Article Text

Abstract
Background The incidence of tuberculosis has increased among South African gold miners despite comprehensive control programmes, including a radiological screening programme. No data are available as to the optimal frequency of screening. The aim of this study was to compare 6-monthly and 12-monthly radiological screening for active tuberculosis case-finding.
Methods Employees of a gold mining company were randomly assigned to the control arm (screening at baseline, 12 and 24 months) or the intervention arm (additional ‘intervention’ radiographs at 6 and 18 months after baseline). Study outcomes included proportion of tuberculosis cases detected by screening, proportion smear-positive, extent of disease and mortality.
Results 22 634 miners were randomised. Compared with 12-monthly screening, 6-monthly screening detected more tuberculosis suspects but not more cases, partly due to greater attrition between screening and further investigation after ‘intervention’ compared with routine radiographs. Tuberculosis cases detected in the 6-monthly versus the 12-monthly screening arm had less extensive disease (p=0.05) and a lower tuberculosis-specific mortality (death on tuberculosis treatment) (2.1 and 2.8 per 1000 person-years respectively, HR 0.73, 95% CI 0.50 to 1.08, p=0.1), which was most marked in the first 2 months of treatment (HR 0.48, 95% CI 0.23 to 0.98, p=0.04) when death from tuberculosis is most likely.
Discussion In settings with a high prevalence of HIV and tuberculosis despite standard tuberculosis control measures, more frequent case-finding may reduce the extent of disease, tuberculosis mortality and tuberculosis transmission through earlier detection of active tuberculosis cases. To be effective, however, all tuberculosis suspects identified through screening must be investigated for tuberculosis.
- Tuberculosis
- radiological screening
- active case-finding
- mortality
- randomised
- HIV
- clinical epidemiology
- tuberculosis
Statistics from Altmetric.com
- Tuberculosis
- radiological screening
- active case-finding
- mortality
- randomised
- HIV
- clinical epidemiology
- tuberculosis
Background
The burden of tuberculosis has increased markedly in sub-Saharan Africa, largely due to the HIV epidemic.1 Tuberculosis is the leading cause of death among HIV-infected Africans.2 The DOTS (Directly Observed Therapy, Short course chemotherapy) tuberculosis control strategy has failed to contain tuberculosis rates in countries with a generalised HIV epidemic,3 and additional strategies are required in these settings.4 5
South African gold mines exemplify the problems of controlling tuberculosis in the context of an HIV epidemic. Despite well run tuberculosis control programmes6–9 that include active case-finding using radiological screening as well as passive case-finding and treatment with fixed-dose combination tables taken under direct observation for the entire treatment period, tuberculosis rates among miners rose during the 1990s to over 3000 per 100 000 per year by 1999.8 Silica dust exposure and silicosis are both risk factors for tuberculosis.10–17 Silicosis occurs commonly among gold miners, so that miners now have a high prevalence of two of the most powerful risk factors for developing tuberculosis disease following infection (silicosis and HIV), and their combined effect is multiplicative.16
Radiological screening has been used in the gold mining industry for decades18; both 6- and 12-monthly radiological screening were used in different companies, with no data concerning the most effective screening frequency, particularly in the context of high HIV prevalence. Earlier detection of tuberculosis could reduce tuberculosis-specific morbidity, particularly chronic lung sequelae, mortality and the duration of infectiousness. In support of this, observational studies have demonstrated significantly less extensive radiological disease19 and lower case fatality rates among tuberculosis cases detected by the radiological screening programme compared with those who self-presented with symptoms.7 However, no trial has previously investigated the optimal frequency of active tuberculosis case-finding using radiological screening.
The aim of this trial was to compare the individual level effect of 6-monthly versus 12-monthly radiological screening on the proportion of tuberculosis cases detected by screening, the proportion who were smear-positive, the extent of the disease and mortality.
Methods
Study site, population, randomisation
The trial was conducted at a single gold mining company in Free State Province, South Africa from 1998 to 2002. All miners were routinely screened for tuberculosis using a miniature screening chest radiograph (100 mm×100 mm) during their annual medical examination to determine fitness to work. All mine workers employed on 15 October 1998 were randomised to the 12-monthly (control) or 6-monthly (intervention) radiological screening arm, using each miner's company number and the randomisation function in Microsoft Excel (Microsoft Office 1997). In accordance with routine company practice, individuals in the control arm were scheduled to have three screening radiographs during the 2-year study period (baseline, 12 and 24 months).
Intervention
Individuals in the intervention arm had an ‘intervention’ radiograph 6 months after both the baseline and 12-month routine radiographs. Trained radiographers read both the routine annual and intervention screening miniature radiographs using a viewing screen with an inbuilt magnifying glass. Tuberculosis suspects were identified by radiographs with new or changing abnormalities compared with previous films. The comparison with previous films made it impossible to conceal the randomisation arm. The routine 12-monthly radiographs were taken in the occupational health department and tuberculosis suspects referred to routine health services for assessment the same day. Because in practice it took 15 months for more than 95% of the workforce to undergo routine ‘annual’ radiological screening, follow-up was extended to 30 months to allow most individuals to undergo three routine radiographs. The intervention radiographs were taken in a mobile unit at the mineshaft (to minimise loss of working time) and read the next day; tuberculosis suspects identified by intervention radiographs were notified to primary health clinics which were requested to refer them for further assessment.
Outcomes
More frequent screening was expected to increase the number of tuberculosis cases detected in the short term, precluding tuberculosis incidence as an outcome. The primary outcome measure was the proportion of all tuberculosis cases detected by radiological screening and the proportion of all culture-positive tuberculosis cases who were sputum smear-positive. Secondary outcome measures included the radiological extent of disease, overall mortality and tuberculosis-specific mortality. All-cause mortality was defined as death from any cause during the study period. Tuberculosis-specific mortality was defined as death while on tuberculosis treatment.
Tuberculosis suspects and cases
Tuberculosis suspects were referred to the mine health service for a standard plate chest radiograph and mycobacterial investigations using a standard protocol with three sputum specimens taken over 2 days for fluorescent microscopy, Lowenstein–Jensen culture and identification of Mycobacterium tuberculosis using a colorimetric ribosomal RNA hybridisation test (Accuprobe M tuberculosis complex probe kit, Gen-Probe, San Diego, California, USA).7 8 Tuberculosis episodes captured in the routine health service database between 1 January 1998 and 31 January 2002 were verified against hospital records. Study data were double-entered into a separate database. Employment records were used to identify individuals who had left the study workforce or died.
Method of detection
Based on review of the clinical records, each tuberculosis case was classified as a ‘radiological screening pick-up’ if tuberculosis was diagnosed following investigations initiated within 90 days of the screening radiograph and otherwise as ‘self-presentation’.
Radiological extent of tuberculosis disease
A sequential sample of 190 patients with tuberculosis starting treatment was graded for extent of radiological disease. Standard size chest radiographs before the start of treatment were scored by dividing each lung into three equal zones and allocating a score according to the total number of zones involved. Two readers who were blind to the study arm and method of detection scored the chest radiographs, resolving all disagreement by consensus.
Sample size estimates
Assuming the proportion of all tuberculosis cases detected by radiological screening in the control arm was 49%, to detect an increase to 65% in the intervention arm with 90% power and a type I error of 5% required 211 cases per arm. Given a tuberculosis incidence of 3% per year, this required approximately 7050 person-years (pyrs) per arm. Assuming 85% of culture-positive cases were smear-positive in the control arm, to detect a decrease to 75% in the intervention arm would require 354 cases per arm; assuming an incidence of culture-positive tuberculosis of 2% per year, this required 15 400 pyrs per arm. The workforce was being downsized when the study was planned but, even with a worst case scenario of a reduction to 15 000 employees, randomisation of the entire workforce with follow-up for 2 years was estimated to be adequate. The study was not primarily designed to detect important differences in mortality.
Data analysis
Data were analysed with STATA 10 software (STATA Corporation). The main analysis was based on intention to treat. Individuals were excluded from analysis if the date of enrolment was unknown, they were in the study <30 days or were on treatment for the entire study period.
The proportion of tuberculosis cases detected through radiological screening, the proportion smear-positive among those culture-positive tuberculosis cases and the extent of the disease were compared by study arm using the χ2 test and summarised using the prevalence ratio and 95% CI. The incidence of tuberculosis and the mortality rate were calculated by censoring at the earliest of date of termination of employment, transferred out, end of study (31 January 2002) or first episode of tuberculosis or death, respectively. Differences in all-cause mortality between study arms were analysed using Cox regression; a secondary analysis of tuberculosis-specific mortality was conducted, restricted to deaths while on tuberculosis treatment and the first 2 months of tuberculosis treatment when the cause of death is most likely due to tuberculosis rather than other causes.7
The analysis of primary and secondary outcomes was restricted to the first episode of tuberculosis occurring during the study period. The evaluation of the process of being identified as a tuberculosis suspect, investigated for tuberculosis and starting tuberculosis treatment included tuberculosis suspects investigated more than once during the study period.
Results
Study population
A total of 22 634 miners were randomised, of whom 622 (2.7%) were excluded from analysis (figure 1) leaving 11 015 and 10 997 miners in the 12-monthly and 6-monthly screening arms, respectively. The two study arms were identical with respect to median age (39 years), the proportion working underground (89%) and duration of follow-up (24 months); 406 miners (3.7%) declined the intervention radiograph. Approximately two-thirds of miners in each study arm had a baseline and two annual screening radiographs during the study period and 92% (n=10 143) of miners in the 6-monthly arm had at least one intervention chest radiograph (figure 1). Most of the losses to follow-up in each arm were due to termination of employment (figure 1). Overall follow-up for the 12-monthly and 6-monthly study arms were 20 858 and 20 777 pyrs, respectively, and the median person time at risk was 2.02 years for both arms.

Study flow chart. *On tuberculosis (TB) treatment for multidrug-resistant tuberculosis for the entire study period.
Tuberculosis cases
During the study period a total of 1302 miners had one or more episodes of tuberculosis identified, 632 in the 12-monthly screening arm and 670 in the 6-monthly screening arm. Forty-two individuals (3.2%) had a second tuberculosis episode during the study period.
Outcomes
The intervention had no effect on the primary outcome (table 1). The proportion detected through radiological screening by the 12-monthly and 6-monthly screening arms was similar (28.3% (179/632) vs 29.4% (197/670), prevalence ratio 1.04, 95% CI 0.88 to 1.23, p=0.67). The proportion of sputum culture-positive patients who were smear-positive did not differ between the 12-monthly and 6-monthly screening arms (84.1% and 85.6% respectively, prevalence ratio 1.02, 95% CI 0.96 to 1.08, p=0.56).
Summary of outcomes by study arm
Pulmonary tuberculosis cases occurring in the 12-monthly screening arm had more extensive radiological disease at diagnosis than those in the 6-monthly screening arm (39.3% (33/84) vs 29.2% (31/106) with ≥4 zones involved, p=0.05). The all-cause and tuberculosis-specific mortality rates (per 1000 pyrs) are shown in table 1. There was a non-significant reduction in all-cause mortality in the 6-monthly screening arm compared with the 12-monthly screening arm (mortality rate 11.7 vs 12.6, HR 0.92, 95% CI 0.78 to 1.10). There was a reduction in tuberculosis-specific mortality in the 6-monthly arm compared with the 12-monthly screening arm (mortality rate 2.1 vs 2.8, HR 0.73, 95% CI 0.50 to 1.08, p=0.1), which was more marked when the analysis was restricted to deaths within the first 2 months of tuberculosis treatment (mortality rate 0.52 vs 1.1, HR 0.48, 95% CI 0.23 to 0.98, p=0.04). As expected, tuberculosis incidence (per 1000 pyrs) did not differ by study arm (12-monthly: 30.3, 6-monthly: 32.2, incidence rate ratio 1.06, 95% CI 0.95 to 1.18, p=0.3).
In order to understand these results, we documented in detail the process of being identified as a tuberculosis suspect, investigated for tuberculosis and starting tuberculosis treatment by study arm. All tuberculosis suspects, including those investigated for tuberculosis more than once during the study period, were evaluated (table 2). More tuberculosis suspects were identified in the 6-monthly screening arm than in the 12-monthly screening arm (13.0% (1433/10 997) vs 10.4% (1145/11 015), p<0.0001). However, when summarised as tuberculosis suspects per chest radiograph, the percentage was higher in the 12-monthly screening arm than in the 6-monthly screening arm (6.4% vs 4.1%, p<0.0001). The investigation of tuberculosis suspects differed by study arm, with fewer suspects being investigated for tuberculosis in the 6-monthly screening arm than in the 12-monthly screening arm (37% vs 42.8%, p=0.003). Of those suspects investigated for tuberculosis, a similar proportion in both arms were treated for tuberculosis and confirmed as ‘radiological screening pick-ups’ on clinical review.
Comparison of tuberculosis suspects* identified by radiographic screening, investigated and treated for tuberculosis
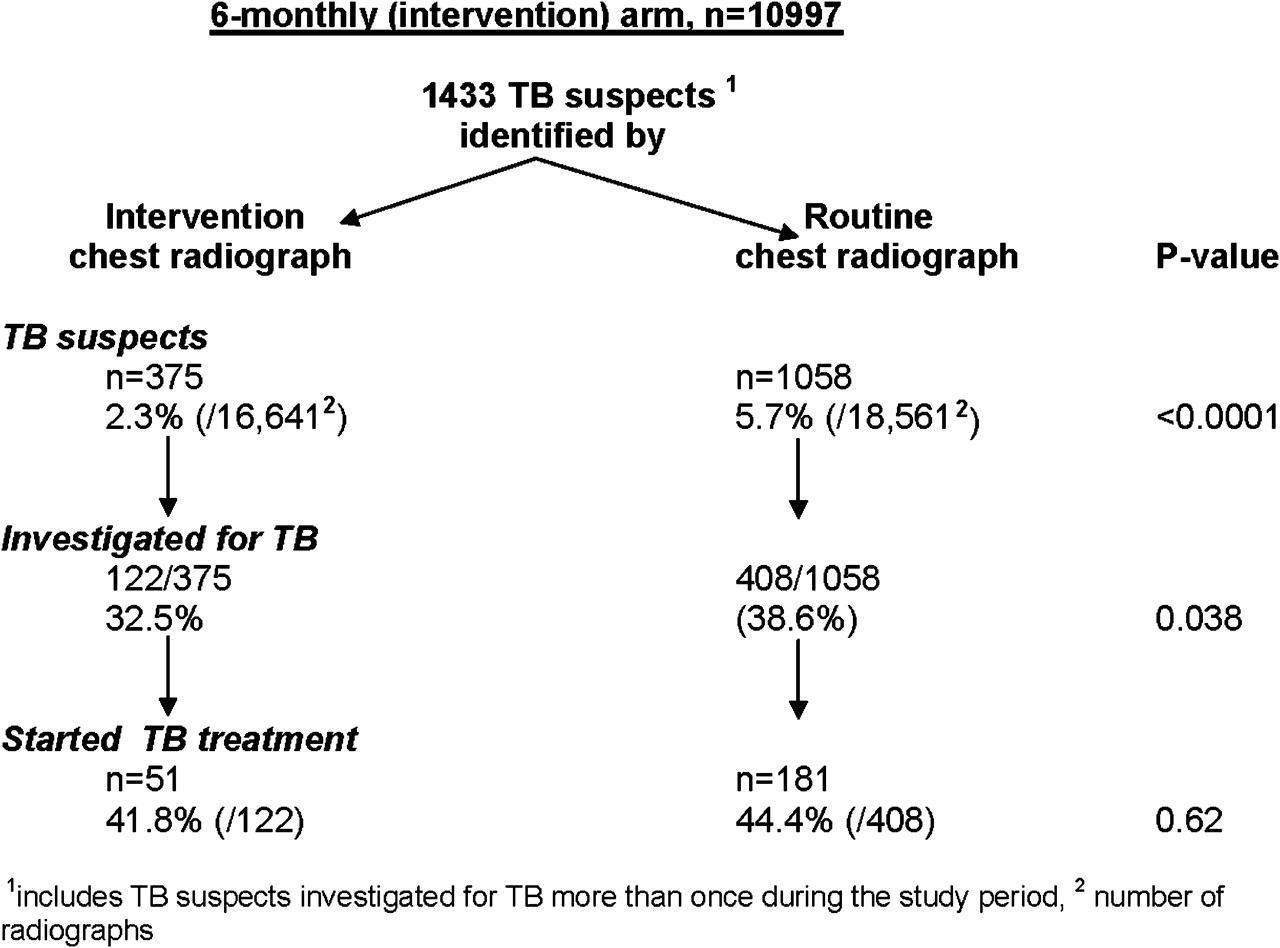
We also compared the investigation of tuberculosis suspects, including those investigated for tuberculosis more than once during the study period, identified by intervention or routine chest radiographs within the 6-monthly screening arm (figure 2). Intervention radiographs generated a smaller proportion of tuberculosis suspects than did routine screening radiographs (2.3% (375/16 641) vs 5.7% (1058/18 561), p<0.0001]). There was substantial attrition between being identified as a tuberculosis suspect by either type of screening radiograph and further investigations for tuberculosis, which was slightly worse after intervention radiographs than after routine screening radiographs (intervention: 32.5% (122/375), routine: 38.6% (408/1058), p=0.038) However, once investigated, the proportion of tuberculosis suspects treated for tuberculosis did not differ between the routine and intervention chest screening radiographs (intervention: 41.8% (51/122), routine: 44.4% (181/408), p=0.62). These unanticipated differences resulted in a similar proportion of tuberculosis cases being detected by radiological screening in the 12-monthly and 6-monthly screening arms (12-monthly: 28.3% (179/632), 6-monthly: 29.4% (197/679); table 1).

{kind=link}
{kind=link}
Comparison of tuberculosis suspects identified by intervention or routine chest radiographs in the 6-monthly screening arm.
Discussion
This large individually-randomised trial found that almost one-third of tuberculosis cases in the 12-monthly screening arm were detected by the routine radiological screening programme. Six-monthly radiological screening detected more tuberculosis suspects than 12-monthly screening, but this did not translate into more tuberculosis cases being put on treatment. However, tuberculosis cases detected in the 6-monthly screening arm compared with the 12-monthly screening arm had less extensive disease and a trend towards lower tuberculosis-specific mortality (death on tuberculosis treatment), which was greatest within the first 2 months of treatment when death from tuberculosis is most likely.
The apparent lack of effect of 6-monthly radiographic screening to detect more cases of tuberculosis than 12-monthly screening was unexpected but can be explained by the differences in the routine and intervention radiographic screening procedures. It is possible that intervention radiographs were either of lower quality or less carefully read than routine films, resulting in fewer tuberculosis suspects being identified. Furthermore, the substantial attrition between identification of tuberculosis suspects and further investigation will have reduced the effectiveness of screening in both arms, but more so in the intervention arm because attrition of tuberculosis suspects after intervention radiographs was significantly higher. The large proportion of suspects not investigated for tuberculosis may be due to poor referral systems because of logistical or communication barriers, or miners opting out of further investigations as they had no or minimal symptoms or because of fears of job security. The differences in the routine and intervention radiographic screening procedures may also explain why the proportion of sputum culture-positive patients who were smear-positive did not differ between the 12-monthly and 6-monthly screening arms. Another possible explanation is that the prevalence of undiagnosed tuberculosis 6 months after the last chest radiograph was lower than after 12 months and therefore the intervention chest radiographs would detect a lower proportion of undiagnosed tuberculosis.
Additional studies in the same workforce provide further insight into why 6-monthly compared with 12-monthly radiological screening may not have detected additional tuberculosis cases. HIV-associated tuberculosis disease differs in a number of respects from tuberculosis disease in HIV-negative persons, including the pace at which symptoms develop and progress. A study comparing the incidence of tuberculosis and point prevalence rates of undiagnosed tuberculosis in this workforce has indicated that HIV-infected patients with tuberculosis present with symptoms much more rapidly than do non-HIV-infected patients.20 As the prevalence of HIV increased among patients with tuberculosis over time, so did the proportion of patients with tuberculosis detected by self-presentation to the health service.8 Thus, it may be that the 6-month interval tested in this study was still too long to substantially increase the proportion of HIV-infected patients with tuberculosis being detected by radiological screening. In addition, radiological screening alone has a relatively low sensitivity for detecting active tuberculosis disease in this workforce.21 This may be because the 12-monthly screening programme has already reduced the prevalence of chronic active tuberculosis that is radiologically detectable to relatively low levels, since radiology consistently detects the majority of prevalent undiagnosed tuberculosis disease in previously unscreened populations. It is therefore possible that adding a different screening test such as sputum culture would have been more effective than increasing the frequency of the existing radiological screening programme.21
Cause of death while on tuberculosis treatment was not established but it is known from other studies that most deaths during the first few months of tuberculosis treatment are due to tuberculosis, unlike deaths occurring later in the course of treatment.7 The trend towards a reduced tuberculosis-specific mortality, particularly when restricted to deaths within the first 2 months of treatment, suggests a survival benefit from earlier detection of tuberculosis cases in the more intensive screening arm, an interpretation that is supported by our finding of less extensive radiological disease among tuberculosis cases in the 6-monthly screening arm.
A limitation of the study was the individually randomised design and the inability to determine the impact of the intervention on overall tuberculosis prevalence or incidence (because any beneficial impact from a reduction in tuberculosis transmission would be equally distributed across the study arms). Further studies of tuberculosis case-finding using cluster randomised designs are therefore required to evaluate the impact of enhanced and active case-finding strategies on tuberculosis control in settings with endemic tuberculosis and high prevalence of HIV.
How generalisable are the results of this study? Active radiological tuberculosis case-finding reduces the prevalence of undiagnosed tuberculosis by detecting symptomatic cases missed by the health service and by detecting infectious tuberculosis cases with asymptomatic or minimally symptomatic disease that has not prompted presentation to the health service or are below the threshold of detection by the health service. Although the mines may have better quality health services that are better able to detect symptomatic tuberculosis cases than many public sector health services in resource-poor countries, earlier detection of asymptomatic or minimally symptomatic tuberculosis cases through active radiological screening that are not detectable by the health services would be generalisable to other settings, including those with poor passive case-finding.
Strengthening tuberculosis control programmes to meet WHO targets for case-finding and cure under DOTS remains a high priority. However, in settings with endemic or epidemic tuberculosis and a high HIV prevalence, the results of this study suggest that enhancing existing case-finding activities or introducing active case-finding campaigns may reduce the extent of the disease and tuberculosis mortality and potentially reduce tuberculosis transmission through earlier detection of active tuberculosis cases. In the mines, 6-monthly radiological active case-finding should be implemented if shown to be cost-effective, in addition to scaling up isoniazid preventive therapy targeted to miners with HIV and silicosis. In order for active case-finding to be effective, however, tuberculosis suspects identified through screening must be investigated for tuberculosis and treated if confirmed.
Acknowledgments
The authors thank the staff of Aurum Institute for Health Research and Ernest Oppenheimer Hospital, particularly those from the Occupational Health Centre, laboratory and radiology departments and the tuberculosis clinic, for their assistance in conducting this study. Dr Daan Mulder, University of the Netherlands, provided invaluable assistance in developing the study protocol. Tragically, Dr Daan Mulder died shortly after the study started.
References
Footnotes
Funding This study was funded by the Safety In Mines Research Advisory Council of South Africa (SIMHEALTH Gen 524). GJC and KF were funded by Aurum Institute for Health Research. ELC was funded by a Wellcome Trust Training Fellowship in Clinical Tropical Medicine. ADG was supported by a UK Department of Health Public Health Career Scientist award. GJC and KF are funded by the Consortium to Respond Effectively to the AIDS TB Epidemic.
Competing interests GJC was employed by AngloGold Health Services during the conduct of the study. None of the other authors has competing interests.
Ethics approval The study was approved by the research ethics committees of Anglogold Health Services and the London School of Hygiene and Tropical Medicine, and through the Mine Health and Safety Committees of each mine shaft with the involvement of union representatives. Individual informed consent for the intervention chest radiographs was not obtained as radiological screening is a legal requirement in the industry and the optimal frequency of radiological screening is unknown and both were used. Individuals had the option to undergo or to decline the intervention chest radiograph.
Provenance and peer review Not commissioned; externally peer reviewed.