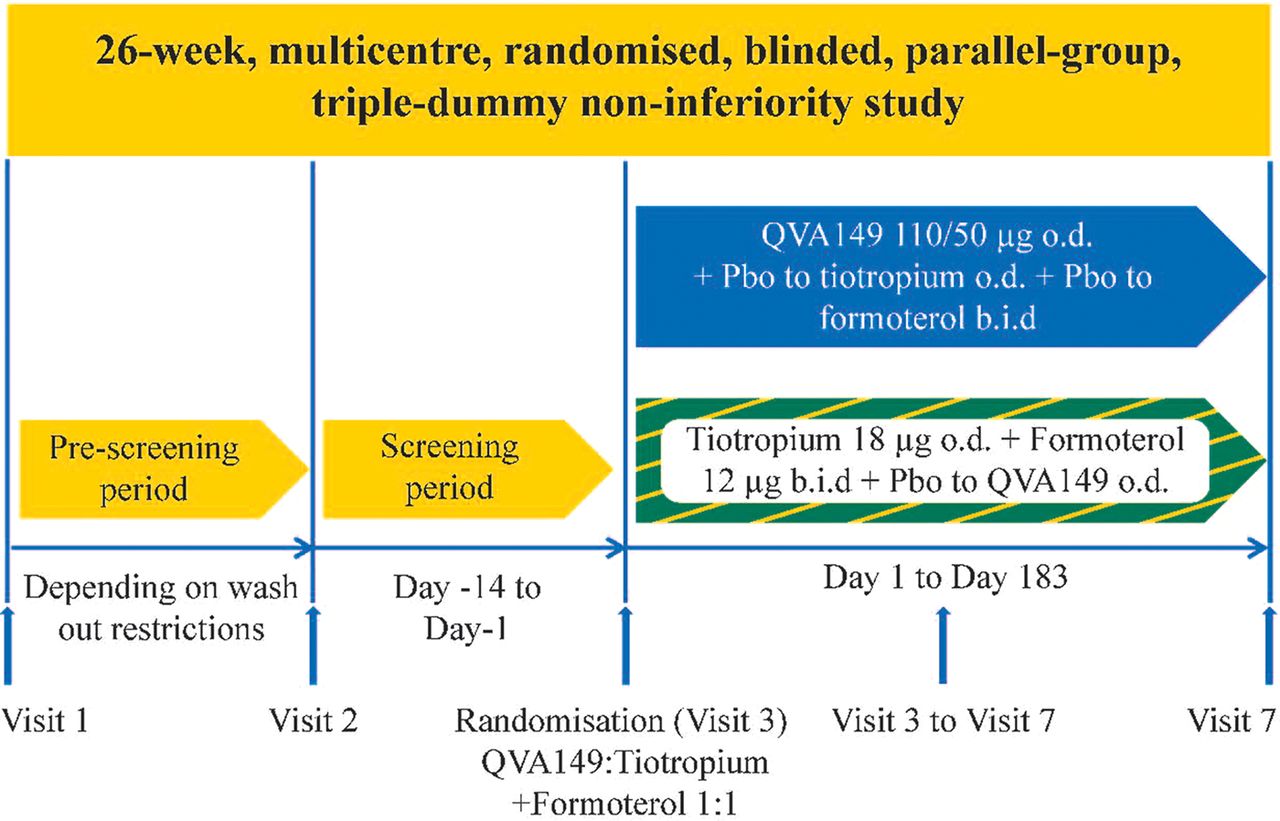
This was a 26-week multicentre, randomised, blinded, triple-dummy, parallel-group, non-inferiority design. After screening and a run-in period (up to 2 weeks), patients were randomised (1:1) to receive QVA149 (indacaterol 110 μg and glycopyrronium 50 μg) o.d. (delivered via the Breezhaler device (Novartis Pharma AG, Stein, Switzerland)) or TIO 18 μg o.d. (delivered via the HandiHaler device (Boehringer Ingelheim, Ingelheim, Germany)) plus FOR 12 μg b.i.d. (delivered via the Aerolizer device (Novartis Pharma AG)) and corresponding placebos (figure 1).14 ,15 ,20 Data were obtained from three examinations in each subject at baseline (visit 3), week 12 (visit 5), and week 26 (visit 7). The study did not include a placebo arm, as both treatments tested had shown efficacy in placebo-controlled trials.11 ,21 ,22 Salbutamol was used as a rescue drug. Patients receiving inhaled corticosteroids (ICS) at baseline continued treatment (or the ICS component alone if taken as a fixed combination with a bronchodilator) at the same or equivalent dose and regimen. The study was approved by institutional review boards and ethics committees, and was conducted in accordance with the Declaration of Helsinki and the International Conference on Harmonisation Good Clinical Practice guidelines. All patients provided written informed consent before study participation. Additional details are included in the online supplementary data.
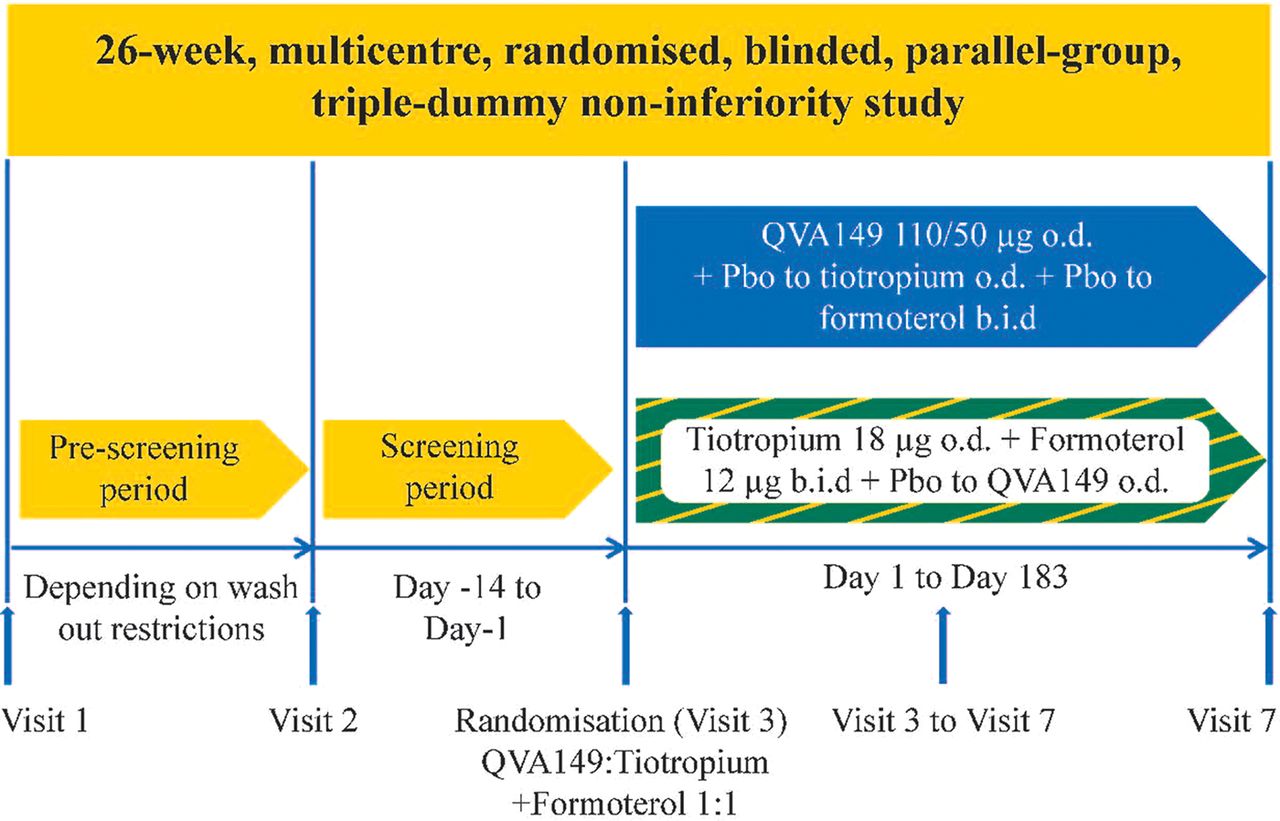
Study design. b.i.d., twice daily; o.d., once daily; Pbo, placebo.
Patients
The study population included men and women aged ≥40 years with moderate-to-severe COPD (GOLD II or III as defined in the GOLD 2010 strategy), current or ex-smokers with a smoking history of at least 10 pack-years, post-bronchodilator forced expiratory volume in 1 s (FEV1) ≥30% and <80% of predicted value, and post-bronchodilator FEV1 to forced vital capacity (FVC) ratio <0.70 at screening. The patient population was similar to those included in other efficacy trials using the TIO and FOR combination.14 ,15 Key exclusion criteria included COPD exacerbation that needed treatment with antibiotics, systemic corticosteroids (oral or intravenous) or hospitalisation in the 6 weeks before pre-screening or between pre-screening and randomisation (visits 1 and 3). Detailed inclusion and exclusion criteria are provided in the online supplementary appendix.
Assessments
HRQoL for eligible patients was measured using SGRQ-C.23 Dyspnoea was assessed using the Transition Dyspnoea Index (TDI), and spirometry (FEV1 and FVC) was done according to American Thoracic Society/ European Respiratory Society standards.24 The primary objective was to demonstrate non-inferiority of QVA149 compared with TIO+FOR combination for HRQoL with respect to the improvement in SGRQ-C. Secondary endpoints included TDI scores, symptoms of SGRQ-C, spirometry (FEV1 and FVC), rate of moderate and severe COPD exacerbations requiring hospitalisation and time to first moderate/severe exacerbation during the treatment period. Moderate exacerbations were those managed with antibiotics and/or systemic corticosteroids; severe exacerbations were those that resulted in hospitalisation. Trough FEV1 measurements were done 45 and 15 min pre-dose (23 h 15 min and 23 h 45 min after the morning dose, respectively). FEV1 30 min measurements were performed 30 min after the morning dose. Study drug compliance was assessed by the study nurse by recording capsule counts.
Adverse events (AEs) and serious AEs (SAEs), including COPD exacerbations and vital signs, were recorded at each visit. ECG and laboratory analyses (haematology, clinical chemistry and urine analysis) were also carried out.
Statistical analysis
The non-inferiority margin was predefined as 4 units, which has been reported in the literature as a sensible definition for the limit for a clinically relevant effect for the SGRQ-C.19 However, this trial was powered to achieve a confidence interval (CI) that allowed excluding even a smaller difference of 3 units. The full analysis set (FAS) was used for the primary efficacy and safety analysis and the per-protocol set (PPS) analysis was conducted as a sensitivity measure. No interim analyses were performed.
The primary analysis was performed using an analysis of covariance model. The model contained treatment, SGRQ-C at baseline and centre as fixed effects. The estimated adjusted treatment difference for QVA149 minus TIO+FOR was displayed together with the associated 95% CI and p value (two-sided). In addition, a one-sided p value for the shifted null hypothesis of inferiority was given. The non-inferiority of QVA149 over TIO+FOR was claimed if the shifted, one-sided p value was <2.5% or, equivalently, if the 95% CI lay entirely to the left (smaller than) of the non-inferiority margin of four points. A true difference of 0 SGRQ-C units and a common standard deviation of 13 were assumed, leading to 396 patients/group to achieve 90% power to reject the null hypothesis of inferiority >3 points for QVA149 versus TIO+FOR. To compensate for drop-out, a minimum of 440 patients per group were to be enrolled into this trial.
Results
Patients
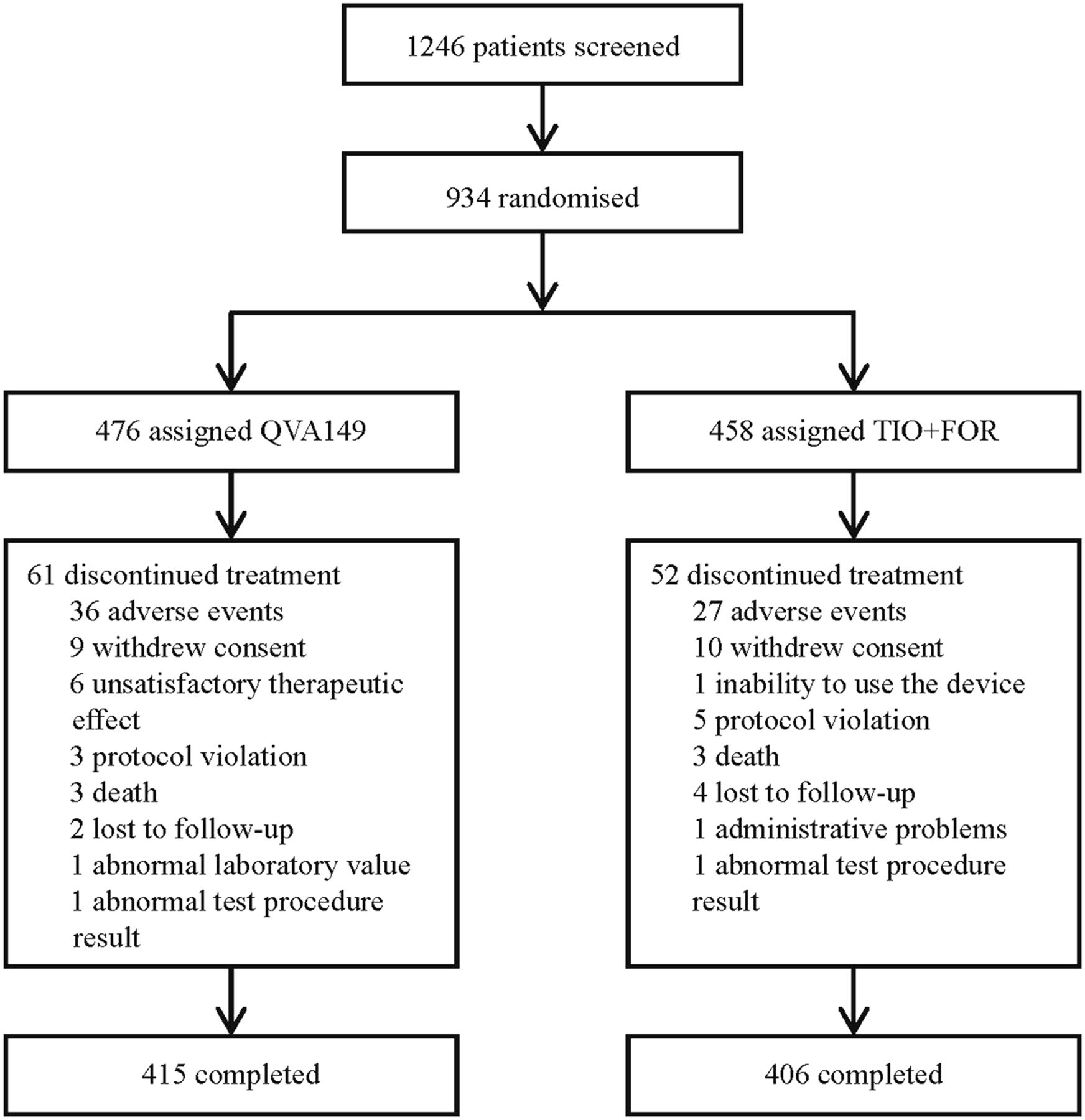
Of the 1246 patients screened, 934 were randomised to QVA149 (N=476) or TIO+FOR (N=458), and 821 (87.9%) patients completed the study (figure 2). Completion and withdrawal rates were similar between the two treatment groups (figure 2). Baseline patient demographics, and other clinical characteristics were numerically comparable across the two treatment groups (table 1).
Baseline demographics and clinical characteristics
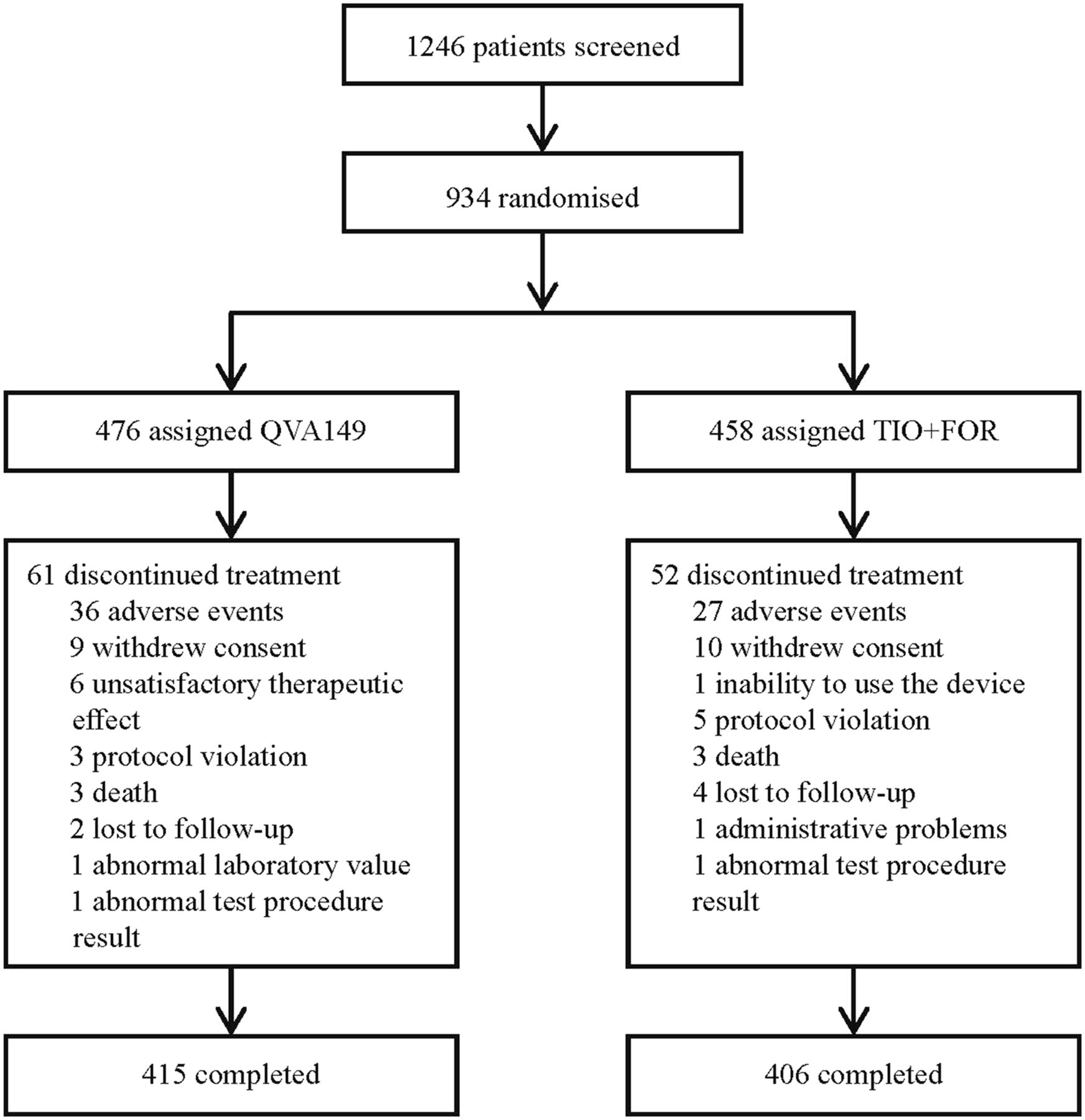
Patient disposition. FOR, formoterol; TIO, tiotropium.
Details on concomitant drugs are provided as online supplementary data.
Efficacy
All the 934 randomised patients were included in the FAS. In the PPS analysis, 747 (80%) patients were included (QVA149: n=373 and TIO+FOR: n=374). Non-inferiority was met (p<0.001; one-sided, shifted test) for QVA149 compared with TIO+FOR as the upper margin of the CI was lower than the predefined non-inferiority margin of 4 units (figure 3). The change from baseline in the SGRQ-C total score (FAS and PPS) was comparable in both groups (figure 4A and see online supplementary figure S1A).
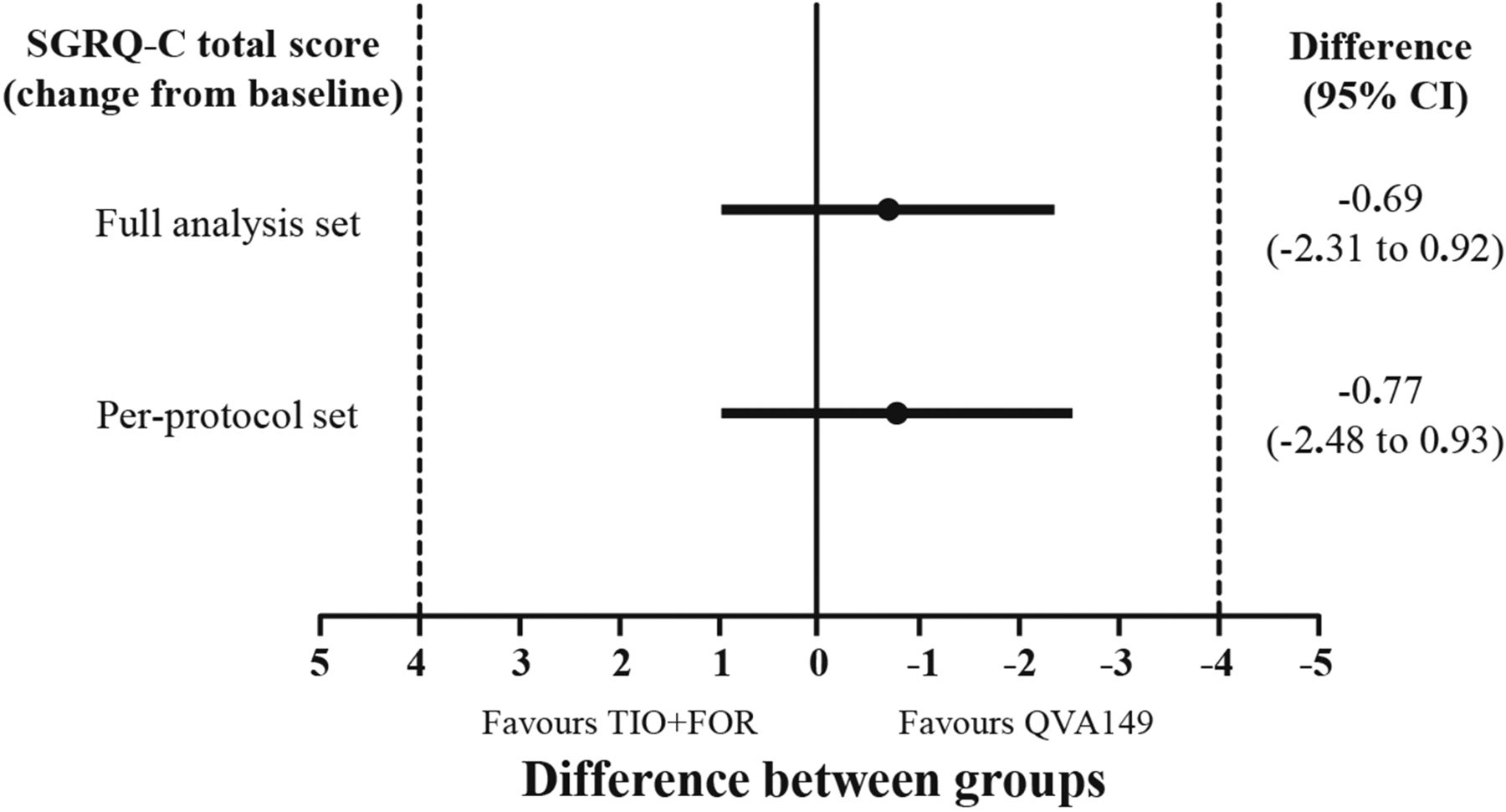
SGRQ-C score at week 26, change from baseline in each treatment group (by FAS and PPS). The non-inferiority margin was –4 to 4 units (shown by dotted line). FAS, full analysis set; FOR, formoterol; PPS, per-protocol set; SGRQ-C, St George's Respiratory Questionnaire for patients with COPD; TIO, tiotropium.

SGRQ-C total score after 26 weeks. (A) LSM change from baseline in SGRQ-C total scores during treatment and (B) percentages of patients achieving the minimum clinically important difference (≥4 units) in SGRQ-C score after 26 weeks (FAS). FOR, formoterol; FAS, full analysis set; LSM, least squares mean; RR, risk ratio; SGRQ-C, St George's Respiratory Questionnaire in patients with COPD; TIO, tiotropium; ns, not significant.
In the FAS, the percentage of patients achieving the minimum clinically important difference (MCID) of 4 units in the SGRQ-C total score25 was similar in the QVA149 and TIO+FOR groups (figure 4B). However, in the PPS, the difference was significantly in favour of QVA149 (p=0.038; see online supplementary figure S1B). Similar improvements in symptom, activity and impact scores of SGRQ-C (see online supplementary table S1) were seen with QVA149 versus TIO+FOR. A subgroup analysis on SGRQ-C based on gender, age group, use of ICS and disease stage (according to GOLD 2010) at week 26 showed no statistically significant influence of the variables (online supplementary table S2).
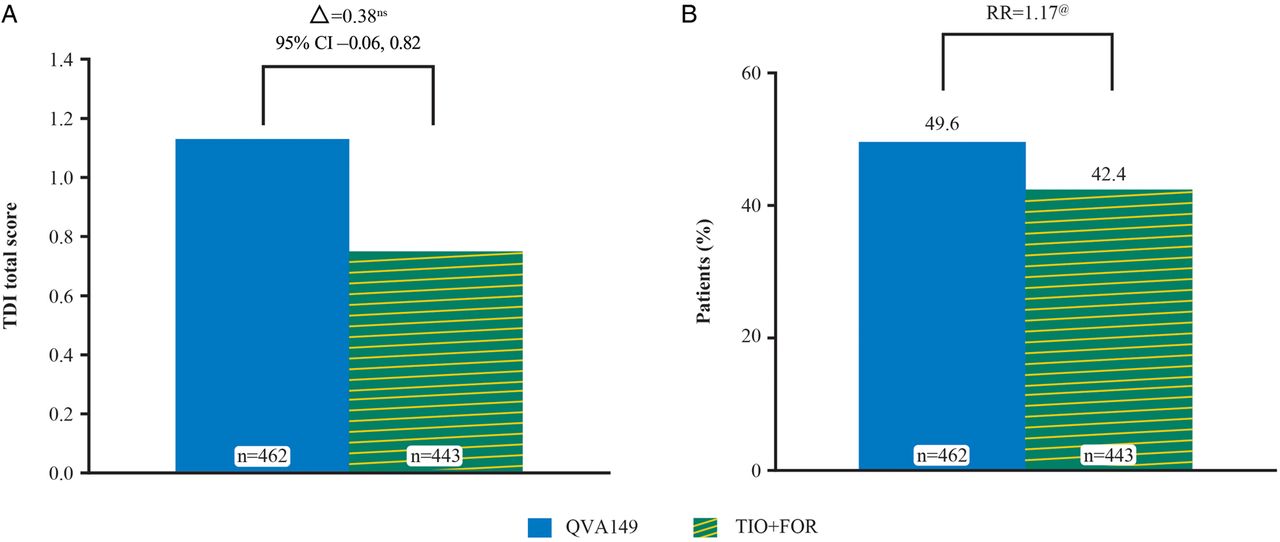
The TDI total score showed similar reduction in dyspnoea with QVA149 and TIO+FOR in the FAS (figure 5A) and PPS (online supplementary figure S2A). Significantly more patients receiving QVA149 achieved the MCID ≥1 unit in dyspnoea26 versus TIO+FOR in the FAS (p=0.033; figure 5B) and PPS (p=0.009; online supplementary figure S2B).

TDI total score. (A) TDI total score (LSM) after 26 weeks and (B) percentages of patients achieving the minimum clinically important difference (≥1 units) (FAS). FOR, formoterol; FAS, full analysis set; LSM, least squares mean; RR, risk ratio; TDI, Transition Dyspnoea Index; TIO, tiotropium. ns, not significant. @p<0.05.
Compared with TIO+FOR, patients receiving QVA149 showed a higher pre-dose FEV1 in the FAS (p<0.001) (figure 6A) and the PPS (p<0.001) (online supplementary table S3). Similarly, improvements in pre-dose FVC values were significantly greater in the QVA149 group than in the TIO+FOR group in the FAS (figure 6B) and PPS (see online supplementary table S3). Post-dose FEV1 and post-dose FVC showed no significant differences between the treatment groups (figure 6A, B and online supplementary table S3).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Lung function at week 12 and week 26 (FAS). (A) Pre-dose and post-dose FEV1 and (B) pre-dose and post-dose FVC. FAS, full analysis set; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity. *p<0.001; #p<0.01; ns, not significant.
The percentage of patients who had at least one moderate or severe exacerbation, and time to first moderate or severe exacerbation, analysed using the Kaplan–Meier method were comparable between the two treatment groups (see online supplementary figure S3 and table S4).
Safety
Overall, the study drug exposure was similar between both groups. The mean±SD duration of exposure was 167.2±44.6 days in the QVA149 group and 169.0±41.0 days in the TIO+FOR group. The average drug compliance was nearly 100% in both treatment groups (mean±SD: QVA149 99.5±8.6, TIO 98.9±11.0 and FOR 97.9±10.8). Table 2 summarises the individual AEs, which were similar in both treatment groups.
Most frequent AEs (excluding COPD exacerbations) in safety set population
Pneumonia occurred at a higher frequency in the TIO+FOR group than in the QVA149 group. The number of AEs leading to study discontinuation was comparable in both groups (table 3).
SAEs, deaths and discontinuation of the study drug
Pneumonia led to premature discontinuation in four patients in the TIO+FOR group, with two patients showing a causal relationship to the study drug. Other AEs leading to study drug discontinuation were cough (n=2 in each group), dyspnoea (QVA149, n=2 and TIO+FOR, n=1), and myocardial infarction (QVA149, n=2). Overall, AEs with a suspected relationship to the study drug were comparable in both treatment groups (table 3).
Overall SAEs and SAEs leading to study discontinuations were comparable in both treatment groups (table 3). Three cases of SAEs in the QVA149 group (one patient each of cerebral ischaemia, tachycardia and an unknown reason leading to death), and one case of SAE (stress cardiomyopathy) in the TIO+FOR group were suspected to be study drug-related.
Overall, three deaths were reported in each group (table 3). In the QVA149 group, the causes of death were myocardial infarction (n=1), pulmonary embolism (n=1) and an unknown reason (n=1). In the TIO+FOR group, the causes of death were acute cardiac failure (n=1), coronary artery disease (n=1) and acute dyspnoea and brain injury (n=1).
Discussion
The QUANTIFY study, for the first time, compared the efficacy of a fixed-dose LABA/LAMA combination (QVA149) with a free-dose combination (TIO+FOR). The combination of TIO and FOR, the standard-of-care LABA and LAMA, respectively, is suggested to be the most widely used free-dose LABA/LAMA combination, hence used as an active comparator in this study. To our knowledge, use of HRQoL as a primary endpoint for comparing active pharmacological interventions for COPD has not been previously evaluated. Moreover, it is well recognised that the effectiveness of COPD treatments should not be assessed by lung function alone.27 This is of particular relevance as the study focused on patient-reported outcomes, which are of key importance, for patients and their physicians and also for health technology assessments.28 The study met its primary endpoint by demonstrating non-inferiority of QVA149 versus TIO+FOR in terms of HRQoL, as assessed by the SGRQ-C. The non-inferiority margin of –4 points is an accepted threshold.19 The study was powered to exclude a difference of –3 units and would have reached non-inferiority even for –1 units. The treatment difference between QVA149 and TIO+FOR indicated a numerical improvement in favour of QVA149. This seemingly small difference, albeit not significant, indicates that more patients receiving QVA149 may achieve clinically relevant improvements in quality of life than those receiving TIO+FOR.19 This was corroborated with a numerically higher percentage of QVA149-treated patients achieving clinically relevant improvement in SGRQ-C25 compared with patients receiving TIO+FOR, which reached statistical significance in the PPS population.
Concomitant drugs did not influence efficacy parameters as the patient baseline characteristics were comparable between treatment groups. Also, the study was undertaken within a close geographical area, so ethnicity and regional factors become negligible. Dyspnoea is the cardinal symptom of COPD and is the major symptom causing patients with COPD to seek medical attention, and also the most relevant burden on patients.1 ,26 Responder rates, which are based on validated response criteria such as MCID, are accepted for comparing active treatments, as the response definition already includes a threshold for relevance.25 ,29 QVA149 demonstrated a statistically significant improvement in TDI responder rates (MCID of ≥1 point improvement) compared with TIO+FOR, which was consistent with the BLAZE and the SHINE studies, with the difference being that these studies used only TIO as an active comparator.3 ,29
Statistically significant improvements in pre-dose FEV1 and FVC were seen in a comparison of QVA149 with TIO+FOR. It is plausible that this bronchodilatory effect might have enabled patients to attain greater levels of activity, and hence improved quality of life.30 ,31 As expected, the treatment difference was not as pronounced for post-dose FEV1 and FVC, as both LABAs (indacaterol and formoterol) are potent bronchodilators with a fast onset of action.32 The simultaneous inhalation of LABA and LAMA from a single device is not the underlying cause, as the effects of QVA149 on lung function are similar to those with the concurrent administration of its monocomponents.18 There was an observed lung function decline in both treatment groups during the study (QVA149 vs TIO+FOR: 49 vs 47 mL in pre-dose FEV1) from week 12 to week 26 which may be potentially due to seasonal aspects as the patients entered this study during summer and the study was concluded in winter.33
Although this study was neither designed nor powered to examine exacerbation rates, fewer patients receiving QVA149 had at least one moderate or severe exacerbation compared with those receiving TIO+FOR. The prevention and reduction of exacerbations might be consequent to improved 24 h bronchodilation34 and potentially contributed to the improvements in SGRQ total score and TDI responders in the QVA149 group as exacerbations are generally associated with worse health outcomes.12 ,35
The beneficial clinical effects of QVA149 versus TIO+FOR treatments are probably a consequence of more potent bronchodilation translating into greater improvements in health status. This view is supported by similar results when single once-daily bronchodilators were compared with drugs with a twice-daily regimen.36 ,37 It is tempting to speculate about other ‘real-life’ benefits of one versus several inhalation(s) a day, which cannot be substantiated in a triple-dummy design, owing to difficulties with different inhalers, complex medication regimens involving multiple drugs and dosing intervals, and the potential to make mistakes.
The incidence and severity of AEs and SAEs were as expected for the patient population in the stage of disease studied, with no clinically relevant differences between the groups. At first instance, the low incidence of typical side effects (eg, dry mouth in the TIO+FOR arm, cough upon inhalation in the QVA149 arm) is surprising. However, this is in line with other QVA149 trials that included tiotropium as comparator. Additionally, the QUANTIFY study recruited many patients with previous exposure to both drugs, who had experienced these side effects and no longer considered them noteworthy.3 ,12 ,29 There were no additional safety concerns for either QVA149 or TIO+FOR. The results were consistent with previous clinical studies.8 ,11 ,12 ,15
There was nearly 100% compliance with treatment in both groups, which is generally expected in a trial. Clinical evidence suggests that adherence to COPD treatment in routine life is strongly correlated with dosing frequency, with once-daily dosing having the highest adherence relative to twice- or thrice-daily dosing.5 Hence, even more pronounced treatment differences can be expected in favour of QVA149 in a real-life setting as patients tend to forget their medication. In addition, QVA149 offers the benefits of dual bronchodilation via a single inhaler device, making it a more convenient option and improving adherence compared with once-daily tiotropium plus twice-daily formoterol inhaled via two different devices.
The study has certain limitations. First, the study only considered the incidence of at least one exacerbation, rather than the number of exacerbations experienced during the study. This was due to the protocol modification during the course of the study, allowing patients with a COPD exacerbation to remain in the study, instead of being withdrawn. Second, because the study was conducted between May and April the following year, seasonal factors might have influenced results. This potential risk was minimised both by randomisation and the large patient population. There was no difference in seasonal exposure to treatment between the two study arms. Third, as most patients in this trial had non-frequent exacerbations, reflecting the real-life situation, effectiveness assessment in patients with frequent exacerbations would be of interest in future trials. Finally, without a placebo arm the possibility cannot be excluded that some of the improvements seen were mainly due to better patient management in a clinical trial. However, in the QUANTIFY study all differences between the two active treatments were in favour of QVA149, strongly supporting a real treatment effect rather than a random placebo effect.
Conclusions
The QUANTIFY study showed that QVA149 is non-inferior to the standard-of-care, free-dose LABA/LAMA combination of tiotropium plus formoterol, for health-related quality of life, with consistent improvement in lung function and dyspnoea. The study supports the premise that QVA149 treatment can be a simpler alternative, suggesting improved patient adherence and compliance. QVA149 has the potential to be more effective than the free combination of TIO+FOR.
Acknowledgments
The authors thank the patients who participated, and the staff at the participating clinical centres. The authors were assisted in the preparation of the manuscript by Vivek Khanna (Novartis). All authors participated in the development and writing of the manuscript and take full responsibility for its content. All authors approved the final draft that was submitted.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors RB and SK contributed to the design of the study. RB, the principal investigator of the study, read and commented on the full study report, and had final responsibility for the decision to submit for publication. CG, WS, KF and SK, investigators of the study, contributed to the writing of each draft of the manuscript. SH and CS, as employees of the sponsor, contributed to the design and preparation, conduct, analysis and interpretation of the study for the manuscript, and also contributed to the writing of each draft of the manuscript.
-
Funding The study was supported and funded by Novartis Pharma GmbH, Germany. Writing support was funded by Novartis Pharma AG, Basel, Switzerland. No restrictions were placed on authors regarding the statements made in the manuscript.
-
Competing interests RB has received reimbursement for attending scientific conferences, and/or fees for speaking and/or consulting from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Grifols, Novartis, Takeda and Roche. SK has served as an advisor to GlaxoSmithKline and received lecture fees from Almirall, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis, Takeda and Grifols. CG has served as an advisor to Boehringer Ingelheim, Chiesi, Novartis and Teva and received lectures fees from Almirall, Boehringer Ingelheim, Chiesi, GlaxoSmithKline and Novartis. KF has received speakers fees from Almirall, Astra Zeneca, Berlin Chemie, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Janssen Cilag, MSD, Mundipharma and Novartis. CS and SH are employees of Novartis Pharma GmbH.
-
Patient consent Obtained.
-
Ethics approval Institutional review boards and ethics committees at participating centres.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves