Article Text

Abstract
Background: Laser acupuncture, a painless technique, is a widely used alternative treatment method for childhood asthma, although its efficacy has not been proved in controlled clinical studies.
Methods: A double blind, placebo controlled, crossover study was performed to investigate the possible protective effect of a single laser acupuncture treatment on cold dry air hyperventilation induced bronchoconstriction in 44 children and adolescents of mean age 11.9 years (range 7.5–16.7) with exercise induced asthma. Laser acupuncture was performed on real and placebo points in random order on two consecutive days. Lung function was measured before laser acupuncture, immediately after laser acupuncture (just before cold dry air challenge (CACh)), and 3 and 15 minutes after CACh. CACh consisted of a 4 minute isocapnic hyperventilation of –10°C absolute dry air.
Results: Comparison of real acupuncture with placebo acupuncture showed no significant differences in the mean maximum CACh induced decrease in forced expiratory volume in 1 second (27.2 (18.2)% v 23.8 (16.2)%) and maximal expiratory flow at 25% remaining vital capacity (51.6 (20.8)% v 44.4 (22.3)%).
Conclusions: A single laser acupuncture treatment offers no protection against exercise induced bronchoconstriction in paediatric and adolescent patients.
- laser acupuncture
- asthma
- children
- CACh, cold dry air challenge
- EIB, exercise induced bronchoconstriction
- EIA, exercise induced asthma
- FEV1, forced expiratory volume in 1 second
- MEF25, maximal expiratory flow at 25% remaining vital capacity
Statistics from Altmetric.com
- CACh, cold dry air challenge
- EIB, exercise induced bronchoconstriction
- EIA, exercise induced asthma
- FEV1, forced expiratory volume in 1 second
- MEF25, maximal expiratory flow at 25% remaining vital capacity
Needle acupuncture has been used in the treatment of various complaints for thousands of years in China and in the last decades it has become very popular in Western countries.1 Laser acupuncture, a painless technique, is commonly practised in the treatment of paediatric patients.
Exercise induced bronchoconstriction (EIB) is a common clinical manifestation of bronchial asthma occurring in 40–90% of paediatric patients.2, 3 The main mechanism leading to EIB is exercise induced hyperventilation.4–6 Hyperventilation causes evaporative water loss from the airways, and the resulting increase in osmolarity of the airway surface liquid is thought to lead to regulatory volume changes of airway epithelial cells.7 This might trigger the release of various bronchoconstrictive mediators from the reactive mucosal cell systems.8
There are few studies of the acute effect of acupuncture on EIB in patients with asthma.9–11 The results of two studies on needle acupuncture treatment were contradictory.9, 10 Only one study has investigated the effect of laser acupuncture in adult patients with exercise induced asthma (EIA) and it was unable to show any effect on EIB.11 To date, laser acupuncture has not been studied in paediatric patients with EIA.
We have performed a double blind, placebo controlled, crossover study to investigate the possible protective effect of a single laser acupuncture treatment on hyperventilation induced bronchoconstriction in paediatric and adolescent patients. Cold dry air hyperventilation was used as a surrogate for exercise provocation to standardise the trigger stimulus and to avoid noise from variations in climatic conditions and exercise intensity.
METHODS
Subjects
Forty four patients (18 girls and 26 boys) of mean (SD) age 11.9 (2.6) years (range 7.5–16.7) with mild to moderately severe bronchial asthma participated in the study. All subjects were recruited from the outpatient clinic of the local paediatric respiratory centre and had to fulfil the following criteria: (1) a diagnosis of bronchial asthma based on clinical criteria,12 (2) a history of EIA, (3) a positive bronchial reaction (decrease in forced expiratory volume in 1 second (FEV1) of 9% or more to cold dry air challenge (CACh)),13 (4) the presence of atopy indicated by a positive skin prick test (mean weal ≥3 mm at 15 minutes) to one or several of 16 common inhalant allergens, and (5) no symptoms of a respiratory infection for 4 weeks before the study. Long term anti-asthma treatment consisted of inhaled budesonide (n=19), fluticasone (n=18), nedocromil (n=5), or disodium cromoglycate (n=2) which were withheld for 24 hours before the study and bronchodilator medication was withheld for 12 hours.
Laser acupuncture
Laser acupuncture was performed by a qualified physician who had been trained in this technique by the Austrian Society for Controlled Acupuncture. Acupuncture was performed at six sites commonly used in the treatment of asthma.14, 15 The points chosen for real acupuncture consisted of Yintang (Ex-1), Chize (Lu-5), Lieque (Lu-7), Feishu (UB-13), Geshu (UB-17), and Shanzhong (CV-17). Acupuncture points that were not relevant for the patients' complaints were selected for placebo treatment. These placebo points were Baihui (GV-20), Quze (Pe-3), Neiguan (Pe-6), Dashu (UB-11), Weishu (UB-21), and Zhongwan (CV-12).
Laser acupuncture was performed using a soft laser (Modulas-Handy 2, Schwa-medico, Ehringshausen, Germany) with output of 22.5 mW ±10%, 830 nm wavelength, and laser beam of 1 mm diameter. Each acupuncture point was stimulated for 60 seconds. To obtain the maximum effect the stimulation was repeated after a 12 minute interval. The applied dose of energy per acupuncture point amounted to 3.6 J/cm2. The same technique was used in both real and placebo acupuncture.
Lung function and bronchial responsiveness
Pulmonary function tests were performed in accordance with standardised guidelines.16 Forced expiratory vital capacity was recorded in form of a volume-time and a flow-volume curve on a pneumotachograph spirometer (MasterLab Pro; Jaeger, Wuerzburg, Germany). FEV1 and maximal expiratory flow at 25% remaining vital capacity (MEF25) were measured from these curves and the results were expressed as percentage of predicted normal based on relevant reference standards.17 Pulmonary function tests were performed as baseline measurements immediately after laser acupuncture treatment—that is, just before CACh and 3 minutes and 15 minutes after CACh.
CACh was performed in accordance with an established protocol13, 18, 19 which consisted of isocapnic hyperventilation of absolute dry air at –10°C air for 4 minutes at 75% of maximal voluntary ventilation. Cold dry air was produced by a commercially available heat exchanger (RHES; Jaeger, Wuerzburg, Germany).
The changes in FEV1 (ΔFEV1) and in MEF25 (ΔMEF25) before and after CACh were expressed as percentage baseline. Airway hyperresponsiveness was defined by a CACh induced fall in FEV1 of 9% or more.13, 19
Visual analogue scale
Respiratory symptoms were assessed immediately before each lung function measurement using a 100 mm visual analogue scale (VAS) with the words “minimum” on the left end and “maximum” on the right end. Subjects were instructed that “minimum” meant “no complaints such as shortness of breath, chest tightness, and breathlessness” and that “maximum” stood for “the worst complaints of respiratory sensations imaginable”. The distance in mm from “minimum” was used in calculations.
Study protocol
Real and placebo acupuncture were performed in random order on two consecutive days between 13.00 and 15.00 hours. To maintain the double blind nature of the study neither the patient nor the laboratory technician performing CACh knew which kind of acupuncture had been used.
Informed consent was obtained from both the patients and their parents, and the study was approved by the ethics committee of the Medical Faculty, University of Graz.
Statistical methods
A power calculation based on previous data on CACh responses of children with asthma13 indicated that a minimum of 39 patients was needed to detect a clinically relevant effect of acupuncture with a power of 80%. Data were expressed as mean (SD). Differences between groups and within groups were analysed by one way analysis of variance (ANOVA). Data in contingency tables were analysed by the χ2 test. A p value of ≤0.05 was taken as the limit of statistical significance.
RESULTS
Effect of laser acupuncture on lung function and bronchial responsiveness
Pulmonary function test results at baseline, after acupuncture, and 3 and 15 minutes after CACh are presented in table 1 and illustrated in fig 1. Baseline measurements did not differ between real and placebo acupuncture, and mean FEV1 and MEF25 values after acupuncture remained unchanged from baseline values. CACh caused a statistically significant decrease in FEV1 and MEF25 at 3 and 15 minutes for both acupuncture regimens.
Mean (SD) results of pulmonary function tests at baseline, after acupuncture, and after cold dry air challenge (CACh)
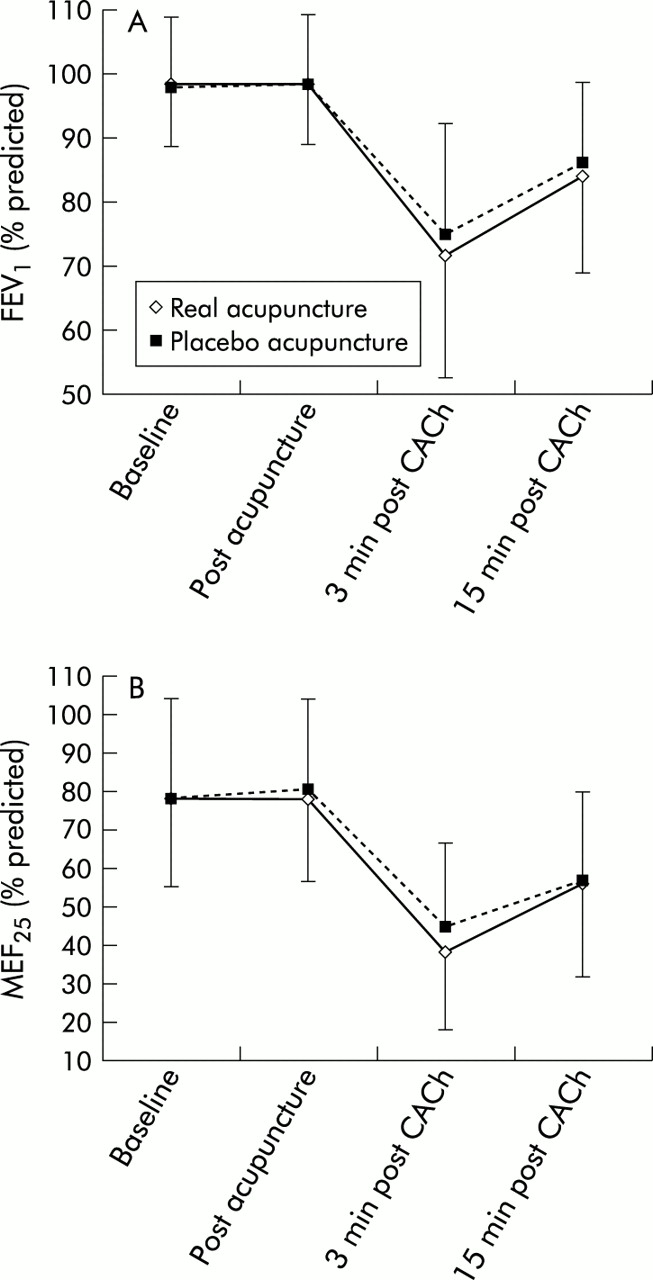
Mean (SD) baseline, post acupuncture and post challenge values of (A) FEV1 and (B) MEF25 (% predicted) for real and placebo acupuncture.
The cross sectional statistical comparison of measurements revealed no significant differences between values after acupuncture and between values 3 and 15 minutes after CACh, although post CACh values were slightly higher after placebo acupuncture than after real acupuncture.
The CACh induced changes in FEV1 and MEF25 are summarised in table 2. Although decreases in FEV1 and MEF25 were somewhat higher after real acupuncture than after placebo acupuncture, the differences did not reach statistical significance at 3 or 15 minutes.
Mean (SD) changes in pulmonary function after cold dry air challenge (CACh)
A normal response to CACh was found in only four of the 44 patients (9%) after real acupuncture and in eight (18%) after placebo acupuncture (p=NS). Thirty two children (73%) remained hyperreactive after both acupuncture regimes.
Effect of laser acupuncture on subjective assessment (VAS)
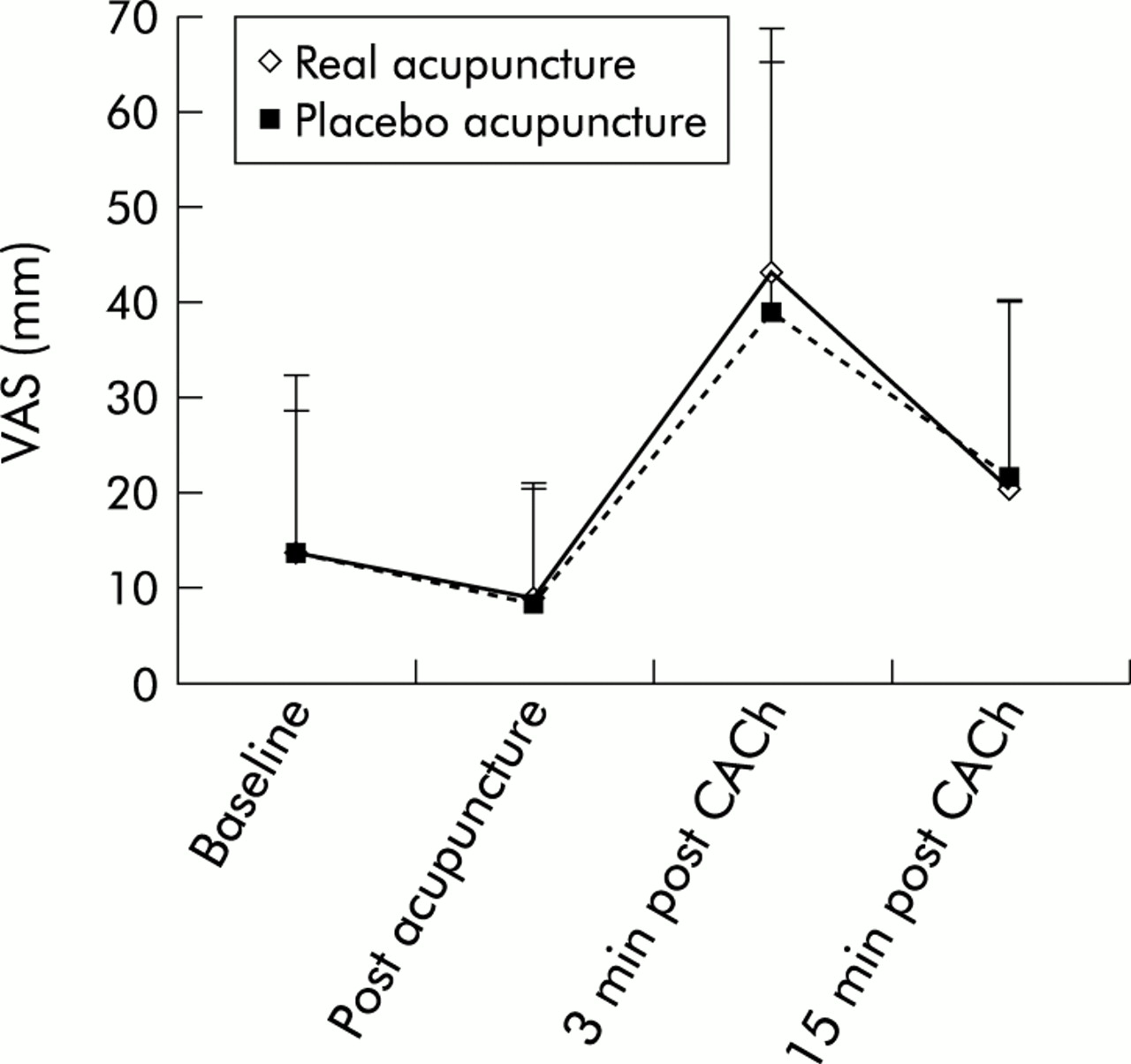
VAS measurements at baseline, after acupuncture, and 3 and 15 minutes after CACh are shown in fig 2. CACh caused a statistically significant increase in VAS values 3 minutes after CACh for both acupuncture and placebo treatment (p<0.001). Fifteen minutes after CACh the VAS values had improved; for placebo there was still a marginally significant difference (p=0.047) compared with the values after acupuncture. Differences between real and placebo acupuncture did not reach statistical significance at any time.
{kind=link}
{kind=link}
Mean (SD) baseline, post acupuncture and post challenge visual analogue scale (VAS) scores in mm for real and placebo acupuncture.
DISCUSSION
Objective and subjective measurements of this study show that a single laser acupuncture treatment on asthma points does not influence the basal bronchomotor tone, and offers no protection against cold dry air hyperventilation induced bronchoconstriction in paediatric and adolescent patients with EIA.
We failed to demonstrate any bronchodilating effect of laser acupuncture. This finding is in agreement with the outcome of two clinical trials that could not show any decrease in the basal bronchomotor tone after needle acupuncture on auricular or body points.9, 10
To date, only one study has examined the effect of laser acupuncture in bronchial asthma.11 This investigation in a small group of adult women with EIA found that a single laser acupuncture treatment administered before exercise did not prevent EIB. Similarly, our results suggest that a single laser acupuncture treatment of children and adolescents with EIA is ineffective in the prevention of EIB.
Two other studies have evaluated the possible influence of needle acupuncture on EIB in children with asthma.9, 10 One reported a significant attenuation of EIB after real (body) acupuncture and placebo (body) acupuncture in comparison with no treatment, with real acupuncture providing more protection than placebo acupuncture.10 The other study, however, found no protection against EIB after real (auricular) acupuncture.9
From these results one could conclude that laser acupuncture is less effective than other acupuncture methods. This hypothesis is suppored by studies in pain research and gastroenterology comparing laser acupuncture with needle acupuncture and/or electroacupuncture in which efficacy could be demonstrated for needle acupuncture and electroacupuncture only while laser acupuncture failed to show any effect.20, 21
The acupuncture protocol used in this study could also explain the lack of therapeutic efficacy. All patients were treated with the laser at the same acupuncture points. This so called formula acupuncture, which is the form of acupuncture practised in Western countries, implies that patients with the same (Western) diagnosis share a pathology which is sufficiently similar to be treated at the same acupuncture points. In traditional Chinese medicine a special kind of diagnosis based on constitutional factors (Chinese anamnesis) and pulse and tongue diagnosis leads to individually tailored acupuncture treatment.22 The underlying concept is that every patient is unique and consequently must be treated individually. Because the selection and number of acupuncture points differ from patient to patient, however, the effect of treatment cannot be compared and therefore traditional acupuncture cannot be used in controlled clinical trials.
We can speculate that repeated acupuncture treatments for several weeks or months may be required to obtain a beneficial effect on EIB. As with topical steroids,23 acupuncture might effect a protection against EIB that develops over several weeks. This hypothesis is supported by a report of increased corticosteroid production after acupuncture treatment.24 No long term studies of the influence of any form of acupuncture treatment on EIB have so far been performed. Some long term trials have investigated the effect of repeated needle acupuncture treatment on asthma symptoms, medication use, and various lung function parameters25–28 with contradictory results.
The different outcome of controlled clinical trials of real versus placebo acupuncture in bronchial asthma raises the question of whether acupuncture in general has a place in the treatment of this disease. Kleijnen et al29 reviewed studies of acupuncture in bronchial asthma and scored the scientific quality of their methodology. They concluded that there are no studies of high quality and that any claims for the efficacy of acupuncture in asthma treatment are not supported by adequately designed clinical trials. A further meta-analysis concluded that it is impossible to make any recommendations about the value of acupuncture in the treatment of asthma on the basis of the current literature.30
In conclusion, the results of the present study indicate that a single laser acupuncture treatment does not influence bronchomotor tone and does not attenuate EIB in paediatric and adolescent patients with asthma. Further research is required to define the possible role of acupuncture in the treatment of bronchial asthma.
Acknowledgments
The authors acknowledge the help of Dr A Berghold with statistical issues in this study.